
Abstract
Aim:
To determine the change in weight loss, lipid profile, and cardiovascular risk predictor (CVRP) in moderately, morbidly, and super obese patients who underwent laparoscopic sleeve gastrectomy (LSG).
Subjects and Method:
A total of 115 patients who diagnosed as moderately (n = 35), morbidly (n = 60), and super obese (n = 20) underwent LSG, and followed up were evaluated retrospectively. The anthropometric measurements of the patients were evaluated four times: Preoperative, 0–4 months, 5–12 months, and after 1 year. Biochemical findings were evaluated twice as the first and last evaluation.
Results:
In this study the median percentage of excess weight loss (%EWL) was 77.9% (12.4–214.7), and median percentage of excess BMI loss (%EBL) was 83.3% (34.9–130.9) after 1 year. Total cholesterol and triglyceride levels decreased significantly in morbidly obese patients (p = 0.01, p = 0.02, respectively). C-reactive protein was greatly reduced in moderately obese patients (p = 0.01). Alanine aminotransferase levels improved in moderately and morbidly obese patients after 1 year (p = 0.01, p = 0.002). CVRP decreased significantly from 3.2 to 2.4 after 1 year in all patients (p = 0.04). There was a negative correlation between %EBL (r = −0,857, p = 0.01), percentage of total body weight loss (r = −0.786, p = 0.03), and CVRP in moderately obese patients.
Conclusion:
In conclusion, we observed that LSG appears to reduce lipid profile and CVRP in moderately and morbidly obese patients in our study.
Introduction
Obesity is the most important health problem of this century due to its high prevalence and consequences. It is estimated that ∼1/3 of adults living in developed and developing countries are overweight and 1/3 are obese. 1 Globally, the numbers of patients with obesity are persistently rising, with a particularly rapid increase over the last two decades. Worldwide obesity has nearly tripled since 1975. In 2016, more than 1.9 billion adults, 18 years and older, were overweight. Of these over 650 million were obese. The World Health Organization reports warn that 23% of the ischemic heart disease burden and 44% of the diabetes burden are attributable to overweight and obesity. 2
Nonsurgical weight loss methods, such as exercise, medical treatment, and diet, are rarely successful in morbidly obese patients, and the weight loss is often not maintained. In contrast, long-term weight loss is possible with bariatric surgery.
Morbid obesity is often accompanied by diseases such as type 2 diabetes (T2DM), hypertension, hyperlipidemia (HL), and cardiovascular diseases (CVDs). In fact, obesity is an independent risk factor for CVD, and it is associated with an increased risk of morbidity and mortality and is associated with reduced life expectancy. 3 Reducing the CVD risk constitutes a primary public health imperative, and weight loss is the most effective strategy to achieve this goal. Bariatric surgery is an efficient and long-lasting strategy of weight loss, improves obesity-associated comorbidities, and reduces cardiovascular mortality. 4 In obese patients undergoing bariatric surgery, weight loss, improvement in comorbidity, and a reduction in complications have been shown.5–8
Laparoscopic sleeve gastrectomy (LSG) is one of the most frequently performed bariatric surgery interventions because of its safety and efficacy. 9 Several studies have focused on percentage of total body weight loss (%TWL), as well as obesity-related comorbidities (T2DM, dyslipidemia, steatohepatitis), after LSG and have reported significant improvements in obese patients at 1 year after surgery.10–12 Nevertheless, concerns have been raised on its detrimental effect on patient nutritional state that can ultimately lead to the loss of fat-free mass (FFM). 9 The aim of weight loss in obese subjects is loss of fat mass, but inevitably a proportion of weight loss is fat free.
