
Abstract
Background:
The purpose of this study was to evaluate a stapleless and staple use surgical technique for gastric bypass.
Methods:
Group 1 (n = 20) included patients who had stapleless one-anastomosis gastric bypass. The patients in group 2 (n = 20) underwent one-anastomosis gastric bypass with stapler use.
Results:
The duration of the bypass procedure was 74.68 ± 21.71 min for group 1, versus 85.5 ± 19.2 min for group 2 (p = 0.051). The patients were discharged postoperatively on day 2.88 ± 1.77 for group 1, and day 3.57 ± 1.18 for group 2 (p = 0.04). The change in body mass index (ΔBMI) for both groups 1 and 2 at 12 months postoperative showed good results: a decrease of 12.13 (8.34–15.93) and 16.04 (11.7–20.37) from baseline, respectively (p = 0001). No mortality or serious complications were observed in either group. When comparing the number of adverse events, the difference was not significant (p = 0.07, χ2 = 3.13). Bile reflux was nonsurgical treated with a dietary recommendation.
Conclusion:
Both gastric bypass procedures significantly reduced weight, however, the stapleless method is 62.78% cheaper. The safety and duration of efficacy can be discussed after longer follow-up studies. Trial registration: ClinicalTrials.gov, NCT03667469.
Introduction
In 2004
Therefore, this stapleless method, like the staple-use procedure, is dangerous owing to potential complications of the suture site, such as leakage and bleeding. 3
For low-income countries, the use of staplers for gastric bypass significantly increases the cost of surgery, and therefore reduces accessibility for the majority of these populations. In addition, all stapler-use and previously developed stapleless gastric bypass methods still require cutting the wall of the stomach.
In 2016, we began to perform a mini gastric bypass with obstructive gastroplication for stapleless pouch creation. 4
Methods for this include using a nonadjustable gastric band, absorbable strips of mesh, and gastroplication to obstruct the communication between the gastric pouch and the greater, bypassed part of the stomach. The novel stapleless technique allows broader access to care in resource-challenged environments, which is very important for low-income countries. However, there is little case study-based evidence regarding the efficacy and safety of this technique. Therefore, a randomized trial is required to compare the stapler-use and stapleless one-anastomotic gastric bypass techniques.
The purpose of this study was to describe a stapleless surgical technique for gastric bypass with the creation of an uncut gastric pouch, and to compare the weight loss and adverse events of this method with the staple and cut method.
Patients and Methods
Study design
This study is part of a prospective randomized controlled trial. 5
Morbidly obese patients undergoing gastric bypass from December 2018 to June 2019 were included in this study. The patients were randomly divided into two groups (n = 40), with 20 patients in each group. Allocation concealment was ensured using identical, sequentially numbered, opaque, sealed envelopes.
Inclusion and exclusion criteria
The inclusion criteria were as follows: obese patients (body mass index [BMI] ≥35 kg/m2), 18–60 years of age, with American Society of Anesthesiologists physical status of I or II, and able to provide written informed consent for randomization and treatment. Patients were excluded if they had a BMI <30 or >65 kg/m2, were <18 or >65 years old, had a drug or alcohol addiction, had a mental illness, or were taking antidepressants.
Group 1, the “uncut stapleless” group (n = 20), included patients who had stapleless laparoscopic one-anastomosis gastric bypass with an obstructive stapleless pouch and anastomosis (LOAGB-OSPAN). The hand-sewn gastrojejunostomy was 2.0 ± 0.5 cm. The gastric pouch was 12 ± 1.5 cm in length, with a volume of ∼35 ± 5 cc.
The patients in group 2, the “stapled cutting” group (n = 20), underwent standard laparoscopic one-anastomosis gastric bypass with stapler use (LOAGB-SU). The wide linear stapler use gastrojejunostomy was 3.5 ± 0.5 cm. The gastric pouch was 16 ± 1.5 cm in length, with a volume of ∼60 ± 10 cc.
Outcome evaluation
We compared the operative duration, changes in BMI after weight loss, and adverse events between the two groups. The mean follow-up period was 12 months.
Patient demographics were assessed preoperatively. Ideal body weight was calculated as 25 × (patient's height in meters) 2 . The effectiveness endpoints included BMI (kg/m2), change in BMI (ΔBMI = initial BMI – postoperative BMI), excess BMI loss (excess body mass index lost, % = [ΔBMI/initial BMI −25] × 100), and total weight loss (TWL, % = [(initial weight − postoperative weight)/initial weight] × 100). 6
Endoscopic assessment
All patients underwent endoscopy of the esophagus and stomach before surgery. During the postoperative follow-up, all patients underwent repeat endoscopies of the esophagus and gastric pouch after 3 and 12 months. If bile was detected in the esophagus, bile reflux was indicated and considered unacceptable. Subsequently, an additional surgery was required to convert to a Roux-en-Y gastric bypass. If, during endoscopy, bile was detected in the upper part of the gastric pouch, then reflux was indicated and considered serious, requiring dietary treatment (more frequent fractional meals). If bile was detected only in the area of gastroenteroanastomosis with signs of superficial gastritis in the distal part of the gastric pouch, bile reflux was considered mild. If there were no signs of gastritis in the presence of bile at the gastroenteroanastomosis, bile reflux was considered absent.
During upper endoscopy, the absence of recanalization between the gastric pouch and the gastric partition (durability of nondivided pouches) was assessed in the group where the stapleless technique was used.
