
Abstract
Objectives:
The study aims to prospectively assess two patient groups receiving standard care and structured training and counseling (STC), in which sleeve gastrectomy (SG) was implemented, in terms of depression, body image, and quality of life.
Methods:
This pretest–posttest, repeated-measures, randomized control prospective study was carried out between March 2017 and May 2018 using an experimental design. Of the participants who underwent laparoscopic SG, 26 patients (control) received standard care and 25 patients (intervention) received STC starting before the operation and lasting for 6 months after the operation.
Results:
The mean age of the patients was 37.1 ± 11.3 years, and 78.4% of them were females and 68.6% were married. The depression scores of the intervention group 6 months after the operation were found to be significantly lower than the control group, whereas the scores of body image and the quality of life were significantly higher (p < 0.05).
Conclusion:
The results supported that the STC program for bariatric surgery was an effective program.
Introduction
Obesity is a health problem that has reached an epidemic scale today. It is reported that 1.9 billion adults are overweight across the world, 650 million of whom are obese. 1 It was stated that the rate of obesity (body mass index [BMI, calculated as kg/m2] ≥ 30) was around 30%, and morbid obesity (BMI ≥40) was around 3% in Turkey in 2009. 2 The prevalence of obesity has increased ∼2.0 times in the last 10 years independent of population growth and age. 3 Obesity, which adversely affects every organ in the body, brings about numerous medical, psychological, social, environmental, and economic problems. Therefore, individuals whose functional status and quality of life has been affected in a negative way start to look for treatments to get rid of obesity. In the treatment of obesity, primarily conservative (diet, exercise, and, behavioral changes) and medical treatments are recommended, and surgical operations might be carried out in cases in which no results have been achieved. 4
Depression is one of the psychopathological conditions caused by obesity. The incidence of depression is higher among patients who look for treatment for obesity.5,6 It was reported that the severity of depression was at the same level as the patients who were hospitalized in psychiatric clinics for psychotherapy. 7 There are conflicting results in the literature as to the influence of bariatric surgery on depressive conditions of patients. In studies in which short- and long-term patient follow-ups were performed, it was reported that depression declined markedly following bariatric surgery8–10 ; however, there are other studies stating that the presurgery rates of the use of depression medication did not change following the surgery 11 and that suicide rates increased. 12 Another significant point related to depression and obesity surgery is that depression negatively affects weight loss or in contrast minor weight loss triggers depression. Various studies show that high depression scores before surgery negatively affects the amount of weight loss after the surgery.13,14 In contrast to this, it was also reported that no significant differences existed between patients who used antidepressants before and after the surgery and those who did not have depression before the surgery. 15
Another important topic related to obesity is body image. Body image disorder in obesity is different from body image disorders developing in anorexia nervosa and bulimia nervosa due to an unrealistic body perception. In obesity, problems related to body perception occur due to discomfort that an individual experiences because of the body shape not approved by the society. Therefore, the concept of “body dissatisfaction (BD)” is more commonly observed in obesity. 16 Studies in which short- and long-term follow-ups were performed report that a decline in BD following the surgery is associated with the duration after the operation and the weight lost.17,18 However, there are various other studies reporting that BD persists due to hanging skin occurring because of excessive weight loss.19,20
No methodological studies were encountered in the Turkish literature investigating the impact of structured training and counseling (STC) on body image and depression in bariatric surgery patient groups during the period in which this study was carried out. These two concepts were studied as dependent variables in line with studies in the international literature indicating that the most significant psychological impact is on body image and depression in bariatric surgery patient groups. Thus, possible problems related to body image can be prevented by informing patients about the problems they might experience about their body image in the short- and long-term after the surgery and possible precautions against these problems, and by having discussions with the patients about the reality of the body image they imagine to have after the surgery. Moreover, STC is required to assess the depression status of patients in preoperative period to achieve the desired outcome from surgery, to carry out psychological monitoring in terms of the possibility of depression in postoperative period, and to develop self-esteem.