Bariatric surgery, which provides the greatest sustained weight loss, may arguably be of greatest concern in loss of the FFM. In addition to significant caloric restriction, bariatric surgical methods can cause malabsorption, malnutrition, and changes to gastrointestinal hormone levels. 13 All bariatric procedures cause FFM loss to a certain extent. Furthermore, the postoperative restricted nutritional program, especially the difficulty experienced by many patients in achieving the recommended daily protein intake of 1.5–2.1 g/kg ideal weight, is concerning because protein malnutrition can further worsen FFM loss. 9
There is a general consensus that obesity is an eminently inflammatory process. Recently there has been rising interest in the role of inflammation in the morbidly obese. 14 The inflammatory response to obesity might have both beneficial and harmful effects, depending on the stage and degree of obesity. Obese subjects with the same body mass index (BMI) have been shown to develop heterogeneous phenotypes that could be differently associated with cardiovascular (CV) risk. In particular, some overweight and obese patients may even show a better prognosis compared with leaner ones, a phenomenon known as “obesity paradox.” 15 However, there is limited study in the literature regarding whether there is a difference in these parameters according to the degree of obesity of patients. The aim of this study was to determine the change in weight loss, lipid profile, and cardiovascular risk predictor (CVRP) in moderately, morbidly, and super obese patients who underwent LSG.
Materials and Methods
In this study, a total of 115 patients who were admitted to the General Surgery outpatient clinic, diagnosed as obesity, underwent LSG, and followed up were evaluated retrospectively. LSG was performed under a 36-Fr calibration bougie as previously described. 16 All surgeries had been performed by the same surgeon who had been working at the surgery clinic. Descriptive characteristics, anthropometric measurements (height, weight, BMI), body analysis measurement results (fat/muscle kg and the percentage of total body weight loss (%TWL), the percentage of excess weight loss (%EWL) and the percentage excess BMI loss (%EBL), obesity related comorbidities serological tests (glucose, HbAC1, blood lipid profile, CVRP (triglyceride/HDL cholesterol ratio), 13 liver enzymes, C-reactive protein (CRP), calcium, magnesium, 25-hydroxy (25-OH) vitamin D levels) were evaluated.
CVDs are the leading causes of death and disability-adjusted life years related to high BMI. Different multivariable models are used to assess CVD risk. In this study we used the ratio of triglycerides to high-density lipoprotein-cholesterol (HDL-cholesterol), which has demonstrated to be a strong predictor of myocardial infarction.4,13,17
Diabetes was defined as currently taking diabetes medication or having HbA1c ≥6.5%. Prediabetes was defined as HbA1c between 5.7% and 6.4% without the use of medications. 18 HL was defined as currently taking a lipid lowering medication or LDL ≥160 mg/dL and high triglycerides as fasting level of ≥200 mg/dL. Abnormal liver enzymes were defined by alanine aminotransferase (ALT): >30 IU/L for men and >19 IU/L for women. 19
Biochemical findings and anthropometric measurements were evaluated retrospectively using computer database records and patient files throughout the previous 1-year period. The anthropometric measurements of the patients were evaluated four times: Preoperative, 0–4 months, 5–12 months, and after 1 year. Biochemical findings were evaluated twice as the first and last evaluation, and statistical analyses were performed using these findings. The final serologic measurements taken were average postop 19 months.
Clinical examination and nutritional evaluation were performed in a multidisciplinary manner (by a surgeon and a dietitian) for all the patients included in the study. The operation was approved and planned for those with BMI >40 kg/m2 or BMI >35 kg/m2 along with a significant medical condition associated with obesity and showing the minimum counter indication for surgery in terms of medical, dietary, or psychological aspects. 20 For further evaluation BMI classification is designated as BMI 35–39.9 kg/m2 class II (moderate) obesity, class III (or morbid) obesity ≥40–49.9 kg/m2, and super obesity ≥50 kg/m2. 13 Based on the laboratory test results, %TWL, %EWL, and %EBL were calculated according to the guidelines from 2007. 21
Nutritional therapy in the postoperative period
The first month after bariatric surgery is the early postoperative period. Upper gastrointestinal system imaging was performed on postoperative day 1 with water-soluble contrast agents, and oral nutrition was initiated after confirming that there was no anastomosis leakage. 22 The patients were discharged on postoperative day 2 with recovery, the nutritional treatment of the patients was managed by a dietitian, and they were followed up in an outpatient clinic in 2-week intervals. In patients who returned to normal diet, follow-up with monthly controls continued until the target weight was reached.