Cost-minimization analysis
Cost-minimization analysis was used to estimate the cost data (cost of medical tests, medical materials, surgical services, medications, blood products, nursing care, hospital bed occupation, and miscellaneous items). 7
Surgical technique and procedure steps
The bypass procedure was performed on the operating table, with the patient in a supine split-leg position. The patient was placed in the reverse Trendelenburg position, with the table inclined to 45°.
The procedure began with the creation of windows in the hepatogastric ligament and in the gastrodiaphragmatic ligament (Fig. 1). The first window was created in the pars flaccida, near the lower edge of the dense portion of the hepatogastric ligament. The second window was created in the gastrodiaphragmatic ligament, at the angle of His (cardiac incisura).
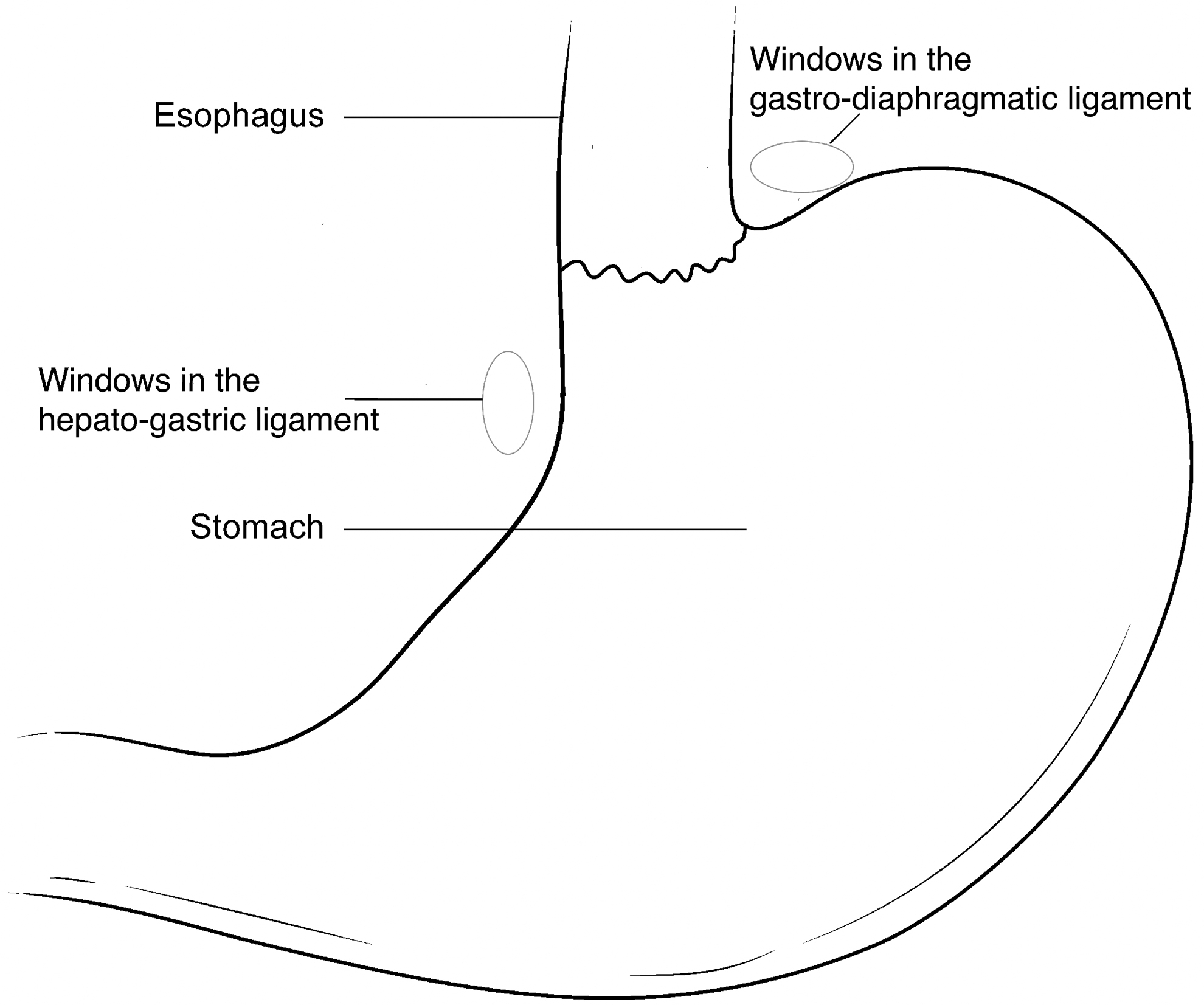
The creation of the windows in the hepatogastric ligament and in the gastrodiaphragmatic ligament.
The next step included the use of a 5 mm laparoscopic instrument to create a retrogastric canal through the space between the posterior wall of the stomach and the diaphragmatic crura, directed from the right diaphragmatic crus and the angle of His. The retrogastric channel was created at the lower, joining edge of the right and left diaphragmatic crura. The ligature, created with Vicryl USP 2-0 (Ethicon US, LLC), which is absorbed within 56–70 days, was introduced through the retrogastric channel (Fig. 2), and pulled into the retrogastric canal.
