
Abstract
Background:
The aim of this study was to investigate specific effects of nutrition counseling on nutrition knowledge and eating behavior of obese people undergoing bariatric surgery.
Methods:
Sixty-five consecutive patients (25 without prior nutrition counseling and 40 with at least 6 sessions) from our bariatric surgery center received a questionnaire with two main sections: Nutrition Knowledge and Eating Behavior. The level of impact of nutrition counseling on nutrition knowledge and eating behavior was statistically analyzed using uni- and multivariate analyses.
Results:
The answers to 42 questions in the Nutrition Knowledge section were not significantly different between nutrition counseling educated and uneducated groups. Of all participants, 79.7% achieved 50–75% correct answers. Nutrition counseling educated patients answered significantly more questions correctly in the Eating Behavior section (7/10 topics).
Conclusion:
Nutrition counseling has a measurable impact on the eating behavior of bariatric surgery patients. Knowledge about nutrition and food components was not affected by the nutrition consultations in this setting. Nutrition counseling remains an important part of multimodal therapy for obese patients before bariatric surgery.
Introduction
Obesity is a global health challenge and a main risk factor for disease and early death. 1 Bariatric surgery has proven to be an effective strategy in treating obesity. 2 American Association of Clinical Endocrinology (AACE), The Obesity Society (TOS), and American Society for Metabolic and Bariatric Surgery (ASMBS) international practice guidelines strongly recommend a conservative therapeutic approach as preconditioning for every patient undergoing bariatric surgical procedures. Key elements of this approach are nutrition counseling, cognitive behavioral therapy, and an active exercise program. 3
Nutrition counseling is considered to play an important role in bariatric surgery recovery and success by changing the eating habits of patients in the long term.4,5 However, evidence on the exact influence of dietetic expert consultations on the different aspects of nutrition counseling, such as knowledge about nutrition, food ingredients, and eating behavior, is inconsistent.1,6,7 Parmenter and Wardle first established and validated a questionnaire for general nutrition knowledge in the late 1990s. 8 Based on that work, Feren et al. published the first nutrition knowledge questionnaire for obese individuals in 2011.1,7 Nonetheless, very few questionnaires in the literature fulfill criteria for the development of a valid and reliable assessment of nutrition knowledge and eating behavior.
Various studies have shown a correlation between the level of nutritional knowledge of patients undergoing bariatric surgery and the extent of their weight loss after the procedure. Batar et al. showed that a high frequency of nutrition counseling after laparoscopic sleeve gastrectomy has a positive impact on a patient's weight loss during the first 12 postoperative months. 9 Mangieri and Strode retrospectively demonstrated that formal nutrition education can enhance weight loss following bariatric surgery. 10 Other studies have found that dietitian counseling is an important factor for the sustainability of weight loss after surgical treatment. 11 The importance of nutrition education seems to be uncontroversial, but the aim of this study was to look at the difference between a patient's knowledge about nutrition and their eating behavior as integral elements of nutrition counseling before and after systematic treatment by a dietitian. In contrast to previous studies, we focused on the level of nutrition knowledge and the character of eating behavior of our patients before and after nutrition education, which was completely independent of when the surgical procedure occurred.
The present study investigated the specific aspects of nutrition counseling as knowledge about nutrition on the one hand and eating behavior of the patients on the other hand. To understand these effects, the focus was to measure nutrition knowledge and eating behavior of the participants before and after they have had nutrition counseling, independent of the fact whether they were already operated or not.
Methods
Subjects
The present exploratory pilot study investigated the specific effects of nutrition counseling on nutrition knowledge and eating behavior of obese patients undergoing bariatric surgery. Sixty-five consecutive patients at the Center for Obesity and Metabolic Surgery (University Hospital Mannheim, Germany) were included. Of them, 25 had never undergone nutrition counseling in their lifetime [uneducated group], while the remaining 40 had completed at least one full round of nutrition counseling involving 6 or more informational sessions about nutrition and eating behavior with a professional nutritionist, according to AACE/TOS/ASMBS guidelines [educated group]. 7 Seventeen of the 40 educated patients (42.5%) had previously undergone a bariatric procedure (sleeve gastrectomy or Roux-en-Y gastric bypass).
Patient questionnaire
All participants (educated and uneducated groups) received at a particular time (before or after undergoing surgery) a questionnaire to measure nutrition knowledge and eating behavior with a total of 63 questions divided into four sections: Nutrition Knowledge (43 questions based on the questionnaire by Feren et al. 1 ), Eating Behavior (10 questions), Physical Activity (2 questions), and Sociodemographic Parameters (8 questions) (Supplementary Appendix SA1).
The first questionnaire section covers knowledge about dietary staples of different foods, drinks, and meals, as well as calories, vitamins, and minerals. It also includes questions about healthy eating based on the general recommendations of the German Nutrition Society.