In the first stage (first 1–2 days postoperatively), patients received clear liquids, sugar-free clear fruit juices (total 1000 mL), and glutamine-containing oral nutritional solution (ONS) (Resource Glutamine, Nestle Health Science, Switzerland) (total of 400 mL). Patients received a total of 1400 mL/day liquid food, 100 mL every hour between 08:00 and 21:00 h (25–30 mL in 15-min intervals).
In the second stage (1–2 weeks postoperatively), patients received a total of 1400–1800 mL/day liquid diet (30–60 mL in 30-min intervals), that is, skimmed milk and soup with no solid pieces in addition to clear liquid foods. During this period, the patients continued to receive 400 mL of glutamine-containing ONS.
In the third stage (3–4 weeks postoperatively), full liquid diet was started. The daily nutrition plan was set as three main meals and three snacks. Soft solid foods such as artificially sweetened yogurt, fat-free diluted yogurt drink, sugar-free pudding, low-fat plain soft cheese, egg white, boiled, blended, and filtered cereals, and vegetable and fruit puree were added to the diet. Patients were not given ONS during this period.
At the fourth stage (weeks 5–6 postoperatively), a puree/soft diet was started. In this period, lean cottage cheese, whole eggs, meat, red lentils, white bread, plain biscuits, and breadsticks were added to the diet in addition to the full liquid-soft diet. The fifth stage is the normal diet period. From the seventh week onward, patients were given soft low fiber diet for 2 months. The daily diet plan was arranged as 4–6 meals/day (1400–1800 mL).
According to the postoperative first month blood values, daily vitamin and mineral supplement was provided: iron (325 mg/day), vitamin B12 (500 mg/day), calcium carbonate or citrate (1000 mg/day), and vitamin C (500 mg/day).
The study was approved by the Scientific Research and Publication Board Ethics Committee of the “[removed for blind peer review]” University (#80706068.02–050/22 and date: 25/09/2019/38).
Statistical analyses
The data obtained in the study were evaluated using SPSS 15.0. Proper descriptive values are given for qualitative and quantitative variables. Qualitative variables are expressed as number (n) and percentage (%), and quantitative variables are expressed as mean and standard deviation (
Results
A total of 115 patients were included in the study, 32 males and 78 females with a median age of 42.5 years (18–70). The comorbidities of obesity we assessed were: T2DM, HL, and steatohepatitis. Preoperatively T2DM was present in 12.2% (n = 49) (prediabetes 42.6% (n = 14)) of the patients, HL in 38% (n = 33), and steatohepatitis in 65.2% (n = 75). All the patients with T2DM, HL, and steatohepatitis were under pharmacological therapy with an acceptable control of their comorbidities. According to preoperative BMI, 30.4% (n = 35) of the patients were moderately obese, 52.1% (n = 60) were morbidly obese, and 17.3% (n = 20) were super obese. Demographic and anthropometric characteristics of the patients are shown in Table 1.
Preoperative Demographic and Anthropometric Findings of the Patients
*p < 0.05.
**p < 0.001, nonparametric Mann–Whitney U test.
Postoperative body analysis measurements and weight loss follow-up
During the 12 months and after follow-up we observed a statistically significant reduction of BMI, body mass, fat mass, muscle mass, and significantly increased %TWL, %EWL, and %EBL in all groups (p = 0.001). In this study, the mean preoperative BMI was 43.5 + 6.4 kg/m2, and after 1 year mean BMI was 31.4 + 5.5 kg/m2 (p = 0.001). The median %EWL was 77.9% (12.4–214.7), and median %EBL was 83.3% (34.9–130.9) after 1 year. The overall success rate after the first year was 72.1% for BMI <35 kg/m2. At the end of the follow-up period, according to BMI, 13% (n = 15) of the patients were normal, 31.3% (n = 36) were overweight, 28.7% (n = 33) were class 1 obese, 20% (n = 23) were moderately obese, 7% (n = 8) were morbidly obese, and there was no patient in the super obesity group.
The results of weight loss measurements of moderately, morbidly, and super obese patients are shown in Table 2. The changes between groups after a year were statistically different in %TWL (p = 0.002), %EWL (p = 0.007), and %EBL (p = 0.002). The fat mass (kg) was higher in super obese patients than the fat mass of morbidly (p < 0.001) and moderately obese patients after 12 months. %EWL was lower in super obese patients than the %EWL of morbidly (p < 0.001) and moderately (p < 0.05) obese patients, and %EBL was lower in super obese patients than morbidly (p < 0.001) and moderately (p < 0.001) obese patients.