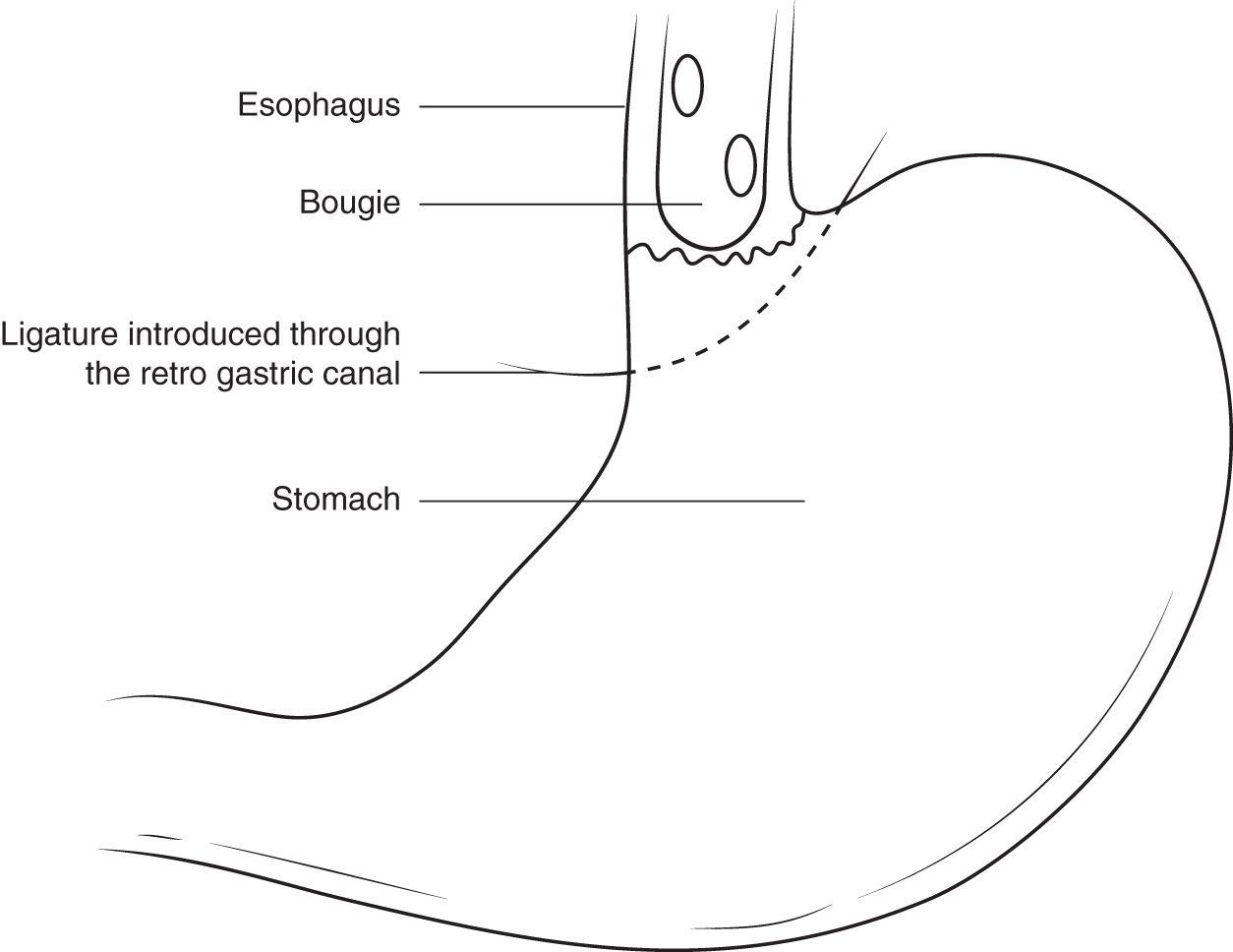
The ligature introducing through the retrogastric channel.
A 32F orogastric bougie (tube) was then pushed along the length of the esophagogastric junction to the crow's foot of the lesser curvature of the stomach, to calibrate the length and volume of the gastric pouch. The length of the gastric conduit must not be <10 cm. The pouch was created only from the front wall of the stomach to the portion that is medial to the vertical line, connecting the angle of His and the crow's foot. The width of the conduit (pouch) should not be >3 cm (similar to an anatomical canal of the pylorus).
After introducing the absorbable ligature through the retrogastric channel and calibrating the gastric pouch, a knot was tied in the ligature. This knot, located around the gastric isthmus, separated the stomach into the gastric pouch and bypassed the stomach (Fig. 3). The tightness between the gastric pouch and the bypassed part of the stomach was tested by air insufflation, which was introduced externally into the gastric pouch through an orogastric tube.