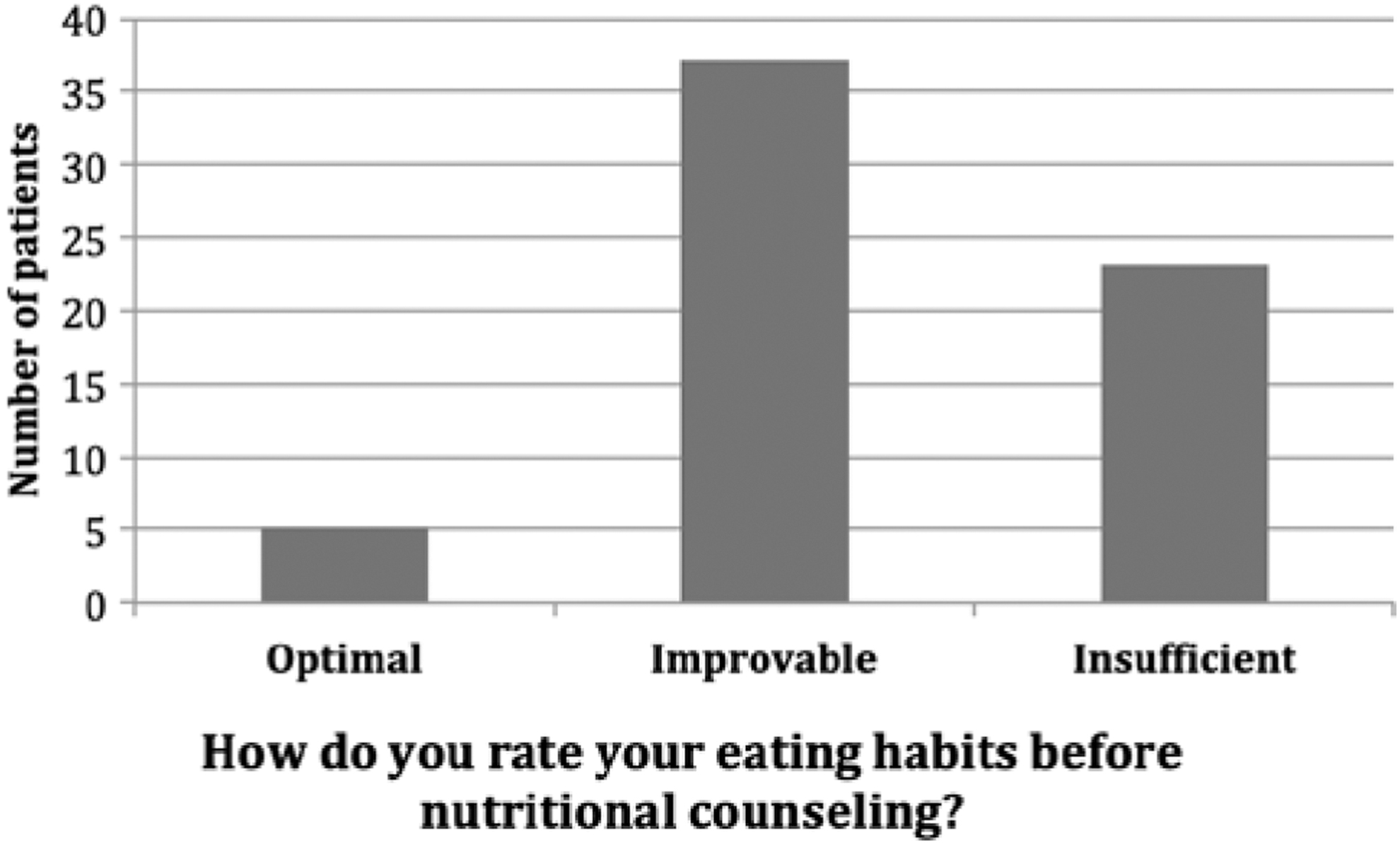
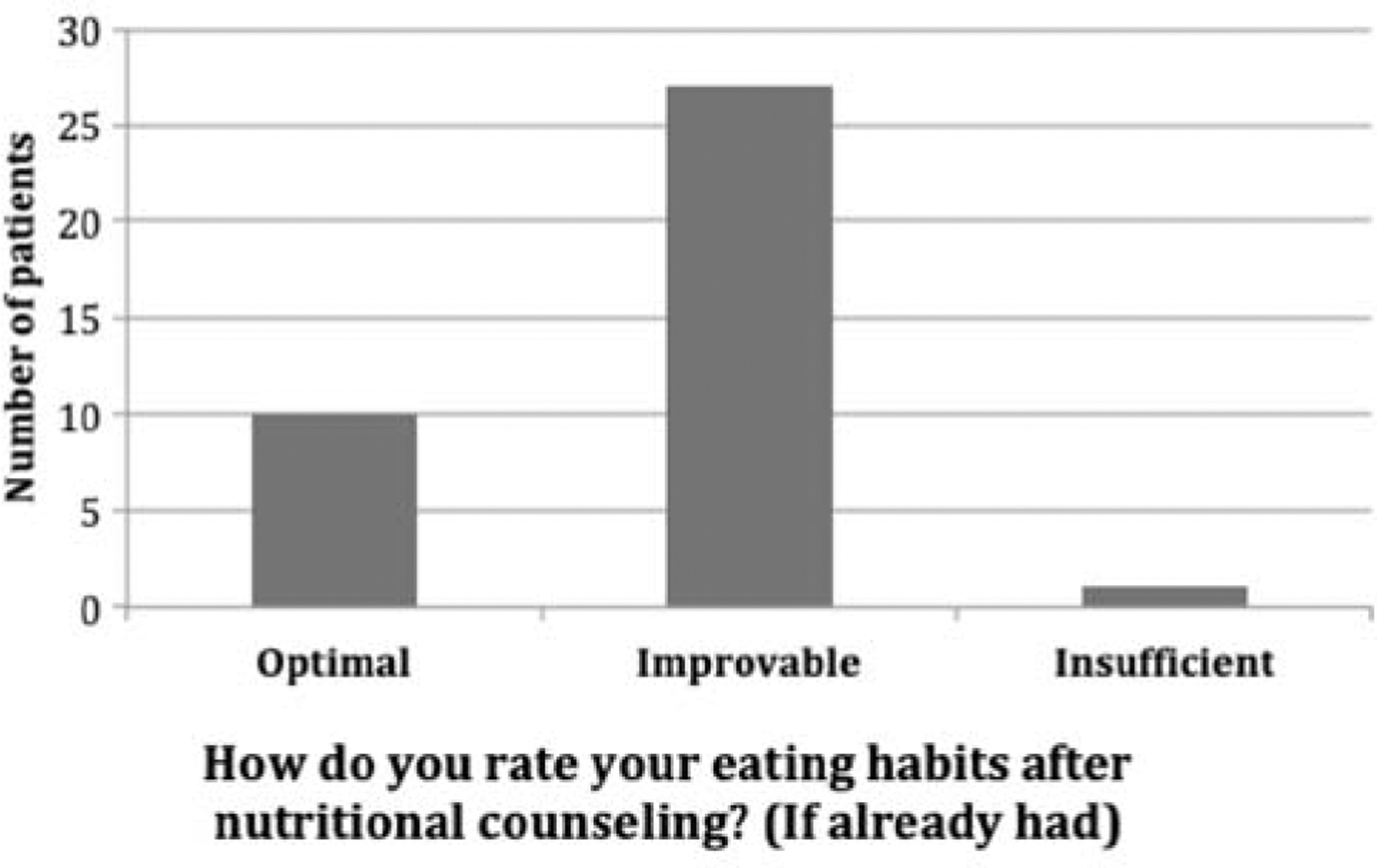
The Eating Behavior section has 10 questions about the individual diet strategy of each patient, including the diet plan, eating protocols, and constant meal timing (eating rhythm). It also contains questions regarding how patients monitor their behavior in terms of weight goals, portion sizes, and solutions for fallback prevention. Two of the 10 questions show how patients rate their own eating habits before and after the professional nutrition counseling (if already completed).
Physical Activity includes an appreciation by patients regarding the general importance of exercise and their own physical condition at the time of the survey.
Sociodemographic Parameters include gender, age, height, body weight, level of education, and employment status.