Body Analysis Measurements and Weight Loss Follow-Up of the Patients in and After 1 Year
p < 0.001 difference from moderate to morbid obesity Mann–Whitney U test.
p < 0.001 difference from morbid to super obesity Mann–Whitney U test.
p < 0.001 difference from moderate to super obesity Mann–Whitney U test.
p < 0.001, nonparametric Friedman test.
p < 0.05 difference from moderate to super obesity Mann–Whitney U test.
p < 0.05.
p < 0.001, nonparametric Kruskal–Wallis test.
Changes in serological tests after LSG
Pre- and postoperative determinations of serological tests of moderately, morbidly, and super-obese patients showed that the results were similar between groups. The evaluation of the serological test at the end of the follow-up period showed that there was a statistically significant decrease in fasting blood glucose in all groups (p = 0.01, p = 0.001, p = 0.01, respectively). Total cholesterol and triglyceride levels decreased significantly in morbidly obese patients (p = 0.01, p = 0.02, respectively). Chronic low-grade inflammation, as assessed by acute-phase CRP, was greatly reduced in moderately obese patients (p = 0.01). Similarly, the increased blood levels of ALT that reflect liver abnormalities (such as steatosis or steatohepatitis) improved in moderately and morbidly obese patients after 1 year (p = 0.01, p = 0.002). Pre- and postoperative determinations of serological test are described in Table 3.
Improvement in Pre- and Postoperative Serological Tests After 1 Year
**p < 0.001, nonparametric Wilcoxon test.
: not significant, nonparametric Kruskal–Wallis test.
In all patients there was a positive correlation between BMI (kg/m2) and serum triglyceride levels (r = 0.320, p = 0.03) and a negative correlation between %TWL and serum glucose levels (r = −0.508, p = 0.001) (Fig. 1).
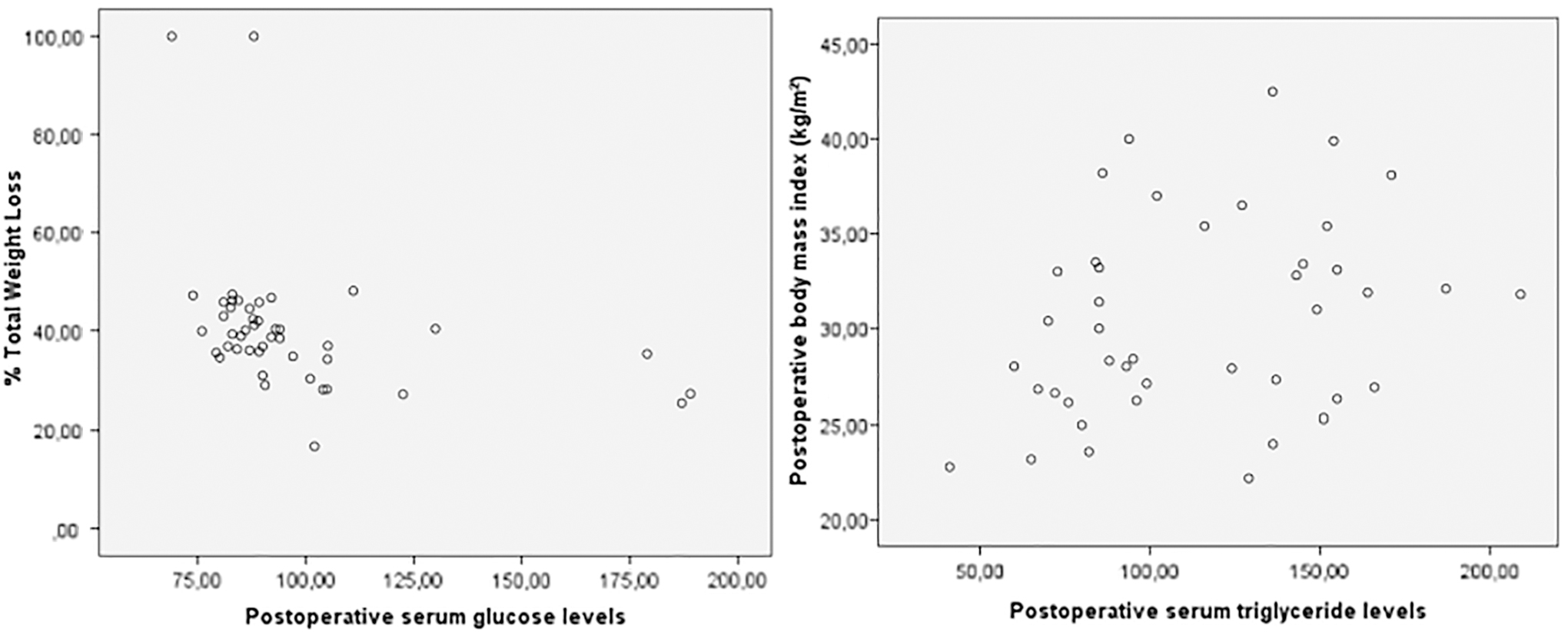
Correlation between weight loss parameters and biochemical findings in all groups.