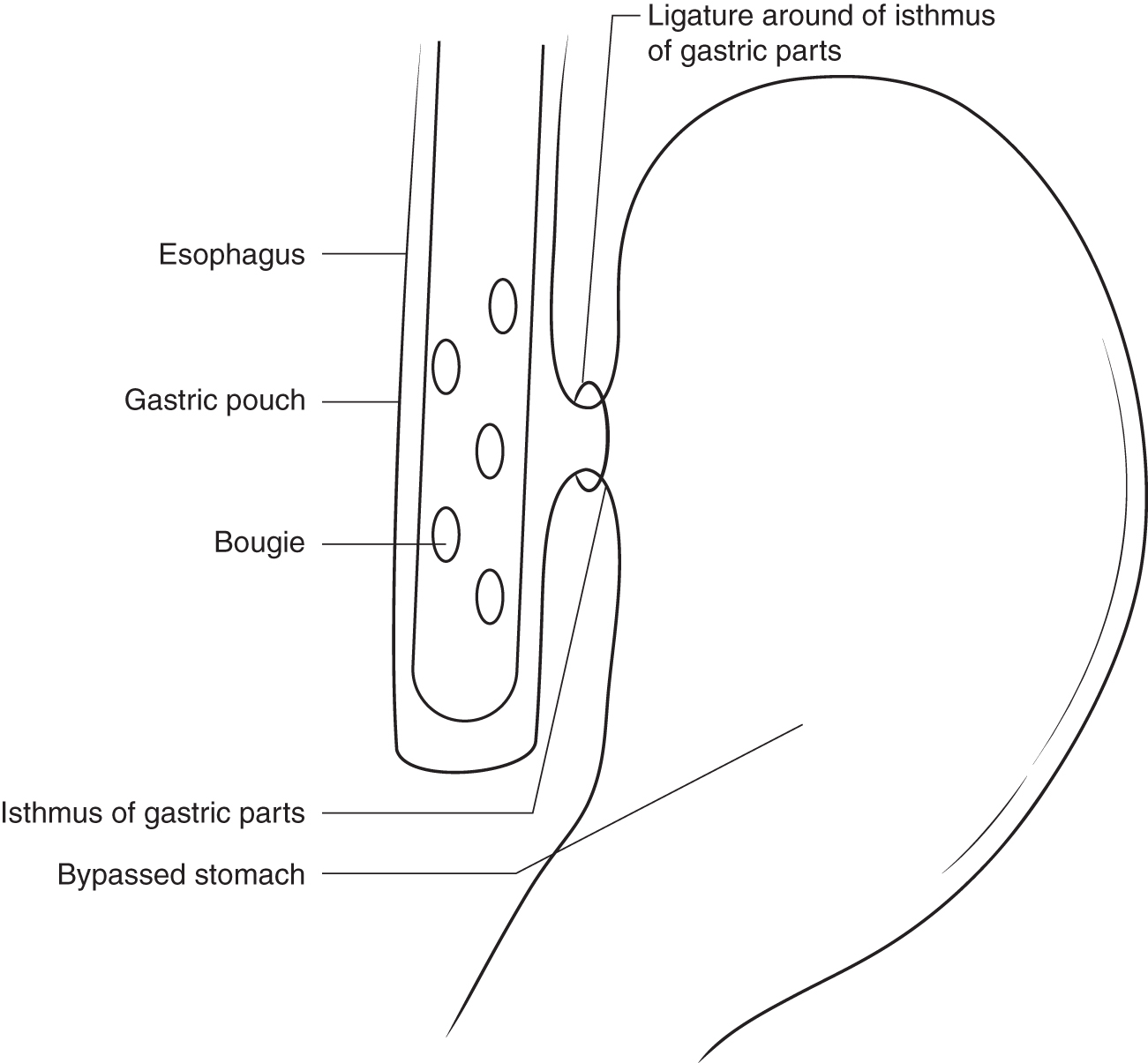
After gastric separation: ligature around of the isthmus of gastric parts.
Gastric greater curvature mobilization was created from across the level of the crow's foot to the left diaphragmatic crus (Fig. 4). After the dissection of a short gastric vessel, the gastric fundus was fully mobilized, allowing for the downward displacement of the gastric fundus.

The gastric greater curvature mobilization and displacement of gastric fundus.
Gastroplication was performed to achieve tightness between the gastric pouch and the remaining stomach after the absorption of the ligature (“gastric tie”). To prevent the development of leakage between the lumen of the pouch and the lumen of the disconnected part of the stomach, we created an obstructive gastroplication. For the creation of the