The quality of life, which is a subjective concept, is also one of the significant criteria in the assessment of obesity surgery. In meta-analyses and systematic reviews investigating the effect of surgical operation on the quality of life, the common view is that there are improvements in the quality of life in both physical and mental aspects, but mental improvements slow down as time progresses.21,22 While the physical area of the quality of life is mostly associated with energy, muscle power, and endurance, the mental area is related to psychological and social areas. One important point is to support the patients physically, psychologically, and socially so that they adapt to their new lifestyles.
The study was carried out to prospectively assess two patient groups receiving standard care and STC, in which sleeve gastrectomy (SG) was implemented, in terms of depression, body image, and quality of life. It was assumed that the group receiving STC would have better scores of body image, depression, and the quality of life than the group that received standard care.
Methods
Study design
This prospective study was carried out on patients who were to undergo SG operation between March 2017 and May 2018 in the general surgery clinic of the application and research center of a university in Turkey using a randomized control, pretest–posttest, repeated-measures experimental model. When the patients apply to the clinic, they take certain tests (measurement of their body composition, blood parameters, endoscopy, and abdominal ultrasonography) following the physician's examination within the scope of preoperative preparations and receive psychiatric and endocrinological consultation to decide for operation, and then, the decision for operation is made by the council. The study included volunteer patients aged older than 18 years with a BMI of 40 and over who did not have any communication obstacles and who could be communicated via Turkish, who had not undergone bariatric surgical operation before, who would undergo SG operation for the first time, and who would be operated by the same surgeon using the same technique. The patients who met the study criteria were divided into intervention and control groups through simple randomization. The control group received standard care given in the center. The intervention group was given STC (nutrition, physical activity, lifestyle changes) starting before the operation and lasting for 6 months after the operation.
Ethical consent
The ethical permission for the study was obtained from the Non-Invasive Ethics Committee of Düzce University (Dated: June 27, 2016, Consent No: 2016/67), and written consent was taken from the participants.
Sample size and randomization
The sample size was calculated using G-Power software for Windows (version 3.1.9.2) and two-sample t-test power analysis tables for clinical trials. For power analysis, the study by Baştürk in 2015, 23 in which results of SG in Turkey were investigated, was taken as reference. Anticipating a 10% difference between the BMI values of the intervention and control groups at month 6, it was determined that the sample group had to include at least 42 patients (intervention = 21, control = 21) with 80% power (p < 0.05). It was planned to include 30 patients in the groups, thinking that there might be individuals who would abandon the study for any reason. However, as there was no endocrinology specialist who would approve obesity surgery in the center at the time when the study began, an endocrinology specialist working at the state hospital in the same city provided consultation to patients of obesity surgery once a week and gave approval for operations. Since this negatively affected the number of operations and patient applications, the intervention and control groups were limited to 27 persons, thinking that the aimed sample size could not be reached. In the course of the study, one patient could not be contacted (n = 1) and two patients did not attend controls (n = 2); therefore, the study was completed with a total of 51 patients: 26 patients in the intervention group and 25 patients in the control group (Fig. 1). During the randomization, the groups were determined by assigning the first patient who was included in the study as of the start of the study to the intervention group and the second patient to the control group.

Sample flow diagram. n = sample.
Assessments
The sociodemographic characteristics, health status, obesity histories, and dietary habits of the patients were collected through Patient Information Forms prepared by the researcher. The height of the patients was measured without shoes by using stadiometer, and their weight was measured using a body analysis device (Tanita, BC418 model). Excess weight loss was calculated using the formula (initial BMI − final BMI)/(initial BMI −25) × 100 based on the weight and height measured during the examination.
The Beck Depression Scale (BDS) was used to assess the presence and level of depression. The Turkish validity and reliability study of the BDS, which was developed by Beck and Ward 24 in 1961, was performed by Kapci et al. 25 in 2008. The scale consists of 21 items and examines how individuals have felt in the last 1 week. Each item has four options ranging from 0 to 3 points. Depression score is calculated by adding the responses given to all the items and the highest possible score is 63. High total scores indicate high levels of depression. Also, psychiatric consultation was performed for the patients before making a decision for operation, and the depression status of the patients was assessed. The results were found to be consistent with the BDS.
