
Abstract
Background:
The provision of a postbariatric multidisciplinary long-term follow-up is recommended, however challenging.
Methods:
Multidisciplinary teams of two centers, a multi-institutional center for diagnostics and representatives of general practitioners in a Dutch metropole region composed a transmural protocol for transferring bariatric patients 2 years postoperatively to primary care. The quality of these transfers was measured by medical outcomes, quality of life, satisfaction, laboratory results, and re-referrals.
Results:
Two hundred twenty-two patients were referred according to protocol of which 150 patients were sent beyond 5 years postbariatric. For 11 patients the outcomes were not provided, 3 untraceable, and 11 no-shows, leaving a total of 47 patients for evaluation. Laboratory results were discussed in 32 patients, the psychologic screening questionnaire in 7 patients. It led to referral to the obesity center in six and to additional psychological treatment in four cases. The average satisfaction was graded 6.8.
Conclusions:
A disappointing low portion of patients was referred to primary care still resulting in an incomplete follow-up. The composition of a transmural protocol by all caretakers did increase the first-level knowledge. The authors assume that this is beneficial for long-term referrals; however, obesity teams should focus on adherence in the first 5 years at a bariatric center.
Introduction
Multidisciplinary long-term follow-up is recommended after bariatric surgery, and the provision of an adequate follow-up program is mandatory for bariatric centers. 1 However, giving the accumulating numbers of bariatric patients, follow-up should be at least, in part, transferred to primary care over time. Referral to the bariatric center is often necessary and should be possible, but there is a growing need for dissemination of first-level knowledge in managing bariatric patients. 2 In The Netherlands the guidelines recommend bariatric centers to follow-up at least for 5 years. 3 All centers have facilities to provide such a program; nevertheless, adherence is decreasing over time. This has been reported by others as well.4,5
The abovementioned challenges were discussed during a meeting of representatives of obesity teams with general practitioners all within the same region with approximately one million inhabitants. Even though there are clear guidelines available, all agreed that there was a lack of a well organized structure for long-term follow-up, deficits in knowledge from both sides on transferring patients, and a decrease in commitment to follow the provided 5-year programs of the bariatric centers. It led to the formation of a study group focusing on these problems. Within the region there is a system of so-called Regional Transmural Agreements (RTAs) to enhance substitution of care. Transmural care is the interface between primary and secondary care in medicine. The focus group sets a goal to compose such a RTA for morbid obesity. Thereafter a pilot study was conducted to explore the possibilities to send patients earlier to the primary care. This article describes the process of setting up a new RTA and to evaluate the outcome after transferring patients in stable condition at least 2 years after bariatric surgery to primary care.
Materials and Methods
Metropole Region Eindhoven (MRE) is a collaboration of 21 townships with nearly one million inhabitants. 6 Within this region, two large bariatric centers provide bariatric services. They collaborated years ago in the same composition of the bariatric guidance program and have regular meetings with first level care providers. Out of these meetings, multidisciplinary obesity teams of both centers, a multi-institutional center for diagnostics and representatives of general practitioners of MRE composed a transmural protocol for transferring bariatric patients. This RTA was supported by educational meetings and eLearning modules to increase knowledge in managing bariatric patients for primary caretakers. The study group overviewed the process and updated/adjusted the RTA if necessary. The most recent version is provided (Appendix A1).
Patients in stable condition at the 2-year follow-up at an obesity center were asked to continue their program at primary care. The eligible group that inhabited the same metropole region was estimated to be 35% of the 3500 bariatric procedures done in a 2.5-year study period. The definition of stable condition was up to the physician's decision. Although encouraged by the physicians/nurses of the obesity centers through oral and written information, patients were completely free in their decision where to continue their program. In case of agreement, an informative discharge letter was sent to the general practitioner (GP), and the patient was signed up for the center for diagnostics.
Patients received annually a call for blood samples (Appendix A1) accompanied by a psychological questionnaire. The results of the former one were sent to the GP; the patient was asked to bring their completed questionnaire along when visiting the primary care. The psychological questionnaire consisted of a set of monitoring questions to support discussing these aspects during the visit. Furthermore, the compulsory RAND-36 quality of life, a numeric rating scale on satisfaction of the program, was asked to be completed. During the contact with the general practitioner or (psychological) nurse at the primary care center, laboratory results were discussed, weight measured, and if necessary the patient was referred back to the obesity centers. The reasons for contact/referrals were educated during the meetings and elearning, as well as summarized in the RTA.