gastric pouch, a gastro-gastric suture was used to close the lumen of the stomach below the isthmus, using nonabsorbable Ethibond 2-0 sutures (Ethicon US, LLC). To ensure a good seal, no less than 5 separate interrupted sutures should be used (Fig. 5). Sutures should alternate, starting at the posterior wall and continuing to the anterior wall of the stomach (Fig. 6). Suturing for gastroplication begins 2 cm below the gastric isthmus. To close the protrusion of the gastric wall after the upper part of the gastroplication, we used a continuous suture, which created an uncut, tubular pouch (Fig. 7).
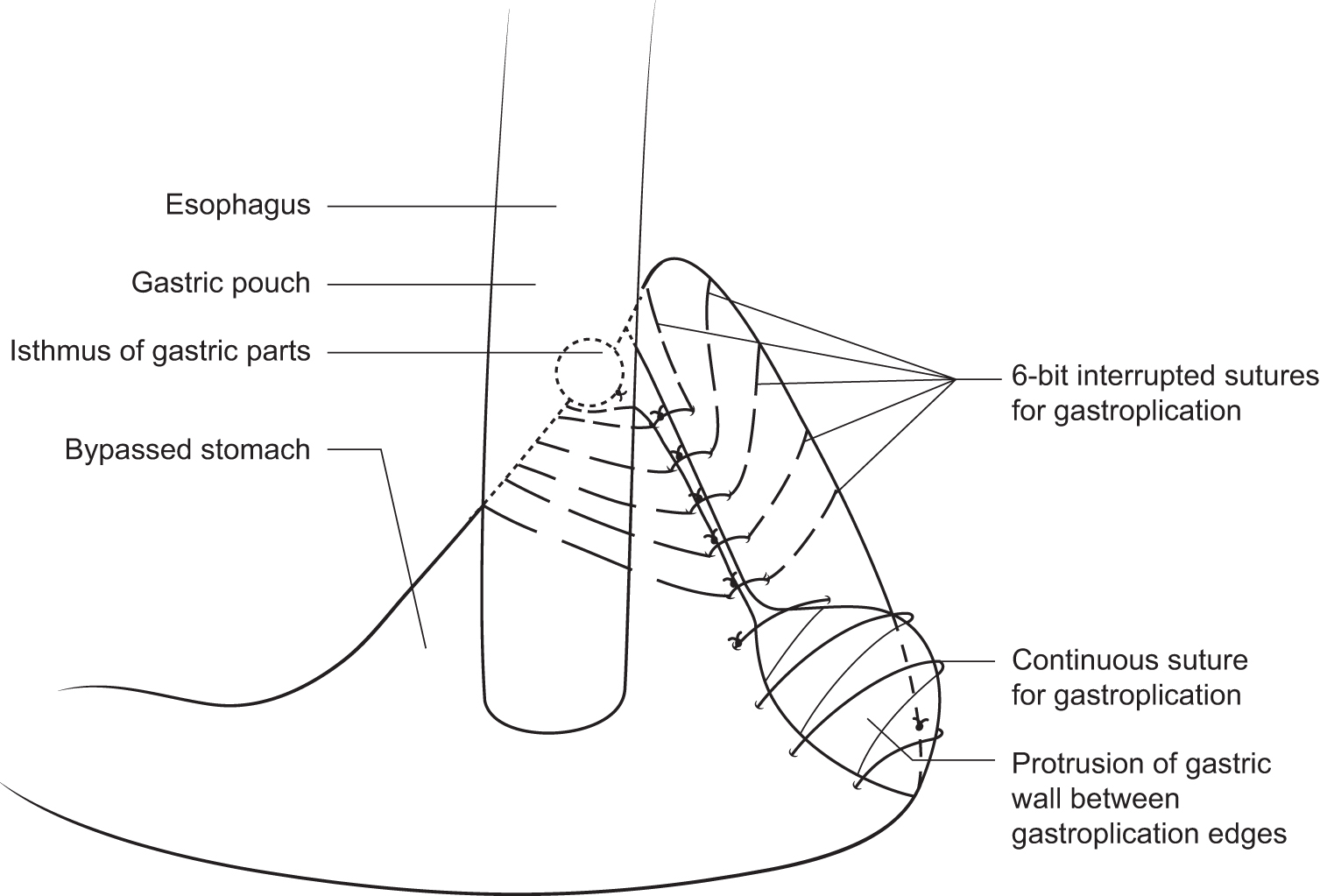
Gastro-gastric suture for finally closure the lumen of stomach.
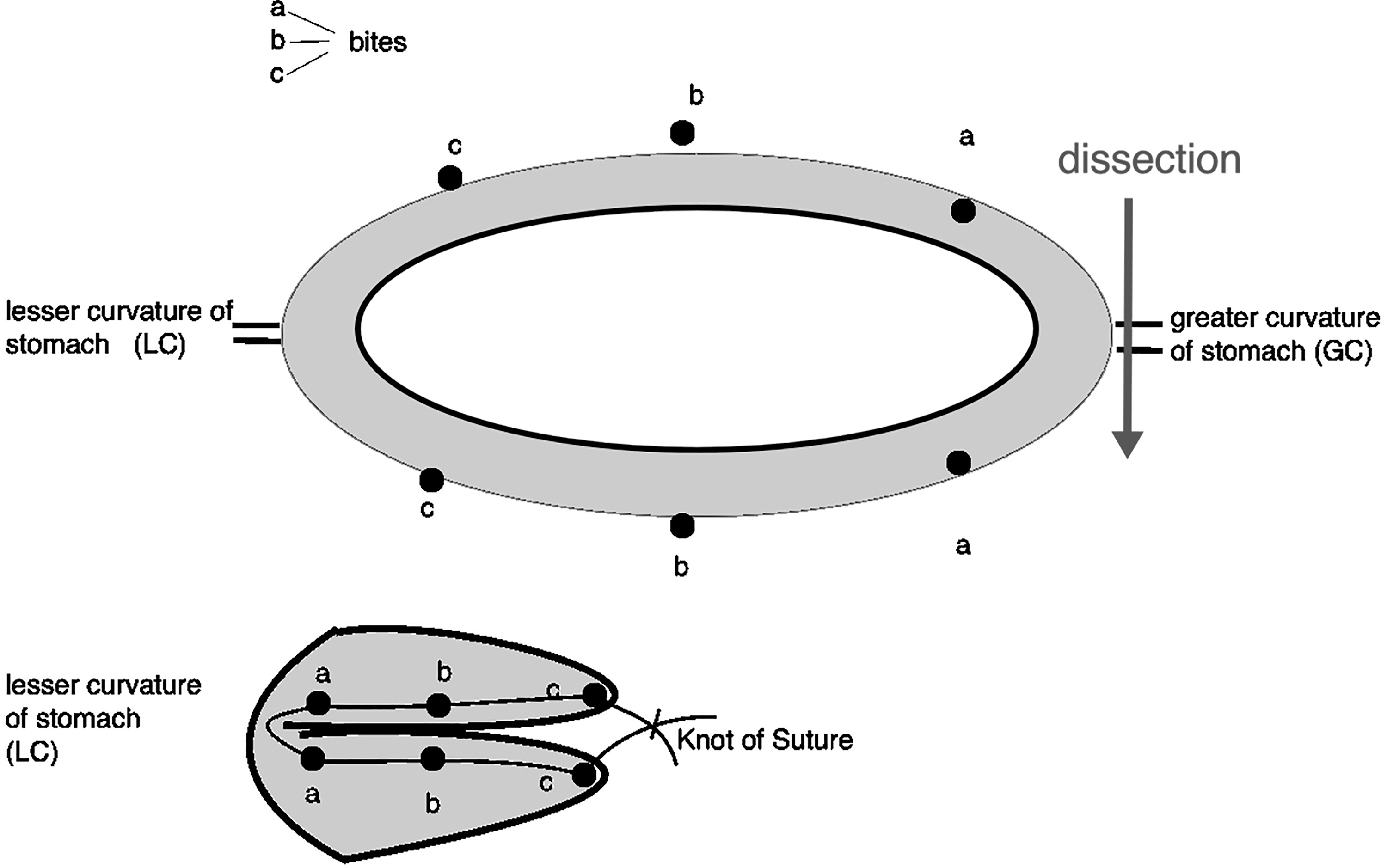
The method of 6-bit interrupted gastric sutures for obstructive gastroplication.