We didn't find any correlation between serum lipid profile and %TWL, %EBL, %EWL in groups (p > 0.05). There was a positive correlation between postoperative serum HDL levels and muscle mass in moderately obese patients (r = −0.883, p = 0.008). The CVRP decreased significantly from 3.2 to 2.4 after 1 year in all patients (p = 0.04). The risk predictor did not differ between groups (p > 0.05). However, there was a negative correlation between %EBL (r = −0.857, p = 0.01), %TWL (r = −0.786, p = 0.03), and CVRP in moderately obese patients. There was a positive correlation in postoperative serum aspartate aminotransferase (AST) levels and cardiovascular risk factor in super obese patients after 1 year (r = 0.900, p = 0.03).
Discussion
In the present study, it was observed that weight loss continued in early and late follow-up of all patients in moderately, morbidly, and super obese patients who had LSG and that there was a significant decrease in the body weight of the patients. The median %EWL was 77.9% (12.4–214.7), and median %EBL was 83.3% (34.9–130.9) after 1 year. The overall success rate after the first year was 72.1% for BMI <35 kg/m2.
In the evaluation of bariatric surgical operations, the focus is primarily on weight loss, in other words, reduction of body fat tissue. 22 As a result of LSG administered in 260 morbidly obese patients, the median %EWL for the first year of follow-up was found to be 65.7%. 23 In a multicenter randomized controlled trial of 217 patients with BMI between 35 and 61 kg/m2 after LSG at the end of the 1-year period %EBL was found to be 72.3%. 24 Our results are similar to ones reported in the literature, and our results are successful in terms of weight loss targeted by bariatric surgery.
In the present study, a significant decrease in muscle mass was observed along with a decrease in fat mass. Skeletal muscle constitutes the largest protein/amino acid pool in the body, and skeletal muscle loss has important effects on health and diseases. Maintaining a certain level of muscle protein requires a balance between muscle protein synthesis and breakdown ratio. Current evidence suggests that a decrease in protein synthesis after gastric bypass surgery leads to muscle loss. This result is not surprising because a decrease occurs in optimal dietary protein intake after gastric bypass, and, unlike other macronutrients, proteins and amino acids are not stored in the body. 25
In a meta-analysis, it was shown that the loss of lean body mass in bariatric surgery performed by the LSG method was less than that occurring in other methods (biliopancreatic diversion and Roux-en-Y gastric bypass). 26 Damms-Machado et al. 27 reported FFM losses of 46.1% and 25.4% at 3 and 12 months LSG, respectively. It is known that rapid weight loss after bariatric surgery causes loss of lean body mass and a decrease in muscle mass. Most obese patients experience moderate fluctuations in body weight and loss of lean body mass as a result of prolonged restrictive or inappropriate diets. Sedentary lifestyle due to obesity can amplify the loss of lean body mass and lead to impaired muscle function. Bariatric surgical procedures may also cause malnutrition. 28 Protein is needed to prevent protein malnutrition caused as part of general malnutrition. Therefore, the necessity for powder protein is included in the guidelines. 29
Modifying the existing dietary practices to increase the uptake of essential amino acids is an approach that can potentially prevent the loss of lean body tissue, resulting in more permanent health levels in patients who underwent bariatric surgery. 25 In the present study, we aimed to provide glutamine supplemented nutritional therapy to patients in the first and second postoperative stage to ensure adequate protein intake. Bariatric surgery is a multidisciplinary process in which dietary counseling is an important part. Before the operation, the dietician will ensure that a restrictive or hypocaloric diet is not continued. 28 Protein intake should be at least 60 g/day, and we provided this requirement. 30 However, we couldn't evaluate the effect of glutamine supplemented nutritional therapy in this study due to the absence of a control group.