The questionnaire was constructed in collaboration with the Norwegian study group of Feren et al. 1 and based on official AACE/TOS/ASMBS recommendations and guidelines for healthy food choices and food ingredients, as well as studies on eating behavior and eating patterns. 3 Four different nutrition experts screened the questionnaire for accuracy, appropriateness, and relevance, and the usability and ambiguity of questions were tested on a group of five nutritional science students. Multiple test–retest reproductions were performed to validate the questionnaire as an instrument for the measurement of nutrition knowledge and eating behavior among obese individuals.
A maximum of 102 points was achieved if all questions were answered correctly. Ten questions had more than one correct answer, meaning that more than one point could be obtained with these questions. Questionnaire results were divided as follows to be statistically comparable between the two study groups: 0–25% (poor knowledge), 25–50%, 50–75%, and 75–100% (excellent knowledge) correct answers.
Statistical analyses
The frequency of different characteristics was evaluated by uni- and multivariate analyses. Whether nutrition counseling changes nutrition knowledge and eating behavior was investigated with cross-classified tables. Significance of cross-classification tables was assessed with a chi-squared test; p < 0.05 was considered statistically significant. The statistical analysis of patient responses was performed using SPSS, version 23, software.
The first question in the questionnaire was whether patients considered nutrition counseling useful within the framework of a multimodal therapy for obesity. On a rating scale from 1 (not meaningful) to 10 (very meaningful), the average value of the answers was 7.5 (Table 1).
Average Scores for Question 1
SD, standard deviation.
Results
Patient characteristics
Sixty-five consecutive patients completed the questionnaire. There were 20 males (30.7%) and 45 females (69.3%); the mean age was 41 years (range, 17–66 years).
Fifty-six patients (88.9%) had obesity grade 3 (body–mass index >40 kg/m2), four had obesity grade 2, and one had grade 1. Two patients had a body–mass index of 25 kg/m2 (normal weight).
Twenty-eight patients (43.1%) had a secondary school diploma, 24 patients (36.9%) had a secondary school leaving certificate, and 12 patients (18.6%) had a high school diploma or higher academic grade. Thirty-seven patients were employed at the time of the study and 28 patients were unemployed.
Nutrition Knowledge