In 2017 there was an interim analysis of the preliminary data. These data were too scarce that no conclusion was drawn. At the end of 2018 again all data were gathered. For this purpose, all patients had provided informed consent. The data collected included weight, evolution in comorbidities, complications, quality of life, satisfaction of the program, laboratory results, and possible referrals back to the obesity centers. Most data were retrieved from the registry of the diagnostic center and questionnaires; for missing data the GP was contacted once.
Results
A total of 222 patients were referred according to the transmural protocol. For 150 patients, this was beyond the first 5 postbariatric years (104 patients were sent by the general practitioners and 46 by an obesity team). Of the remaining, 11 patients were treated by GPs not providing the outcomes, 3 were untraceable, and 11 did not show up, leaving a total of 47 patients for evaluation of mid-term results. Their male:female ratio was 8:39, mean age 50.7 years, and their average total weight loss was 32.6%.
The no-show rate was 32% as 15 out of 47 patients never contacted the GP after the blood samples or for any other reason. Five GPs actively asked for a visit; however, no additional visit was noted. The laboratory results were discussed for the remaining 32 patients, not always by the GP. The evolution of comorbidities and the extent of laboratory results were too diverse to be analyzed, however, 15 times an adjustment in treatment followed after the visit. The results from the psychologic screening questionnaire were the subject in 7 out of 47 visits. It led to referral to the obesity center in six and to additional psychological treatment in four cases (Table 1).
The Follow-Up
GP, general practitioner.
Quality of life was rated 7 out of 9 times which improved compared to preoperative RAND36 results, once equal and more disappointing for one patient. The satisfaction of the program was graded 6.8 on a 10-point scale on average.
Discussion
Bariatric surgery is the only treatment with proven long-term effect for morbid obesity. Nevertheless in more than half of the patients weight regain occurs. 7 The contributing factors to this regain are multifaceted in their complexity, however, potentially reduced with self-monitoring strategies. 8 Furthermore, a guidance program after a bariatric procedure is necessary for detection of (micro)nutrient deficiencies or late complications. 9 For this purpose, a follow-up program is compulsory for at least the first 5 years in the Netherlands. With 18 bariatric centers and even more institutions providing such a program, possibilities are always nearby. Nevertheless increasing no-show rates during the years postbariatric are challenging. In contrast, there is a burden for sources and personnel, and most patients will be referred to general practitioners after 5 years. So, transferring postbariatric patient earlier to primary care could be a solution for improving adherence and was the subject of the present study.
To be honest, the results were regarded as disappointing. We could identify some possible explanations for these results. First only a very low portion of patients was referred. As only those who visited the obesity centers (and thereby showing their commitment) were asked to participate, maybe they were more adherent to the follow-up program in secondary care. They started before the surgery with emphasis to the clinical pathway and were free of choice to complete this. Despite all members of the obesity teams agreeing to the study, their dedication to provide this care themselves could have influenced the discussion on transferring to primary care. As the diagnostic center called the patient for the first time 1 year after the referral, some patients did not yet receive the invitation due to the time limits of the study. Nevertheless, only 47 patients out of a merely 1000 eligible patients are scarce and beyond the influence of abovementioned factors. Second, in this small group of patients who agreed to visit their GP, one out of three did not show up. And even a smaller number of completed questionnaires were available. No conclusion could be drawn out of these data. Trying to grade the quality of the visits, not every patient discussed the status of health with their GP and/or nurse. For the sake of future comparable programs a possible useful root-cause analysis is added (Fig. 1).