To assess body image, the Body Cathexis Scale (BCS) was used in the study, which was developed by Secord and Jourard 26 in 1953 and adapted to the Turkish society in 1986 by Hovardaoğlu by studying its validity and reliability. 27 The test, implemented to obtain individuals' opinions on the characteristics of body, consists of 40 items that can be scored between 1 and 5 points, and the total score that might be obtained varies between 40 and 200. It is concluded that as the total score gets higher, satisfaction with body image increases.
In the assessment of the quality of life, the Life Quality Short Form (SF-36) was used, which was developed by Ware in 1987 and whose validity and reliability study was carried out by Pınar 28 in 1995. The scale, consisting of 36 items, is made up of 2 main dimensions that evaluate 8 concepts of health. The concepts of physical functioning, role strength-physical, energy/vitality, somatic pain, and general health perception constitute the physical component, whereas the concepts of social functioning, role strength-emotional, mental health, energy/vitality, and general health perception form the mental components. The scale has a Likert-type scoring, and the score of each subdimension and two main dimensions in the scale varies between 0 and 100. It is concluded that as the score of the health area increases, quality of life related to health increases. 28
In the study, the data as to body composition were measured three times, before the operation (T0), 3 months after the operation (T1), and 6 months after the operation (T3). The other data were collected twice, before the operation (T0) and 6 months after the operation (T2). The patients were given information as to how to complete data collection forms and they were allocated enough time to complete the forms. The researcher provided necessary clarifications in cases when the patients could not understand a specific point. It took about 15 min to measure the patients and interpret the results and about 30 min to complete the forms.
Interventions
Standard care
The patients included in the control group were subjected to the standard practices of the center where the study was carried out. There are no special training programs for obesity surgery patients in the center. When patients apply to the polyclinic, first the surgeon evaluates their body composition and then explains the tests to be performed before the operation during the preparation phase to the patients. Information to be given to the patient about the operation technique and risks according to the operation planned is provided by the surgeon orally in line with the informed consent. When the patients are being discharged, they are given a printed list of standard diet and it is advised that they have at least 30-min daily physical activity. However, no extensive training and counseling unique to individuals is offered. The patients are prescribed vitamin and mineral supplements and medical nutrition supplements following the operation. They are called for medical control at day 10, month 1, 3, and 6 after the operation. However, there are no follow-up/registration systems for the patients.
Structured training and counseling
While establishing STC, the program was carried out in the form of individual counseling since there was no common time in which the patients could gather together. To allow for group interactions, it was considered to enable the patients to interact through social media. However, this practice was removed from STC as some patients could not use social media tools. Training materials unique to the visual and auditory area were prepared before the implementation in line with individual STC. A training book consisting of 12 chapters was prepared in line with the literature such as to cover the preoperative, intraoperative, and postoperative periods. A computer presentation (PowerPoint) was prepared simultaneously with the book. Videos were shot in a professional studio, and video CDs (optical disks) were prepared in digital environment. The suitability of the program and data collection tools was assessed by 10 specialists (3 clinic surgeons, 1 psychiatrist, 2 dieticians, and 5 nursing professors). These specialists approved the suitability of the program content. However, they agreed that eight sessions that were initially planned were too long and the program was rearranged as six sessions. The program that was revised on four bariatric surgery patients was pre-applied. After the pre-application, no changes were made in the program. The patients on whom pre-application was carried out were excluded from the study.
STC started 15 days before the operation and continued till month 6 after the operation under the guidance of the prepared training book. In addition to a total of six individual training sessions, twice before the operation (15 days and 1 day before) and four times after the operation (10 days, 1, 3, and 6 months after), the patients were able to communicate with the researcher via phone when the patients needed help. Moreover, they had the opportunity to repeat the trainings by means of the training book and video CDs given to them.
STC was established on two main themes. The first part included general topics related to obesity, obesity surgery, information that will facilitate adaptation to surgery in the preoperative, intraoperative, and postoperative periods, nutrition suitable to bariatric surgery, physical activity, and developing lifestyle changes. The second part focused on depression management, coping with stress without getting food, adaptation to changes in body image, enhancing motivation, and the importance of social support. Each session lasted ∼30 min.