This section of the questionnaire consisted of a total of 42 questions. Six patients did not answer the questions of this section on the questionnaire form and were removed from this part of the statistical analysis. Of the remaining 59 patients, five patients (8.5%) answered 25–50% of the questions correctly, 47 (79.7%) answered 50–75% correctly, and 7 (11.8%) answered more than 75% correctly. None of the patients had a score of less than 25% on correct answers for questions (Table 2). There was no significant difference between the educated and uneducated groups in terms of overall percentage of correct answers (p = 0.635).
Distribution of Results of the Nutrition Knowledge Section of the Questionnaire
Eating Behavior
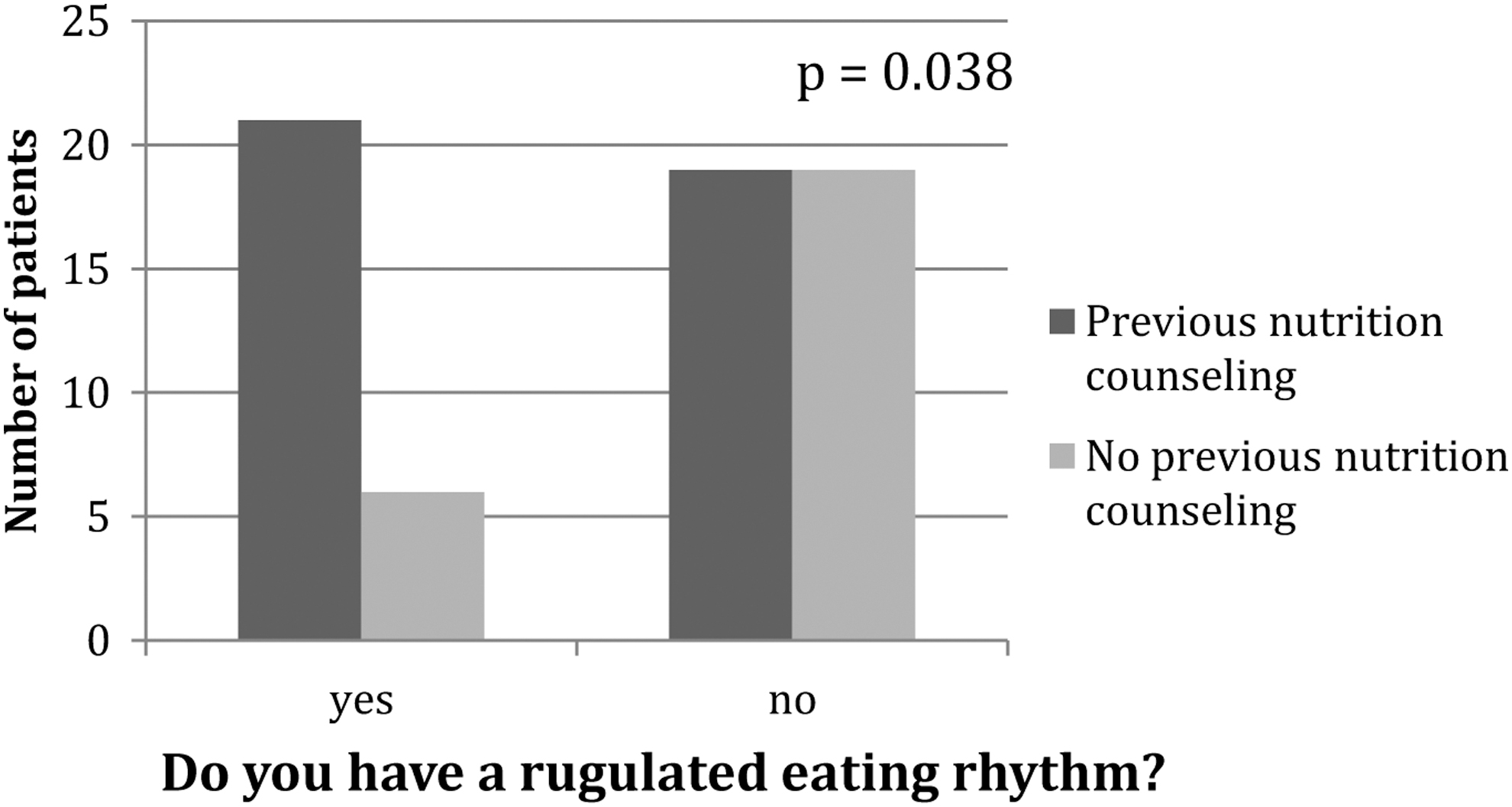
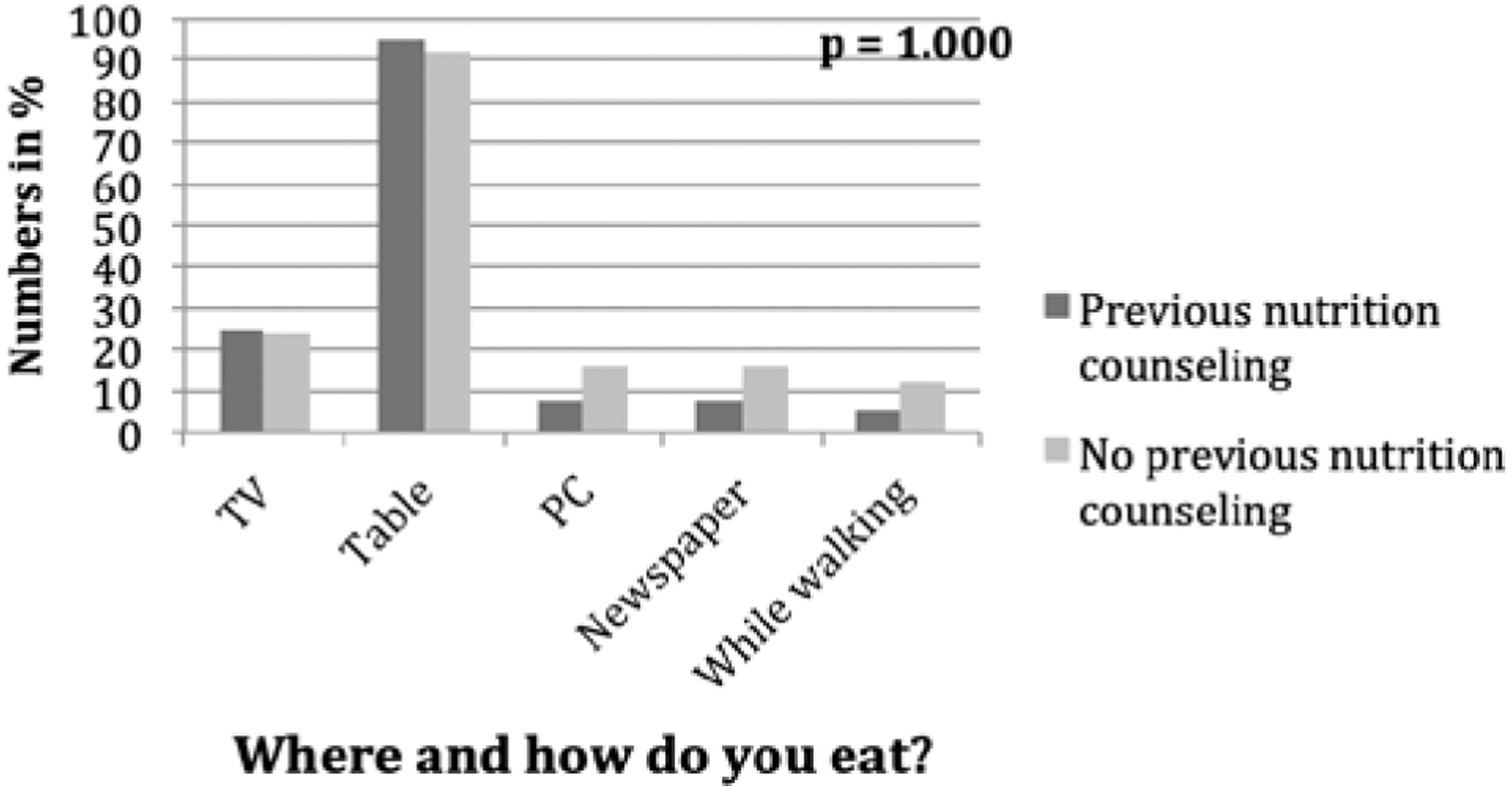
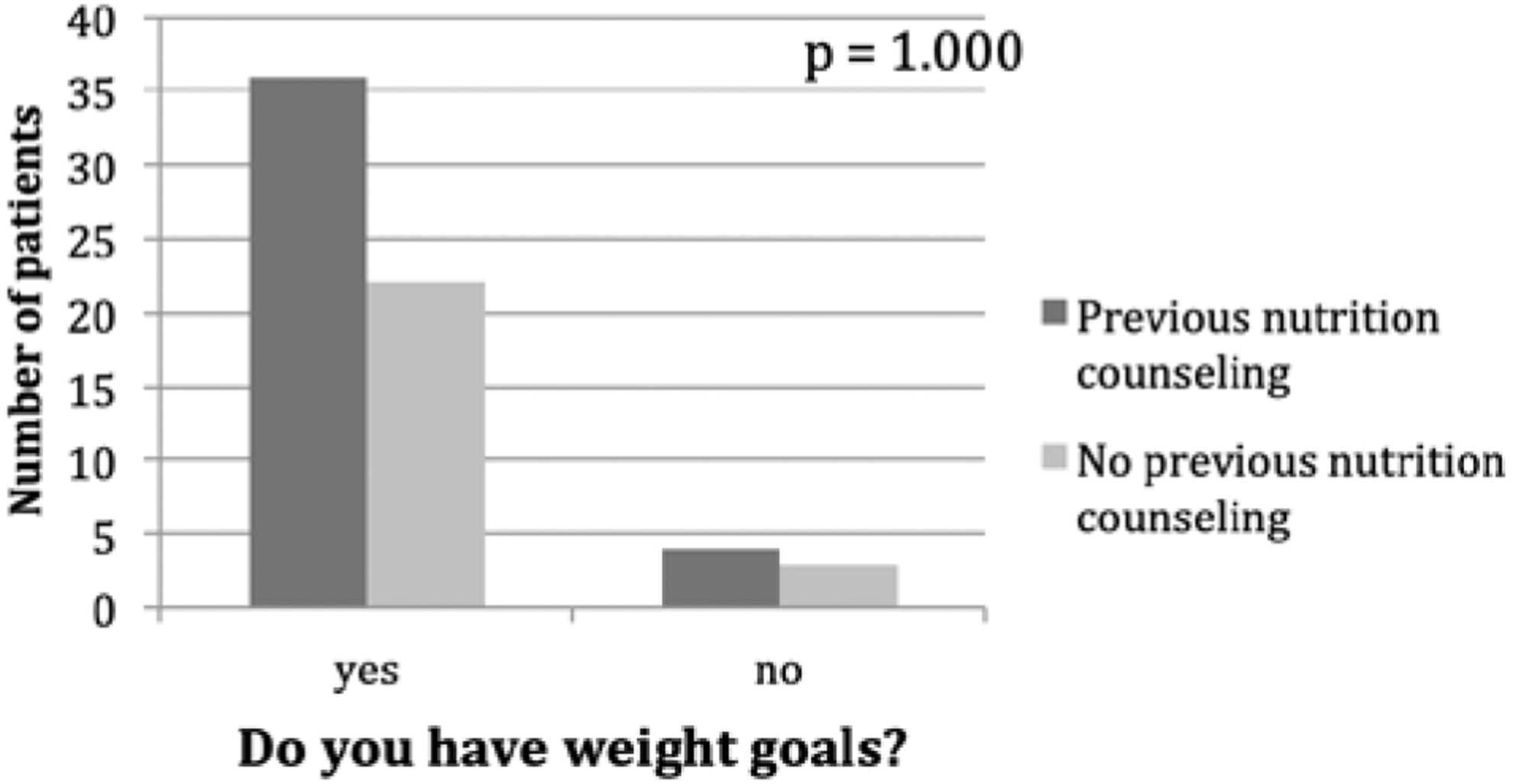
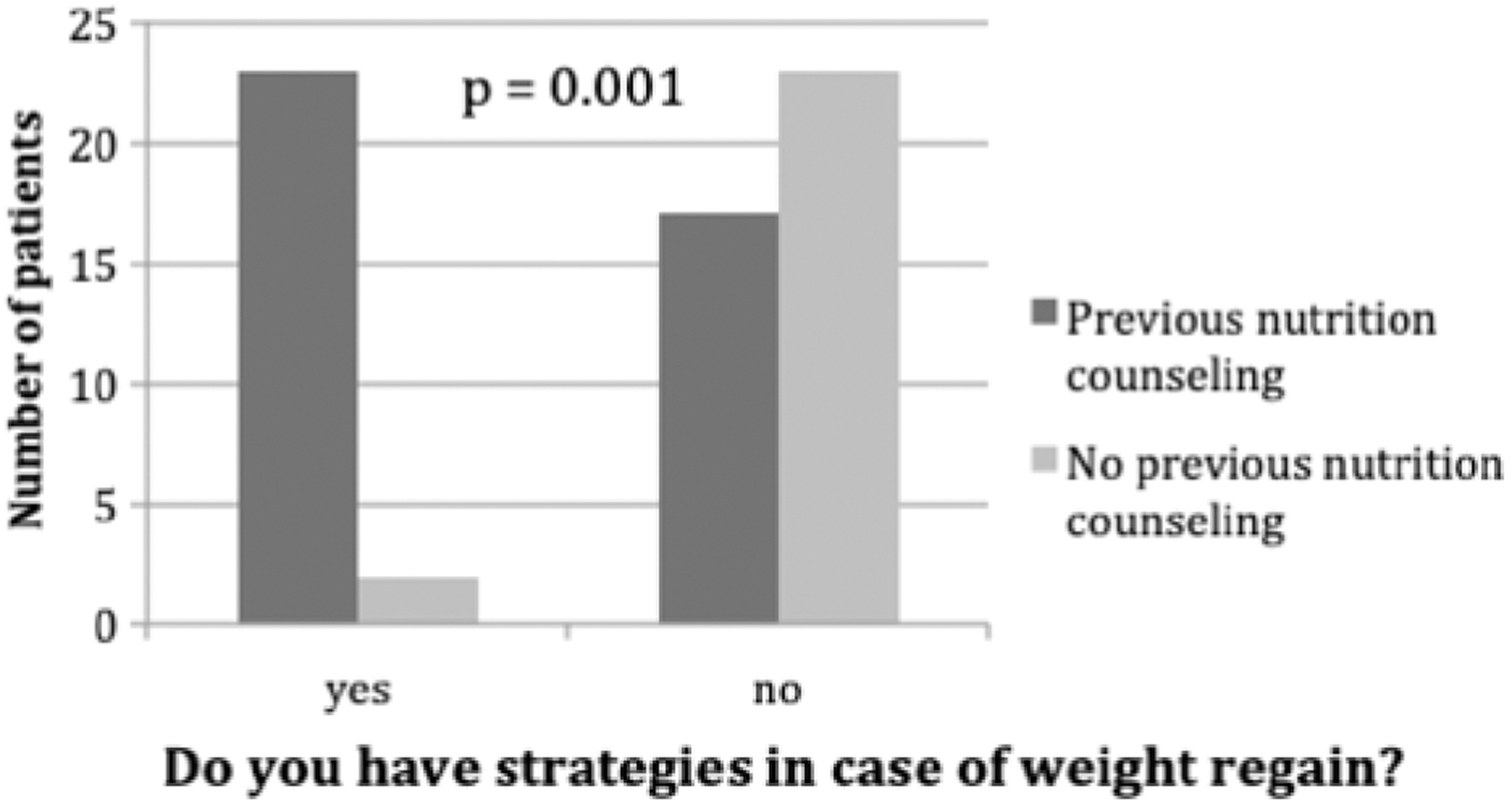
In this section of the questionnaire, a significant difference was detected between the two patient cohorts in favor of the educated group, in terms of having calorie-adapted nutrition plans, using nutrition protocols, eating more varied and diverse food, having a regulated eating rhythm, using self-monitoring models for weight goals, and having strategies for dealing with weight gain. The results of the Eating Behavior section analysis are displayed in Figures 1–10.
