
Abstract
Background:
The aim of this review was to determine the optimal exercise program to prevent weight gain and maintain weight loss in patients after undergoing bariatric surgery.
Materials and Methods:
We conducted a systematic review in accordance with the PRISMA guidelines. We systematically investigated exercise training studies performed after bariatric surgery published from 2008 through 2018. Studies reporting changes in body composition, muscular strengths, aerobic capacity, functional capacity, walking distance, or relevant health outcomes were included. The review protocol is available from PROSPERO (CRD42018110174).
Results:
Seven articles were included in the review. The included studies reported data on 255 patients. The duration of intervention was between 4 and 26 weeks. The frequency of the session was two to five times per week and each session was ∼30–80 min. Three studies used aerobic exercise for the intervention group, two studies planned resistance training, one study used an outpatient physiotherapy program that included breathing, strengthening, and stretching exercises, and one study used a combination of endurance and strengthening exercises.
Conclusions:
Gradually increasing low–moderate-intensity exercise, and a combination of aerobic, strength, and stretching-type exercise should be planned comprising a minimum 150–300 min per week in postoperative bariatric surgery patients to prevent weight gain and maintain weight loss.
Introduction
Obesity is a problem that is experienced around the world, which brings with it many diseases, such as diabetes, dyslipidemia, hypertension, cancer, and cardiovascular diseases,1–3 and is associated with significantly higher all-cause mortality. 4 Therefore, it is very important to decide the most appropriate treatment method in the treatment of obesity.
Bariatric surgery has become an accepted method in the treatment of obesity in recent years because it helps in the treatment of diseases that develop secondary to obesity. 5 Changes in hormones of the gut and the associated calorie reduction are some of the ways through which weight is lost after bariatric surgery. 6 This surgery results in significant weight loss and has positive effects on diabetes in many patients. 7 Although bariatric surgery is the most commonly used method and the long-term effects of obesity treatment are well known,8,9 weight loss after surgery is difficult to maintain and weight gain might even occur.10–12
Exercise programs after bariatric surgery are recommended for patients because of the benefits in preventing weight regain and maintaining weight loss.13,14 Thus, exercise after bariatric surgery is an important step for treatment. However, there is no clear exercise program that has been determined in terms of intensity, frequency, or duration for patients after bariatric surgery.
The aim of this review was to determine the optimal exercise program to prevent weight gain and maintain weight loss for patients who have undergone bariatric surgery.
Materials and Methods
Literature search
This review was planned to investigate and determine the optimal exercise program for patients who have undergone bariatric surgery. We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. In this systematic review, PubMed (NLM), Pedro, and the Web of Science databases were searched for articles published from January 2008 through September 2018. Search terms included the following: [(bariatric surgery OR gastric bypass OR gastroplasty OR jejunoileal bypass OR lypectomy) and (rehabilitation OR exercise therapy)]. The search terms were determined using the MeSH browser. Searches were restricted to articles published in the English language and included randomized controlled trials. A total of 1552 articles were found.
Interest outcomes
Studies were reviewed for the following outcomes of interest: weight loss and body composition (7 included), muscular strength (3 included), functional capacity (3 included), aerobic capacity (1), and walking distance (4 included).
Inclusion criteria
The inclusion criteria for review were as follows; an exercise therapy program should be included after bariatric surgery, the exercise therapy program should be defined, patients should be 18–65 years of age, the efficacy of the exercise program should be measured by appropriate methods, study length should be more than 4 weeks, include both preoperative and postoperative data collection, studies must be randomized controlled trial and published in English, and multimodal programs with exercise components should be included.
Exclusion criteria
The exclusion criteria were as follows: studies with a sample size of less than 10 and PEDro scale less than 4 points.
Quality of studies
The full text of the articles was evaluated using a standardized article screener by two of the researchers. Disagreements between the two authors were resolved by discussion and by consultation with all authors of the review until consensus was reached. The methodologic quality of all studies was independently assessed by the reviewer using the PEDro scale, which consists of 11 criteria, with a maximum score of 10 (range 0–10); the first item (the specification of the eligibility criteria) is not included in the total score. For rating the methodologic quality, the following classification was used: a PEDro score of 4 indicated poor methodologic quality, a score of 4–5 indicated fair quality, a score of 6–8 was good quality, and a score of 9–10 indicated excellent quality. 15
Results
One thousand five hundred fifty-two articles that matched the search criteria were found in the initial literature search. The abstracts of these publications were screened and 44 that met the inclusion criteria were obtained in full. Thirty-seven articles were then excluded for reasons stated in the PRISMA flowchart (Fig. 1) and seven articles were included in the final review. This process, including reasons for exclusion, is detailed in Figure 1.