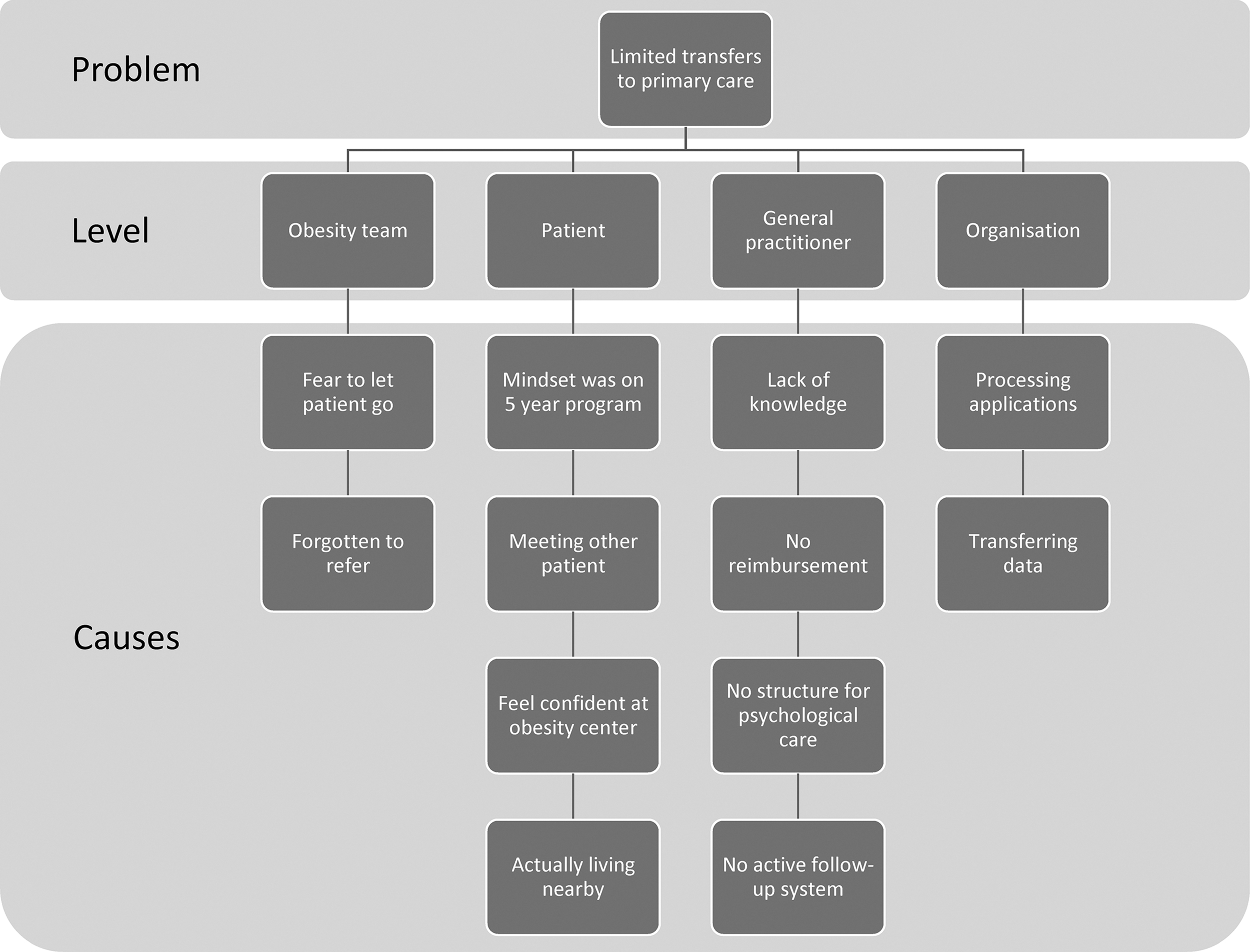
Root-cause-analysis.
In contrast, several useful lessons were learned out of this pilot study. First, looking at the referrals back to the obesity centers, to additional psychological pathways, and number of adjustments after the laboratory results, they underlined the importance of a follow-up program. Second, through a continuous process of updating the RTA, knowledge on both levels increased. Finally, the relatively high number of referrals beyond the 5 years demonstrated that this service fulfilled an existing need. For these reasons the multidisciplinary project group will go on improving this protocol for those long-term controls.
Conclusions
A disappointing low portion of patients was referred to primary care still resulting in an incomplete follow-up. The composition of a transmural protocol by all caretakers did increase the first-level knowledge. The authors assume that this is beneficial for long-term referrals; however, obesity teams should focus on adherence in the first 5 years at a bariatric center.
Footnotes
Acknowledgments
To the patients and to the other members of the study group: K. Berghuis (physician assistant CZE), de Boer AK (clinical chemist CZE), S. Cosijns (nurse practitioner MMC), F. van Dielen (surgeon MMC), Erdtsieck (internal medicine MMC), M. de Greef (transmural pharmacist CZE), M. van Himbeeck (data management CZE), G. van Hout (clinical psychologist CZE), A. der Kinderen (general practitioner GGZ), A. Lucas (medical director diagnostic center [Diagnostiek voor U]), M. Oosterwerff (internal medicine CZE), M. Oostindiër (coordinator transmural care MMC), M. Said (nurse practitioner CZE), N. Schuilwerve (clinical psychologist MMC), F. Smulders (surgeon CZE), and F. Wittkämper (general practitioner).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.