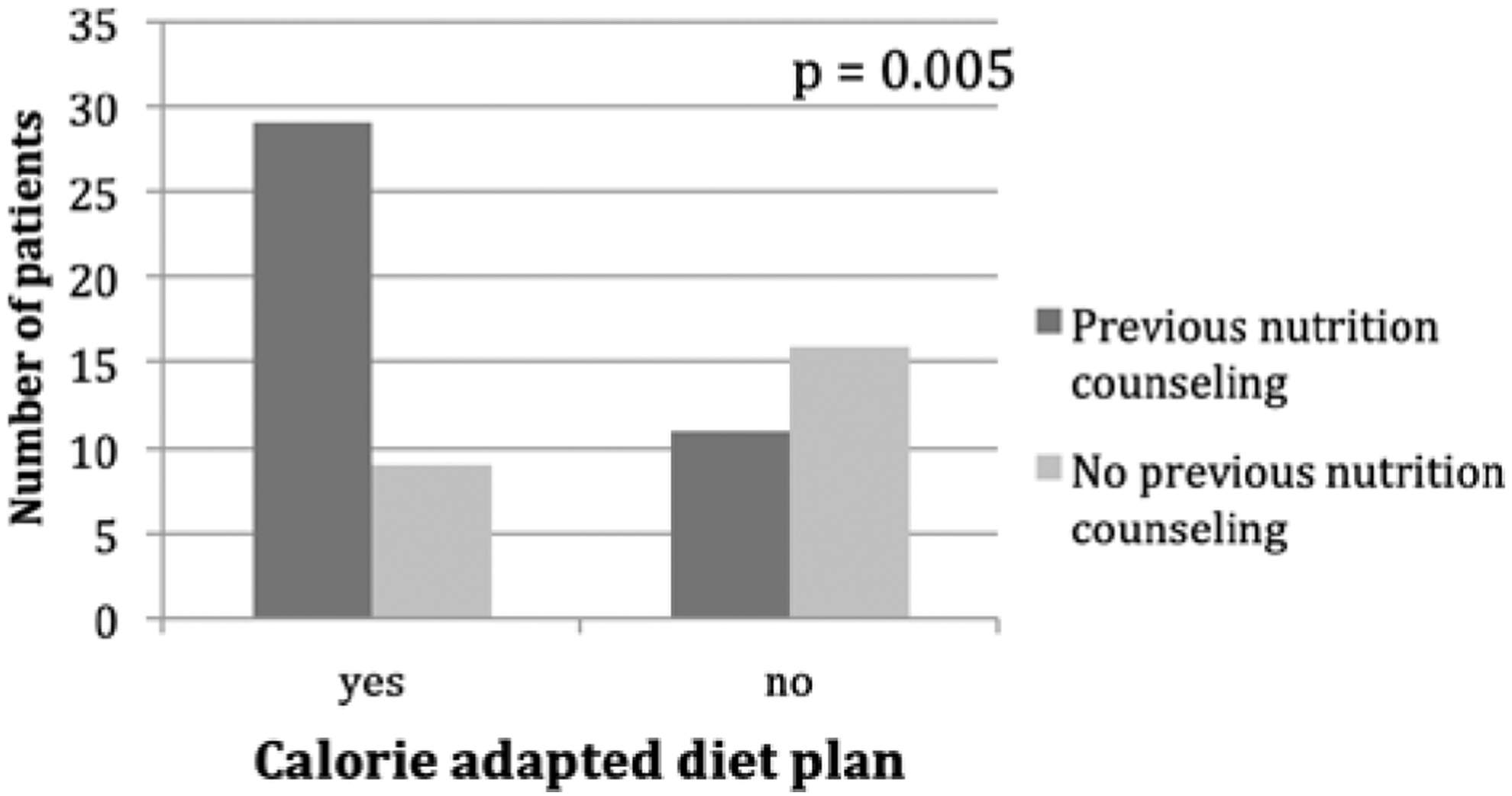
Question 44.
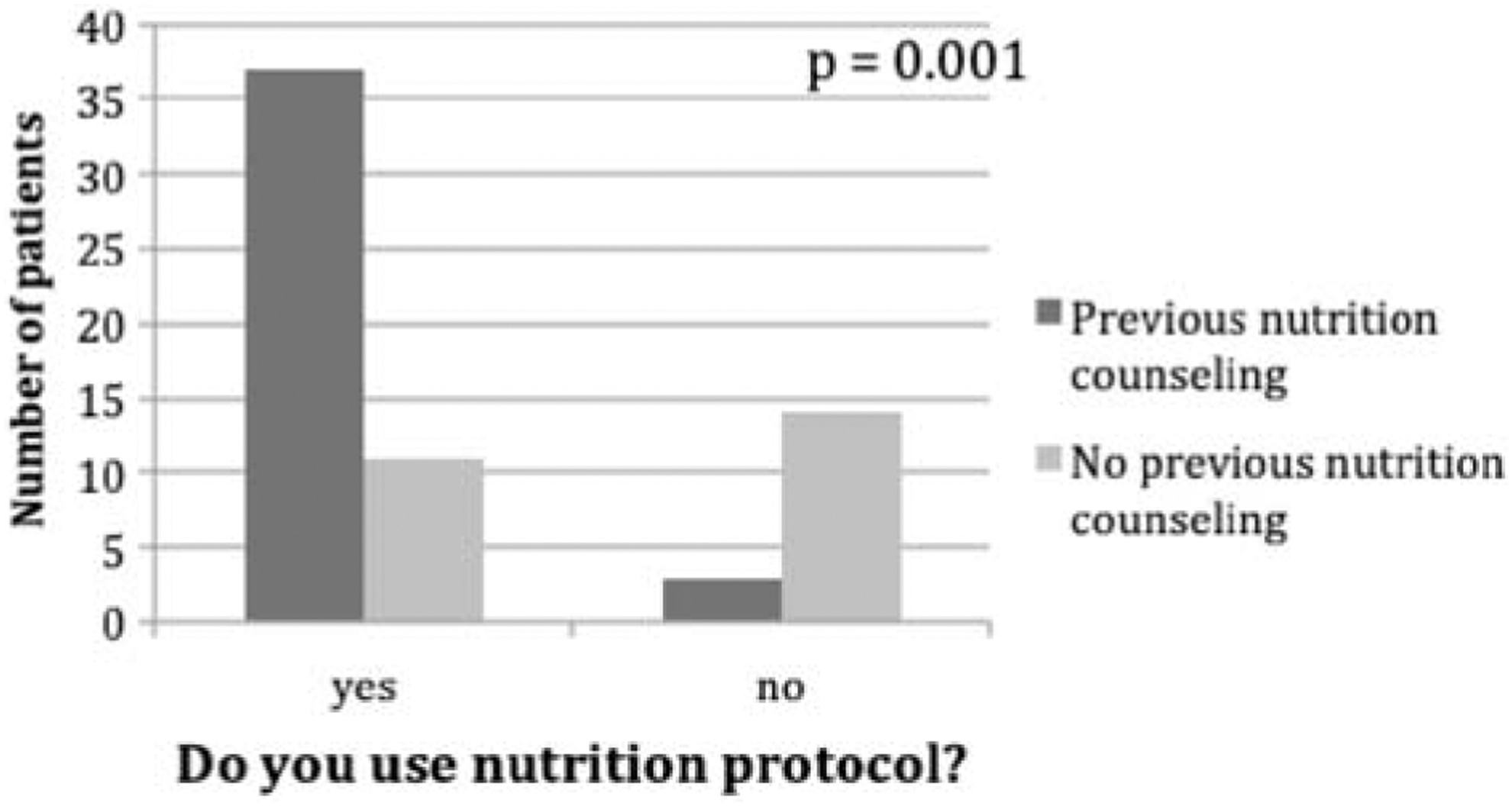
Question 45.