Data analysis
The SPSS Windows 21.0 (Statistical Package for the Social Sciences, Düzce University) was used in data assessment. The results were accepted statistically significant at the level of p < 0.05. Continuous variables were denoted with mean ± standard deviation, and categorical variables with number and percentage. The normality of data distribution was assessed using the Kolmogorov–Smirnov test. The homogeneity of the groups in terms of sociodemographic characteristics was compared via chi-square and the Mann–Whitney U test. The intragroup temporal changes of depression, body image, and quality-of-life scores were analyzed using the Wilcoxon signed-rank test, and the intergroup changes were analyzed using the Mann–Whitney U test. The intragroup temporal changes of anthropometric measurement values were analyzed with the Friedman test, whereas the intergroup changes were analyzed using the Mann–Whitney U test.
Results
The mean age of 51 patients included in the study, who underwent laparoscopic SG, was 37.1 ± 11.3 years (intervention group = 25, control group = 26). Of the sample, 78.4% were female, 64.7% had an educational level of high school and above, 68.6% were married, and 54.9% were unemployed. One or more chronic diseases existed in 47.1% of the patients. The demographic, socio-economic, and anthropometric characteristics of the intervention and control groups were not different and the groups were homogeneous (Table 1).
Comparison of Demographic, Socio-economic, and Anthropometric Findings of the Groups
p-Value is considered significant at <0.05 and is two-sided for comparison between study groups.
BMI, body mass index; SD, standard deviation.
No significant difference was found between the intervention group (16.6 ± 9.2) and the control group (15.7 ± 5.9) in terms of BDS before the operation (p > 0.05). The mean BDS scores of the intervention and control groups were affected positively by temporal changes (p < 0.05). In the intergroup comparison, it was observed that the mean follow-up score of the intervention group from the BDS at month 6 was significantly lower than the control group (p < 0.05). The mean BDS score was 119.2 ± 17.8 in the intervention group and 114.5 ± 23.7 in the control group before the operation, and there were no significant differences between two groups. The mean BCS scores of both groups were affected positively by temporal changes (p < 0.05). However, in the intergroup comparison, the mean follow-up score from the BCS at month 6 was significantly higher in the group that received STC than the group that did not (p < 0.05) (Table 2).
Comparison of the Beck Depression Scale and Body Cathexis Scale Scores of the Intervention and Control Groups
p-Value is considered significant at <0.05 and is two-sided for comparison between study groups.
BCS, Body Cathexis Scale; BDS, Beck Depression Scale.
Table 3 presents the change in quality-of-life scores of the intervention and control groups before and 6 months after the operation. No significant difference was detected between the mean scores of both groups obtained from all the areas of quality of life (p > 0.05). It was seen that the mean scores of all the areas of quality of life increased at month 6 follow-up of the intervention group (p < 0.05), whereas the mean scores that the control group obtained from the other areas of quality of life increased significantly (p < 0.05) except for mental health (p > 0.05). In the intergroup comparison, it was observed that the mean scores of the intervention group from physical functioning, vitality, mental health, general health perception, and physical and mental component were significantly higher than the control group at month 6 follow-up (p < 0.05). There was no significant difference between the mean scores of the groups in the areas of role strength, emotional role strength, social functioning, and pain at month 6 follow-up after the operation (p > 0.05).
Comparison of SF-36 Scores of the Intervention and Control Groups
p-Value is considered significant at <0.05 and is two-sided for comparison between study groups.
The mean preoperative scores for the BMI were 44.3 ± 4.6 in the intervention group and 46.7 ± 5.8 in the control group, with no significant difference (p > 0.05). The mean BMI score at month 3 and 6 after the operation was 35.7 ± 3.8 and 30.6 ± 3.72 for the intervention group and 38.8 ± 6.2 and 34.4 ± 6.5 for the control group, respectively. The temporal change of the mean BMI scores of both groups was statistically significant (p < 0.05). In the intergroup comparison, the mean BMI score of the intervention group at month 6 follow-up was significantly lower compared with the control group (p < 0.05) (Fig. 2). The mean excess weight loss at month 3 and 6 follow-ups after the operation was 45.6 ± 8.1 and 73.3 ± 15.6 for the intervention group and 38.7 ± 13.8 and 60.2 ± 20.7 for the control group, respectively. In the intergroup comparisons, the mean excess weight loss of the intervention group at both month 3 and 6 was found to be significantly higher than the control group (p < 0.05) (Fig. 3).