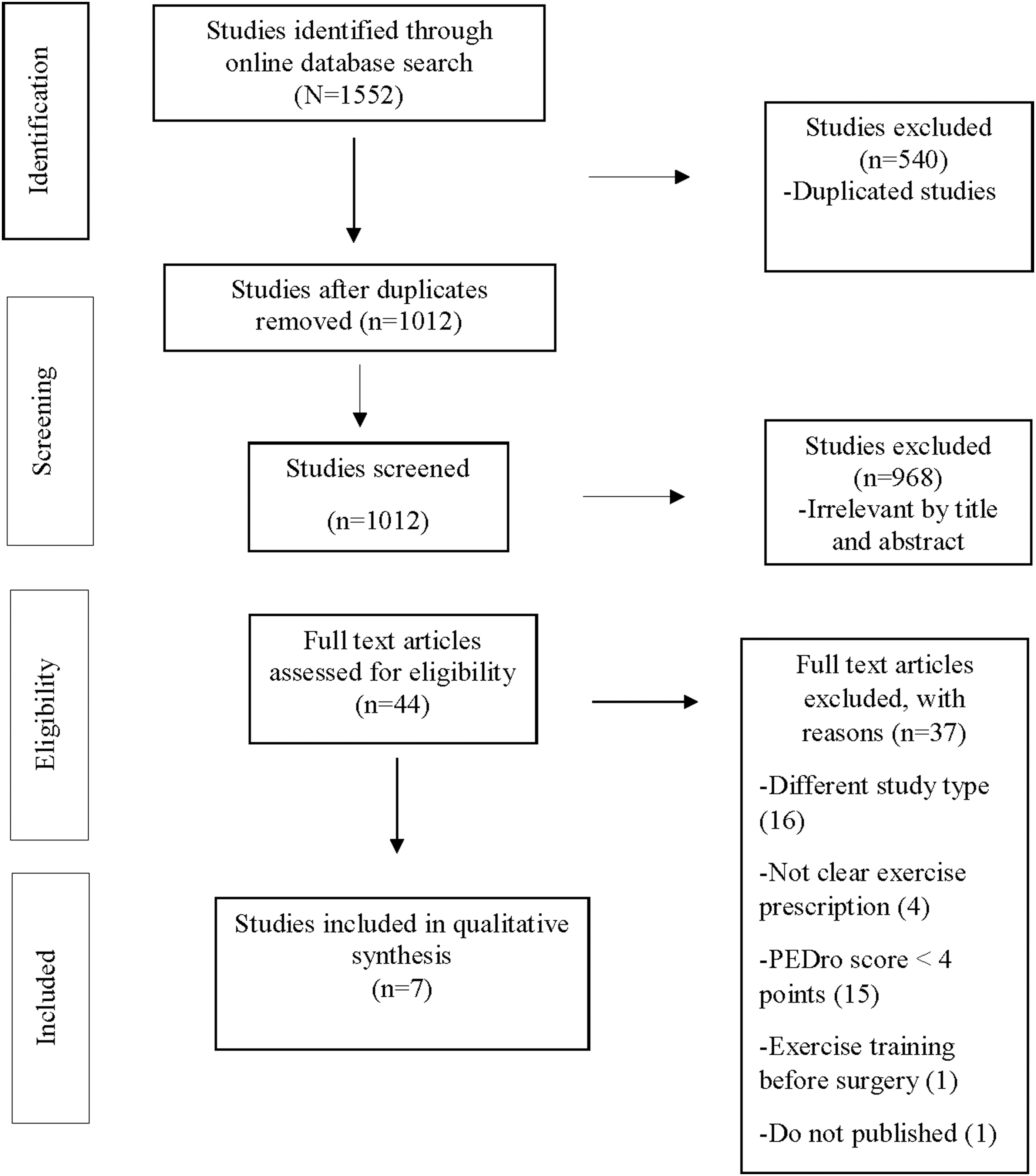
Flow chart.
Characteristics of included studies
The distribution of studies according to years was two articles in 2011, one article for each of 2013, 2016, and 2017, and two articles in 2018. The included characteristics are shown in Table 1. The included studies mainly focused on three different surgery types: Roux-en-Y gastric bypass, gastric bypass, and gastric band.