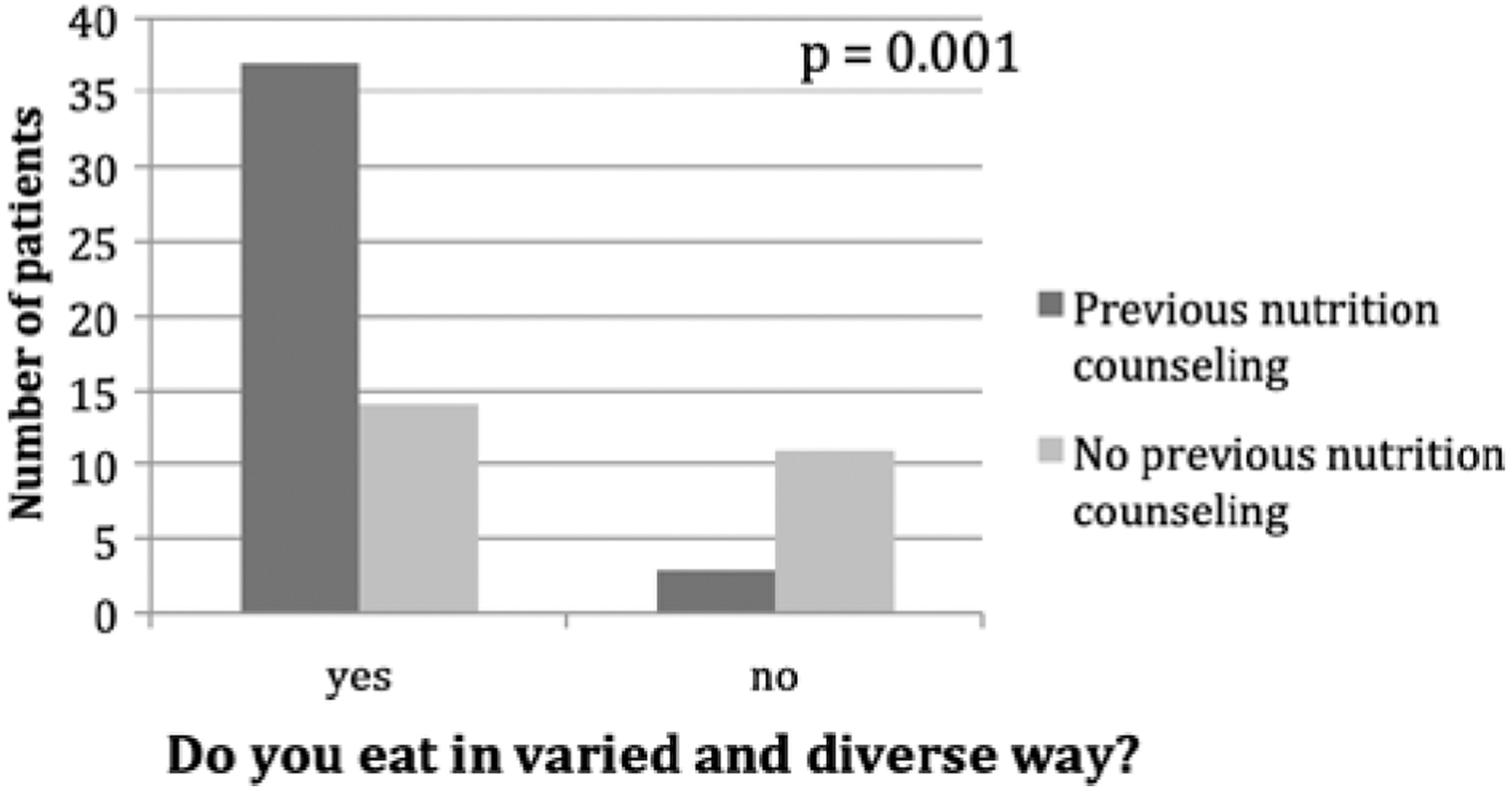
Question 46.
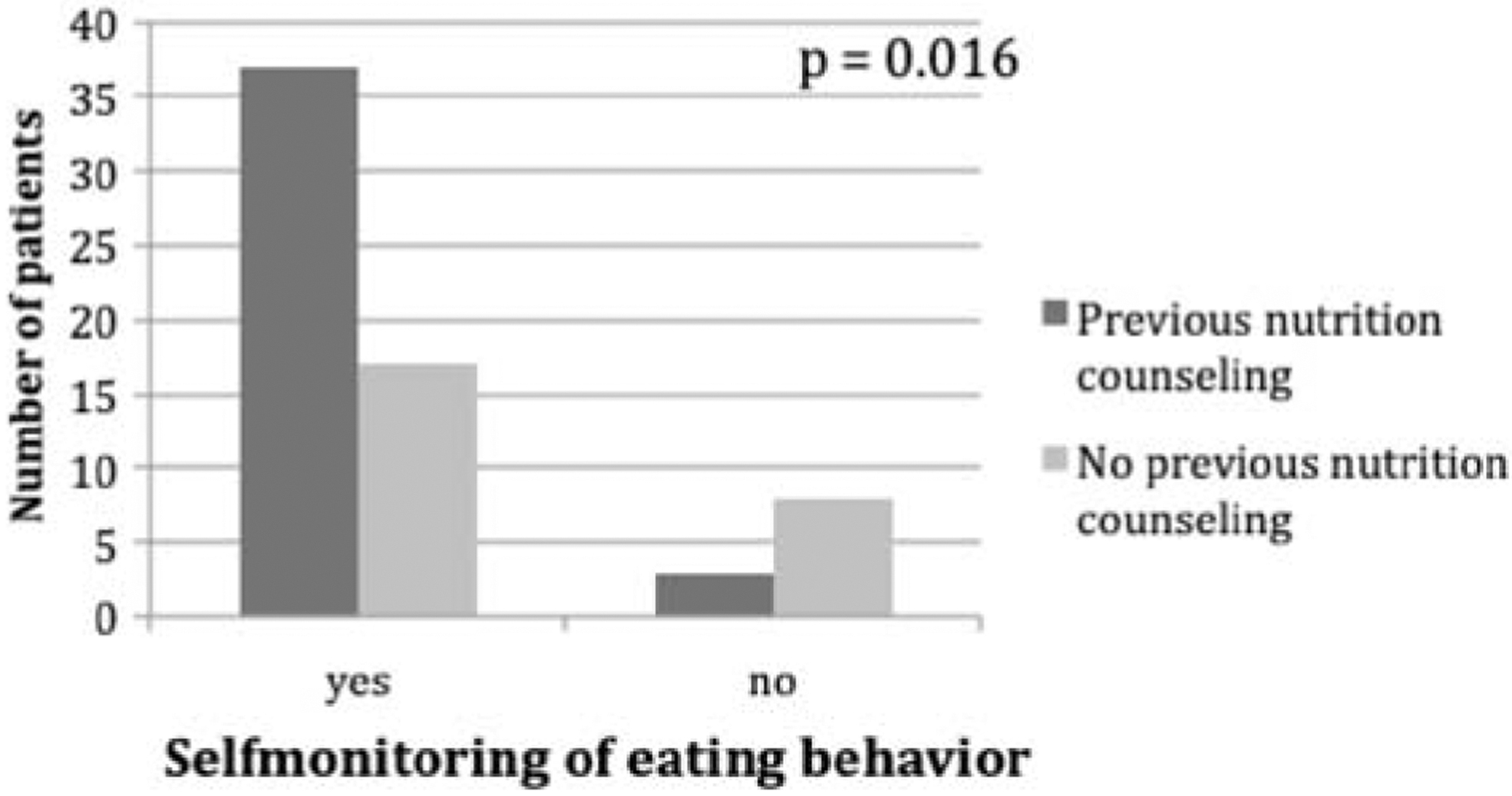
Question 47.