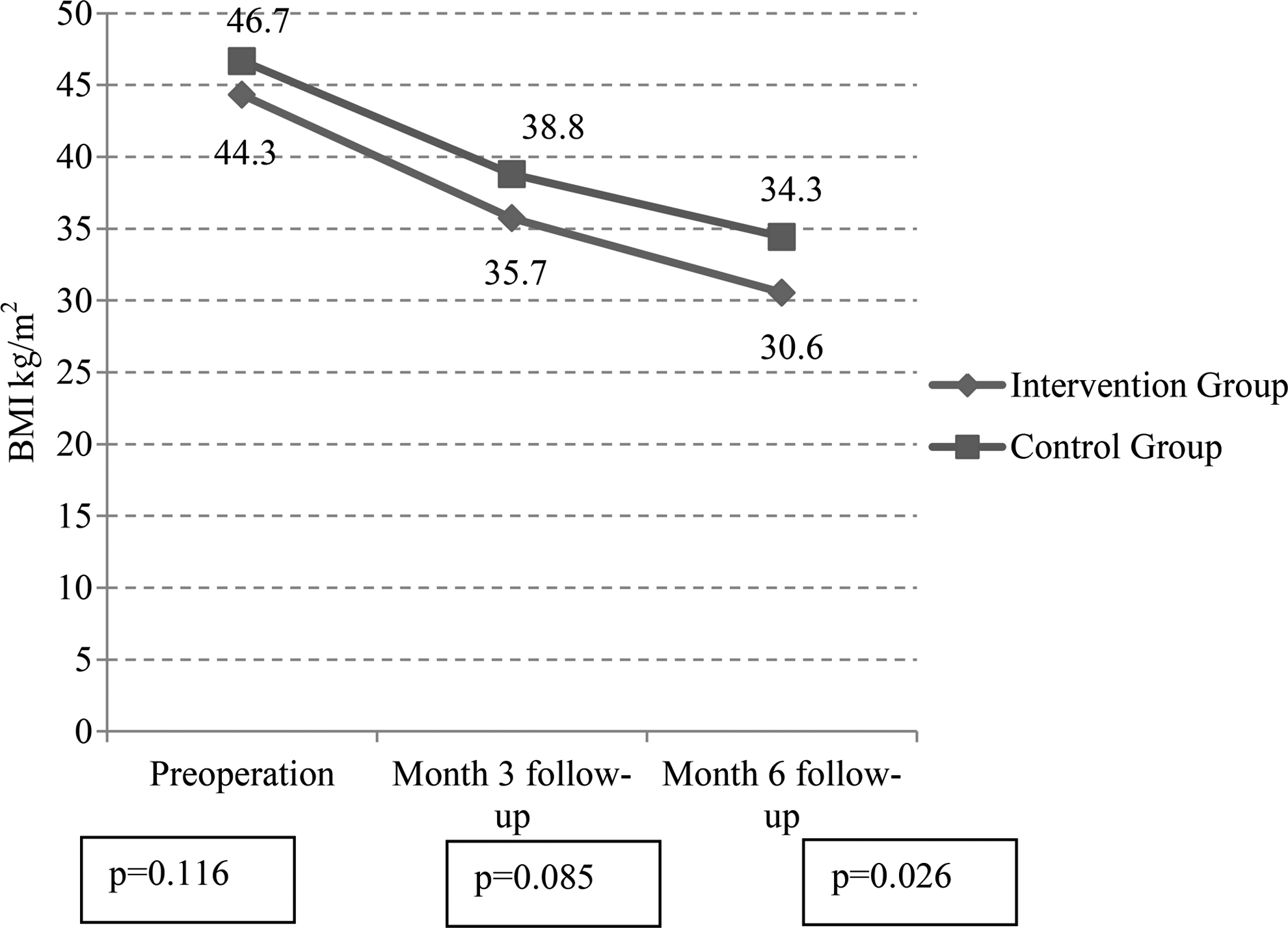
Comparison of the BMIs of intervention and control groups. p = significant. BMI, body mass index [calculated as weight (kg)/height (m) 2 ].

Comparison of the EWL of intervention and control groups. p = significant. EWL, excess weight loss [calculated as (initial BMI − final BMI)/(initial BMI −25) × 100].