Study Characteristics
BMI, body mass index; CG, control group; FEV1, forced expiratory volume; FVC, forced vital capacity; GBS, gastric bypass surgery; HR, heart rate; HRV, heart rate variability; HVEP, high volume exercise program; IG, intervention group; REE, resting energy expenditure; RM, repeated maximum; RYGB, Roux-en-Y gastric bypass; TG, training group.
The included studies reported data on 255 patients. The mean number of patients within each study ranged from 16 to 60 (33.9 ± 13.11) years. In general, the patient population was middle aged (41.94 ± 9.11 years) and follow-up ranged from 4 weeks to 24 months. There were more women than men in all of the studies. Three studies included only female patients, the other studies had more than 80% female participants. The study characteristics are shown in Table 1.
Exercise programs
The duration of intervention was between 4 and 26 weeks. The frequency of the session was two to five times per week and each session was ∼30–80 min. The average duration since surgery ranged from 1 month to 3.5 years in the intervention group. Three studies used aerobic exercise for the intervention group, two studies planned resistance training, one study used an outpatient physiotherapy program that included breathing, strengthening, and stretching exercises, and one study used a combination of endurance and strengthening exercises.
Discussion
In this review, we aimed to determine the optimal exercise program after bariatric surgery. Seven studies were included in the review and the effects of exercise on interested parameters after bariatric surgery were examined.
No adverse or negative effects of exercise after bariatric surgery were reported.16,17 In previous literature, the effects of exercise on weight loss, physical fitness, and wellness have been clearly defined. 18 However, consensus as to what constitutes an exercise program, and what is the intensity, duration, or volume after bariatric surgery remains uncertain. The current recommendations for exercise, derived from an extensive review of data pertaining to nonsurgical patients by the American College of Sports Medicine (ACSM), suggest a minimum of 30 min per day, totaling at least 150 min per week. On the other hand, the ACSM also recommends 60 min of moderate-intensity exercise for at least 5 days per week (300 min of exercise/week) to achieve substantial weight loss. 19 Based on the ACSM recommendations, the optimal exercise program should be planned for a minimum 300 min per week to achieve and protect weight loss. 20 In previous literature, low–moderate-intensity or a combination of low and moderate-intensity exercise programs were recommended.21,22
All of the studies included in this review focused on postoperative exercise. It is unclear if preoperative exercise would have an additional positive effect in the postoperative period. Therefore, preoperative exercise planning should be done and this subject would contribute to the literature. 23
There was no common exercise type in the included studies, which are largely heterogenic. There is no uniformity with regard to outcome variables and little is known about the effect of exercise programs on weight regain after bariatric surgical interventions. Stretching and strengthening exercise have a positive effect on muscle strength and walking distance.24,25 Also, aerobic exercise has benefits on energy consumption and heart rate variability.26,27 While preparing exercise programs, depending on the aim, such as weight regain or muscle strengthening, researchers can choose or combine these types of exercises.
In the majority of studies on exercise in the bariatric population, exercise has no adverse effects and positive effects on functional capacity, physical and cardiorespiratory fitness, body composition, muscle strength, and energy consumption have been described.16,28,29 Based on the ACSM's recommendations, a minimum 150–300 min per week, gradually increasing low–moderate-intensity, and a combination of aerobic, strength, and stretching-type exercise should be planned in postoperative patients who have undergone bariatric surgery. 20 Forty-eighty–minute workouts, including a 5-min warm-up and 1-min recovery period is appropriate for such patients. Their program frequency can be planned 2–5 days per week, for 4–24 weeks in total. The intensity can be set as 50–70% of heart rate peak exercise or it can be adjusted to lose ≥2000 kcal/week. Aerobic exercise training should be included in addition to breathing, stretching, strengthening, and core exercises.
In light of the results of this review and ACSM, we recommended the exercise program, which includes warm-up sessions, strengthening training, aerobic training, breathing exercises, stretching exercises, and cool-down sessions at least for 12 weeks for bariatric surgery patients. In addition, we recommend that the exercise program and physical activity be continued after the 12th week to achieve long-term weight control, reduce cardiometabolic risks, and produce behavior modification. The recommended 12 weeks exercise program was given in Table 2.
The Recommended 12 Weeks Exercise Program
Conclusions
Gradually increasing low–moderate-intensity exercise, and a combination of aerobic, strength, and stretching-type exercise should be planned comprising a minimum 150–300 min per week in postoperative bariatric surgery patients to prevent weight gain and maintain weight loss. The consensus on the optimal exercise prescription for the bariatric populations is not yet clear. For this reason, further studies examining the type, duration, and long-term effects of exercise are needed.
Ethics Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Footnotes
Author Disclosure Statement
No competing financial interests exist. There are no conflicts of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.