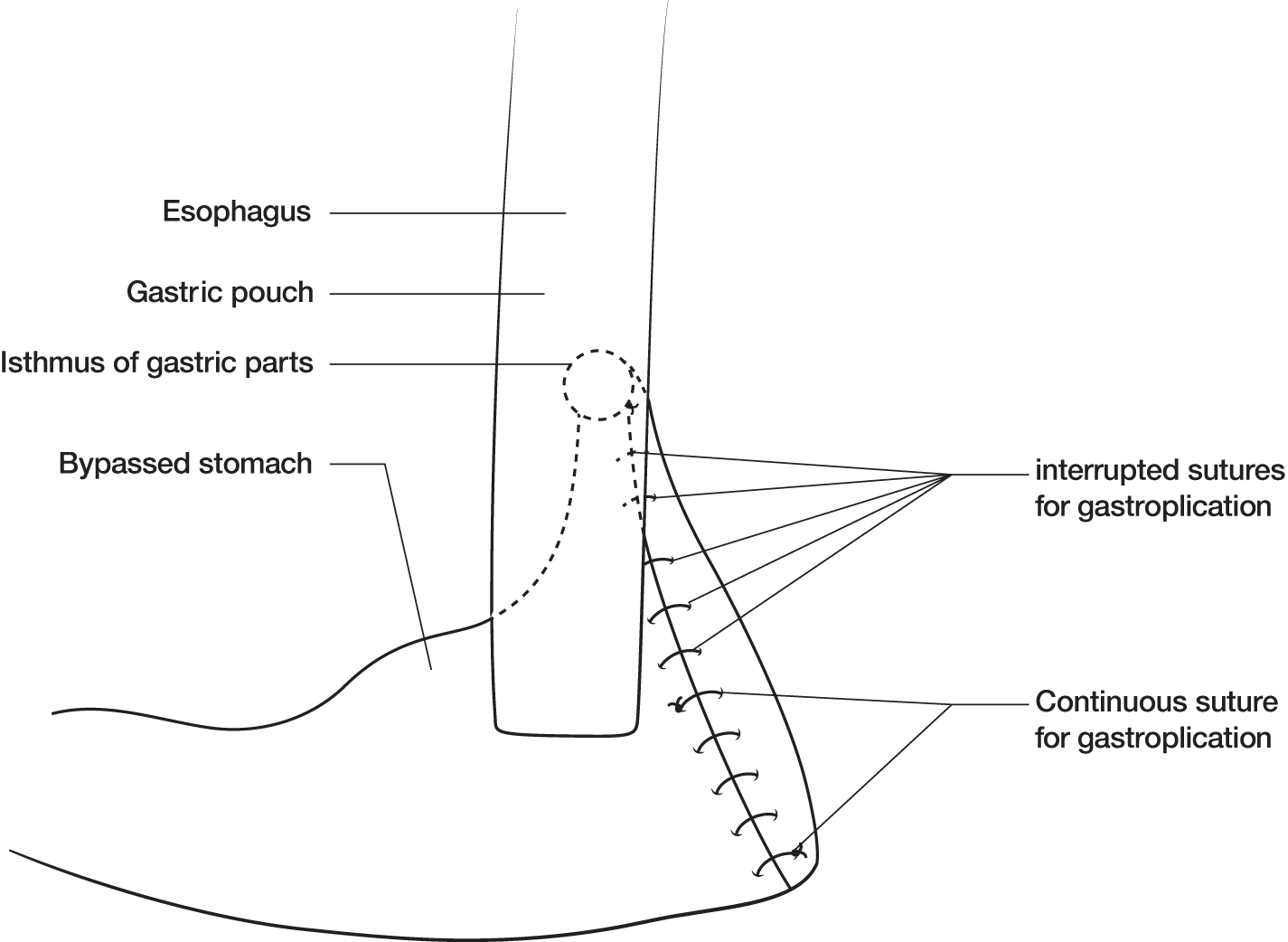
The obstructive gastroplication for uncut gastric pouch is completed.
With the transverse colon and greater omentum in a turned-up position, a suitable small intestinal limb was chosen for the connection to the gastric pouch, without tension in the antecolic position. A jejunal loop was selected, measuring ∼150 cm (BMI <40 kg/m2) to 200 cm (BMI >40 kg/m2), from the ligament of Treitz. The side of the jejunal loop was anastomosed to the gastric pouch using an “end-to-side” technique (Fig. 8). A two-layered hand-sewn gastrojejunostomy with a 2 cm stoma was created using Vicryl USP 2-0 (Ethicon US, LLC) absorbable sutures.