Question 48.
Question 49.
Question 50.
Question 51.
Question 52.
Question 53.
Physical Activity
All 65 participants considered physical activity to be an important part of weight loss. The majority of patients rated their levels of current daily activity and fitness as low to medium.
Discussion
Nutrition counseling plays an indispensable role in the multimodal therapy of obesity, but does it change patient knowledge about nutrition or their eating behavior patterns? To answer this question, the present study subdivides the participants into nutrition counseling educated and nutrition counseling naive groups and does not focus on the time of the surgical procedure.
The results showed a significant improvement in eating behavior for educated compared with uneducated patients. In fact, the educated group was superior to the uneducated group in almost every part of the Eating Behavior section of the questionnaire. Educated patients used calorie-adapted meal plans and nutrition protocols more often, had greater variation and diversity of food choices, and had a controlled meal rhythm. They also employed strategies to prevent weight regain and had better self-awareness of eating habits. Thus, eating behavior can be modified by nutrition counseling and it demonstrates the importance of nutrition counseling as a part of the multimodal treatment of patients with morbid obesity. These results are in line with those of Wardle et al., which showed measurable improvement in nutritional patterns after counseling together with an increase in intake of vegetables and fruits and a shift toward a low-fat diet. 12 However, their results are not unconditionally comparable with the present findings because their trial was not designed for obese or overweight individuals.
The Nutrition Knowledge section of the questionnaire did not detect significant differences between educated and uneducated patients in terms of knowledge about nutrition and food ingredients. Some studies have reported similar results, postulating that dietary counseling is ineffective and does not lead to better nutrition knowledge.13,14 However, those studies did not use validated reliable instruments for measuring nutrition knowledge. The results of the present study also provide information about the importance of differentiating between nutrition knowledge and nutrition behavior/habits when assessing the value of nutrition programs and counseling methods. Future research should be focused on specific tools for measuring these aspects of nutrition coaching targets. The comparable nutrition knowledge in both educated and uneducated groups in the present study can also be explained by the fact that many obese people have already tried several diets in the course of their chronic disease and therefore have a certain amount of knowledge about food and food components. This is particularly reflected in results showing that most patients in both groups were able to correctly answer 50–75% of nutrition knowledge questions.
Sherf-Dagan et al. show in a prospective trial that preoperative online nutrition counseling increases nutrition knowledge of patients in the intervention group before bariatric surgery, as assessed with a nutrition knowledge score; however, this study does not measure the effect after the procedures. These data suggest that nutrition knowledge can be modified over the short term. 15 Nevertheless, other studies discuss the need for frequent dietitian appointments after surgery to maintain a sufficient level of nutrition knowledge with patients and ensure that they adhere to the new eating habits over the long term.9,11 Previous studies have correlated these effects with weight loss after bariatric surgery, which was not the focus of our study. The strengths of the current study are the use of a complex and validated questionnaire tool, which allowed for differentiation between the role of nutrition knowledge and eating behavior as specific elements of nutrition counseling. This represents a novel point of view for dietitians when counseling patients despite the small number of participants in our study.
Although meta-analysis data and prospective randomized trials have not shown a substantial impact of intensive lifestyle intervention (nutrition counseling, diabetes nursing, and physical exercise program) on total weight loss and weight control in the long-term, the role of nutrition counseling in terms of modulating eating habits and patterns seems to be indisputable.16,17 In this context, Andromalos et al. used an 11-question quiz to demonstrate that before bariatric surgery, patients lacked essential knowledge about critical nutritional and behavioral concepts, which lends support to the importance of preoperative education. 18 Their data point to areas for educational focus to help improve postsurgical results and reduce complications. Finally, the short Physical Activity section of our questionnaire showed that obese patients recognized the role of physical activity for weight control, but were largely unable to make sufficient effort toward this area.16,17
In conclusion, the current study revealed that nutrition counseling has a measurable impact on the eating behavior of bariatric surgery patients. However, knowledge about nutrition and food components was not affected by nutrition counseling in the present setting. Thus, nutrition counseling remains an important part of multimodal therapy in obese patients before bariatric surgery.
Study limitations
Although the present study had a prospective design, patients were not randomized, and only a small number of patients were included. Another limitation is that even though the validated questionnaire by Feren et al. 1 was used to create the current questionnaire, several new questions were added, resulting in a new questionnaire that was not validated in the same way. Moreover, the same team of nutritional experts, representing a possible source of bias, did not treat the patients in the present study as nutrition counseling itself was not standardized.
Ethical Approval
The study protocol was reviewed and approved by the local institutional ethics committee. The study was performed according to the Declaration of Helsinki.
Statement of Informed Consent
Informed consent was obtained from all participants involved in this study.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.