Discussion
Today, surgical treatment is used extensively in the treatment of obesity, which causes medical, psychological, social, environmental, and economic problems. It is observed that patients for whom surgical treatment is planned are more disadvantageous due to their attitudes and behaviors toward eating, levels of adaptation to diet and exercise, impaired physical health, and psychopathological conditions. It is advised that a “structured training program” be implemented so that the patients can adapt to the anatomical change in their bodies, shape their lifestyles in line with this, be affected by negative factors the least, and increase their success level.29–32 Based on this, our study prospectively compared the impact of standard care and STC on depression, quality of life, and body image in patient groups in which laparoscopic SG was implemented.
Patients included in STC showed great enthusiasm to participate in the program. They stated that the most significant factor supporting this was the sense of trust that they could always reach the researcher. It was concluded through these statements that the process of information via telephone significantly increased the impact of STC. Starting the program in the preoperative period strengthened the bond between the researcher and the patients and minimized their anxiety, thus supporting their motivations to participate in the program. It is not known how social interaction will affect STC as no interactions were made in social media platforms in the program. The patients were mostly interested in topics related to operation techniques in the sessions in the preoperative period. The sessions held in the first postoperative month dealt with the management of depression due to limited nourishment, whereas those in the third month focused on physical activity. In the 3–6 months of the program, the focus was on anxiety about body image as weight loss increased.
The study results showed that extensive training and counseling starting before and continuing after the operation positively affected depression, body image, and quality of life among patients. Moreover, the intervention group experienced more weight loss in the first postoperative 6 months than the control group.
In this study, the depression scores of both the intervention and control groups were above the normal limits, which support previous studies.5,7 Positive changes in the depression levels of the intervention group following STC are similar to the results of studies in which group training or cognitive behavioral therapy programs are implemented after the operation.33,34 It is considered that the intervention group was positively affected by practical behavior-changing recommendations presented in relation to coping with stress without food in the scope of STC.
According to the study results, the body image satisfaction scores of both the intervention and control groups were low, which means that the patients included in the study suffered from BD. There are studies in the literature showing that BD decreases in relation to the postoperative weight loss.17,18 Moreover, some studies indicate that body image can be negatively affected by hanging excess skin due to rapid weight loss.19,20 One of the key points in rapid weight loss is preventing muscle loss through regular physical activity to minimize hanging skin. It can be concluded that body image was positively affected in the intervention group as the patients were directed to regular physical activity during the program.
Short-term effects of obesity surgery on quality of life are improvements in both mental and physical areas.18,21,22 In the study, the physical and mental areas of quality of life improved in both the intervention and control groups. However, it is noteworthy that the recovery in the intervention group was higher than the control group. Quality of life, which is a multidimensional concept, is closely related to depression, anxiety, and body image.7,17,18 Higher weight loss and positive changes in depression and body image in the group that received STC could have affected the change in quality of life.
It was determined that weight loss was significantly higher in the group that received STC in the first postoperative 6 months than the control group. The amount of weight loss varies based on the type of the operation carried out in bariatric surgery.35–37 To prevent discrepancies emerging from the operation technique, the sampling was performed on the patients operated by the same surgeon using the same technique. The results of this study have parallels with other studies in which similar programs were carried out. However, the long-term effects of the training could not be revealed as the patients were only followed-up for the first 6 months after the operation.
Conclusion
The STC conducted for this study contributed to excess weight loss as well as positive changes in depression, quality of life, and body image of bariatric surgery patients. It is necessary to consider obesity surgery as a process because its consequences can be obtained in the long-term. Programs should be implemented to facilitate adaptation to this process starting from the preoperative and continuing in the postoperative period. Making a contract with the patient before the program can enable active participation. Programs should not only have instructive content but also aim to achieve a permanent change in lifestyle, determine problems, and produce alternative solutions to these problems. Interactive programs should be presented in the form of individual and group trainings and supported by means such as telephone or the Internet. It is recommended to plan accredited programs for which cost analysis has been performed and randomized control studies in which lengthened observations can be made.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a grant from Sakarya University, Sakarya, Turkey (Grant No: 2016-40-02-009).