After 1 year we found that BMI was positively correlated with serum triglyceride levels, and %TWL was negatively correlated with fasting glucose levels in our study population. It is known that elevated triglyceride levels are an independent risk factor for coronary heart disease (CHD). 31 In 1996, Hokanson and Austin evaluated the independent role of plasma triglyceride as a risk factor for CHD in a meta-analysis of 17 population-based prospective studies. 32
As expected we obtained a significant improvement at the end of the follow-up period in fasting glucose in all groups. Total cholesterol and triglyceride levels decreased significantly in morbidly obese patients in our study population. The changes in lipid profile were not statistically significant in moderately and super obese patients. However, there was a negative correlation between %EBL, %TWL, and CVRP only in moderately obese patients. Iannelli et al. 33 showed that 1 year after surgery, Roux-en-Y gastric bypass was equally effective at reversing metabolic syndrome, inflammation, and insulin resistance in morbidly obese and super-obese women. Hady et al. 34 showed that LSG leads to the improvement of metabolism of insulin, glucose, cholesterol, and triglycerides in obese patients. However, obesity classification was not performed in this study.
“Obesity” itself is a disease that affects cardiac functions. Excess weight is associated with many important CVDs, not only CHD but also abnormalities in heart rate and ventricular function. This association is due to multiple mechanisms, including hypertension, diabetes mellitus, or dyslipidemia. The diagnosis of obesity should include measurements of total body fat content and its distribution. 35 The adipose tissue is not simply a passive storehouse for fat but an endocrine organ that is capable of synthesizing and releasing into the bloodstream an important variety of peptides and nonpeptide compounds that may play a role in cardiovascular homeostasis. 3
Obesity is also associated with a state of systemic low-grade inflammation, as shown by increased plasma levels of C-reactive protein (CRP), a marker of inflammation. In turn, CRP has been reported to be an important indicator of cardiovascular risk. 36 Our data confirm those reported by others and show a significant improvement in inflammatory markers 1 year after bariatric surgery.14,37
Chronic low-grade inflammations, as assessed by acute-phase CRP, were greatly reduced in moderately obese patients. Similarly, the increased blood levels of ALT that reflect liver abnormalities (such as steatosis or steatohepatitis) improved in moderately and morbidly obese patients after 1 year. We thought that the reduction in serum triglyceride in morbidly obese patients and the correlation between CVRP and %EBL and %TWL in moderately obese patients are related to the fat mass. After 1 year the fat mass was similar between moderately and morbidly obese patients. Super-obese patients had a higher fat mass than moderately and morbidly obese patients and a lower %EBL and %EWL in our study, and there was a positive correlation in postoperative serum AST levels and cardiovascular risk factor in super-obese patients.
The most important limitations of this study are that the changes in the nutritional treatment processes (nutritional requirements according to the needs of patients and the compliance of patients with diet) of these patients could not be determined in detail because the study was conducted retrospectively and that the patients could not be evaluated individually. Randomized controlled prospective studies with more participants are warranted.
In conclusion, in the present study, it was observed that the continuation of early and late weight loss was achieved, and there was a decrease in the results of serum triglyceride and fasting glucose levels in all patients undergoing LSG. LSG appears to reduce lipid profile and cardiovascular risk factor in moderately and morbidly obese patients in our study.
Footnotes
Authors' Contribution
B.G.A. made important intellectual/conceptual critical corrections for preparation of the content for the study that is ready for publication.
E.P. provided important contributions to conceptual or planning stages of the study and collection of the data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.