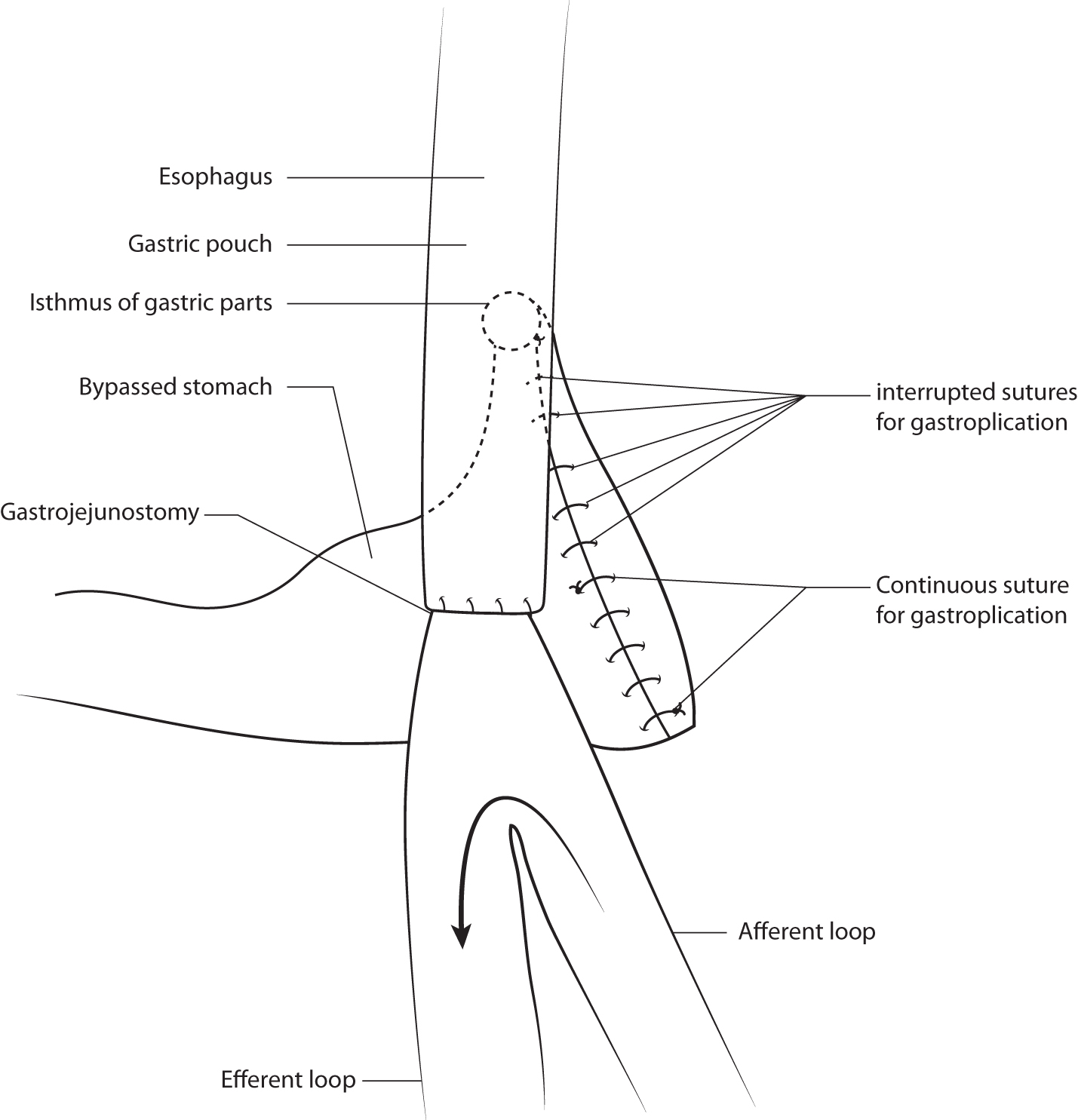
The final aspect of the hand-sewn gastrojejunostomy in an omega disposition.
The gastroenteroanastomosis was then tested with air insufflation and methylene blue using an orogastric tube. The port sites were closed using standard closure techniques. A drainage tube was inserted into the abdominal cavity near the gastroenteroanastomosis in each patient, for 1 day to assess bleeding.
Statistical analysis
Statistical analysis was performed using Microsoft Excel for Mac (Microsoft Corp., Redmond, WA) and StatPlus: Mac Pro (AnalystSoft Inc., Walnut, CA). Using power calculation for the trial focusing on the sample size criteria, a test was performed to determine whether a statistically sufficient number of patients were studied to draw safe conclusions based on this new technique. A normality hypothesis test (Kolmogorov–Smirnov) was performed to examine whether the observations followed a normal distribution.
Continuous variables are presented as mean ± standard deviation, and were analyzed using the independent samples t-test or paired samples t-test, as appropriate. We used the 2 × 2 table analysis command to calculate the following statistics for 2 × 2 contingency tables (χ 2 2 × 2, tabulated data). Categorical variables are presented using values and percentages, and were analyzed using Fisher's exact test. Statistical significance was set at 0.05, and all tests were two-tailed.
Results
No mortality or serious complication occurred in either group. The characteristics of the patients at baseline and during surgical procedures are given in Table 1.
Characteristics of the Patients at Baseline and Surgical Procedures
Fisher's exact test.
Independent samples t-test.
BMI, body mass index; F, female; LOAGB-OSPAN, laparoscopic one-anastomosis gastric bypass with an obstructive stapleless pouch and anastomosis; LOAGB-SU, laparoscopic one-anastomosis gastric bypass with stapler use; M, male.
The duration of the bariatric procedure was 74.68 ± 21.71 min in group 1, versus 85.5 ± 19.2 min in group 2 (p = 0.051). There were no conversions or serious postoperative complications. The patients in group 1 were discharged on postoperative day 2.88 ± 1.77, and on day 3.57 ± 1.18 in group 2 (p = 0.04).
One-year follow-up of postoperative weight loss and % total weight loss are given in Table 2. The ΔBMI in groups 1 and 2 showed good results 12 months postoperatively: a decrease of 12.13 (8.34–15.93) and 16.04 (11.7–20.37) from baseline, respectively (p = 0.001 in both groups). However, %TWL in group 2 was greater than that in group 1 (p = 0.01). This is owing to the increased baseline BMI in group 2, 45.91 ± 5.5 kg/m2 versus 39.88 ± 5.8 in group 1 (p = 0.01).
One Year Follow-Up of Postoperative Weight Loss
TWL, total weight loss.
Early and late postoperative adverse events/complications are given in Table 3.
Adverse Events
2 × 2 Table analysis (tabulated data).
In the early postoperative period for group 1, one patient with abdominal pain required analgesics for >3 days, and one patient with nausea and emesis required hydration. These two adverse events were associated with obstructive gastroplication, as these events were not observed in the other group.
In the late postoperative period for group 2, there were six cases of bile reflux with gastritis, versus one case in group 1 (p = 0.037, χ 2 = 4.33). When comparing the number of adverse events between the two groups, the difference was not significant (p = 0.07, χ 2 = 3.13).
The treatment plan for bile reflux included: quitting smoking, abstaining from alcoholic beverages, eating more frequent fractional meals, reducing fatty food intake, and avoiding lying down after meals. There were no severe cases of bile reflux that did not respond to nonsurgical treatment.
At 12 months postoperative, esophagogastroduodenoscopy showed that all patients in group 1 had durable gastric folds of obstructive gastroplication. There were no patients with partially or totally disrupted gastric folds.
A cost-minimization analysis of the two surgical methods of gastric bypass showed an average cost reduction of $2511.91 (62.78%) when using the stapleless technique (the stapleless mini-gastric bypass method amounted to $1488.81, vs. $4000.72 when using the stapler method).
Discussion
The International Federation for the Surgery of Obesity and Metabolic Disorders commissioned a task force to determine if mini gastric bypass—one anastomosis gastric bypass—is an effective and safe procedure, and if it should be considered a surgical option for the treatment of obesity and metabolic diseases. 8
Attempts to perform a gastric bypass without staples over a 15-year period have been limited, and have not led to widespread use of this technique, owing to both insecurity and questionable economic benefits. Cutting the stomach wall with the LigaSure (Covidien) and the subsequent suturing makes stapleless gastric bypass more technically complex and dangerous than the staple method of gastric bypass. 3
This complexity subsequently led to the search for a new method in stapleless gastric bypass.
The use of an adjustable band to create a band-separated gastric pouch can lead to erosion of the band, and can also be expensive. 9
The use of a nonadjustable band can be complicated if a leak develops between the created gastric pouch and the larger bypassed portion of the stomach. Therefore, it was proposed to supplement the bypass operation with obstructive gastroplication. 4
However, a study involving a series of cases was not sufficiently conclusive. For a more objective assessment of the results, a comparison of stapler use (LOAGB-SU) and stapleless gastric bypass (LOAGB-OSPAN) in a randomized controlled study was required.
The results of this study revealed a relatively identical technical complexity of the two operations, which is evidenced by the insignificant difference in the duration of the operation. In terms of weight loss, we obtained conflicting results. BMI after intervention did not differ significantly between the two groups. However, %TWL was better in group 2 a year postoperative. We associate this with a significant difference in BMI before surgery, despite the randomized distribution of patients into two groups. It is known, however, that %TWL is always higher in patients with a larger BMI before surgery. 6
Based on this result alone, it can be argued that the “stapler use” gastric bypass (LOAGB-SU) has a better bariatric result in the 1st year after surgery.
We associated more frequent cases of biliary reflux in group 2 with a larger size gastroenteroanastomosis (4 cm) resulting from the use of staples, versus that of the hand-sewn gastroenteroanastomosis (2 cm) in group 1. In addition, the gastric pouch in group 1 had no incisions, with the exception of the site of the anastomosis, which, evidently provides a better gradient of intracavitary pressure. However, this assumption requires further evidence, acquired with the use of intracavitary pressure measurements, in a continuing study.
Two cases of protein deficiency in group 2 were caused by noncompliance with dietary recommendations, which led to insufficient postoperative nutrition in this group.
Partially and totally disrupted gastric folds are complications specific to laparoscopic greater curvature preservation procedures (LGCP). 10
The reliability of our technique, using gastroplication for stenosis and the narrowing of the stomach, is ensured by the use of five separate, interrupted nonabsorbable sutures, each of which can independently maintain a reliable stenosis of the stomach for the functioning of the gastric pouch. Thus, if at the LGCP—obstruction or gastric stenosis is a complication, then at the LOAGB-OSPAN—obstruction or gastric stenosis below gastric pouch is the main element of a properly functioning of stapleless gastric pouch.
Limitations and strengths
The primary limitations of this study are its small size and limited follow-up time. The primary strength is a unique development in the surgical technique of stapleless gastric bypass, with a randomized comparison of the results of stapled and stapleless one-anastomosis gastric bypass.
Conclusion
Both the stapleless LOAGB-OSPAN and the “stapler use” procedures reduced body weight, but the stapleless method is 62.78% cheaper. The safety and duration of efficacy can only be discussed after longer follow-up studies are conducted.
Ethic Approval
The ethics committee of the KF “UMC” has granted ethics approval for this study (May 24, 2018, approval number 5).
Footnotes
Disclaimer
Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The work was supported by the Ministry of Education and Science of the Republic of Kazakhstan, grant number AP05135241. The funder had no role in the study design, data collection, data analysis, data interpretation, or writing of the article.