
Abstract
Background:
Any deterioration in pyloric muscle activity has the potential to influence gastric emptying. In such a case, gastric emptying time would also be changed due to the paralysis of pyloric muscles, which is the botulinum toxin's effect mechanism. This study aimed to investigate how the pyloric orifice structure influences the success of intragastric botulinum toxin type A injection (GBI) therapy in Class I–II obese patients for weight loss.
Methods:
The GBI applied patients were categorized according to pyloric orifice structure during upper gastrointestinal system endoscopy: Group A: the patients whose pylorus had normal peristaltic activity and closed completely and Group B: the patients whose pylorus did not close properly or were nonperistaltic. We measured the body mass index (BMI) of the patients before and 6 months after the procedure and expressed postprocedure weight loss in terms of the percentage of excess BMI (E-BMI%) loss. We compared preprocedure and sixth-month BMI and E-BMI% values. We applied the Student's t-test to analyze the differences among study groups, and p < 0.05 was accepted as statistically significant.
Results:
Seventy-seven patients completed the 6-month follow-up period. The measurements without considering the pyloric orifice structure showed that the mean BMI decrease in female patients (from 36.4 ± 5.4 to 32 ± 7.2 kg/m2) was significant (p < 0.05). And the BMI and E-BMI% loss in Group A were statistically significant (p < 0.05).
Conclusion:
We advise being selective and applying GBI to class I–II obese patients with normal pyloric orifice structure.
Introduction
The prevalence of obesity has doubled globally in the last four decades to the extent that nearly one-third of the world population is now classified as overweight/obese. 1 Obesity causes adverse impacts on almost every physiological system in the human body and comprises an important public health problem. It is associated with an increased risk of many developing co-morbid conditions, such as diabetes mellitus, cardiovascular disease, several types of cancers, musculoskeletal disorders, and poor mental health. 2
Current treatment options for patients with obesity include lifestyle intervention, obesity pharmacotherapy, and bariatric surgery. 3 The components of lifestyle intervention involve diet, exercise, and behavior modification and should be recognized as the cornerstone of any obesity treatment method 4 ; however, the impact of lifestyle intervention is limited in patients with morbid obesity.
Surgical therapies with laparoscopic approach are accepted as the most effective and persistent obesity treatment methods, with a significant reduction in complication rates and postoperative recovery. 5 Gastric banding, sleeve gastrectomy, Roux-en-Y gastric bypass, and biliopancreatic diversion are commonly performed bariatric surgical procedures worldwide. 6 However, the idea of scarless methods in which the video-endoscopy device is used as the primary carrier device, expecting to achieve results at least as good as laparoscopic procedures, has significantly developed within the last decade. In addition, the development of effective and safe, newer endoscopic bariatric procedures provides another adjunctive treatment for patients with obesity, who cannot handle this disease with lifestyle modification alone or who is not a candidate for surgical procedures. Endoscopic therapies, such as intragastric balloons, duodenojejunal bypass liners such as the EndoBarrier, and endoscopic suturing platforms, have also become proposed alternatives to surgery, considering their minimally invasive advantages. 7 However, given the lack of long-term data at present, the role of such devices continues to be determined. 6
Newly, botulinum toxin A application into the stomach has been proposed as a treatment method in obesity. 8 It impacts through acetylcholine receptors located in smooth muscle cells and suppresses stomach motility. This method aims to decrease gastric emptying time and thus to extend the duration of feeling full. 9 This effect of intragastric botulinum toxin A injection (GBI) makes it easier to adhere to dietary prescriptions, which is the cornerstone of any obesity treatment method. 10
Considering our endoscopic inspections and the complicatedness in literature results, 10 we thought cases that have not succeeded in losing weight after GBI might have pylorus contractility problems. Any deterioration in pylorus activity is recognized to have the potential to influence gastric emptying. 11 In such a case, gastric emptying time would also be altered due to the paralysis of pylorus muscles, which is one of the effect mechanisms of botulinum toxin A.
The pyloric orifice structure may have a crucial role in the success or failure of GBI therapy for obesity treatment, and Kanlioz and Ekici previously investigated this possible role. 10 However, we believe that the pyloric orifice structure is an important subject that necessitates being investigated more. In this study, we aim to explore whether there is a correlation between weight loss after GBI and pyloric orifice structure.
Materials and Methods
Study design
Medical records of patients who underwent GBI from June 2019 through June 2020 at the Istanbul Okan University Hospital in Istanbul were retrospectively evaluated. All patients' medical history was noted, and psychological and nutritional evaluations were assessed before GBI. In addition, complete blood count and coagulation tests were also made before the endoscopy. Demographics and body mass index (BMI) features of the individuals are shown in Table 1.
Patient Statistic Before Application of Intragastric Botulinum Toxin A
The patients who completed a 6-month follow-up period.
BMI, body mass index.
Classification according to BMI
We used the formula described by Keys et al., 12 and we applied the overweight and obesity classification scheme created by the National Institute of Health. 13
Patient selection for GBI therapy
We only involved class I obese patients and class II obese patients with no comorbidities (Class II obese patients in combination with obesity-related comorbid conditions such as diabetes mellitus, hypertension, hyperlipidemia, nonalcoholic fatty liver disease, sleep apnea, asthma, venous stasis disease, severe urinary incontinence, debilitating arthritis, Pickwickian syndrome, and class III obese patients, were consulted to a surgeon specialized in bariatric procedures). The scheme of the study is shown in Figure 1.
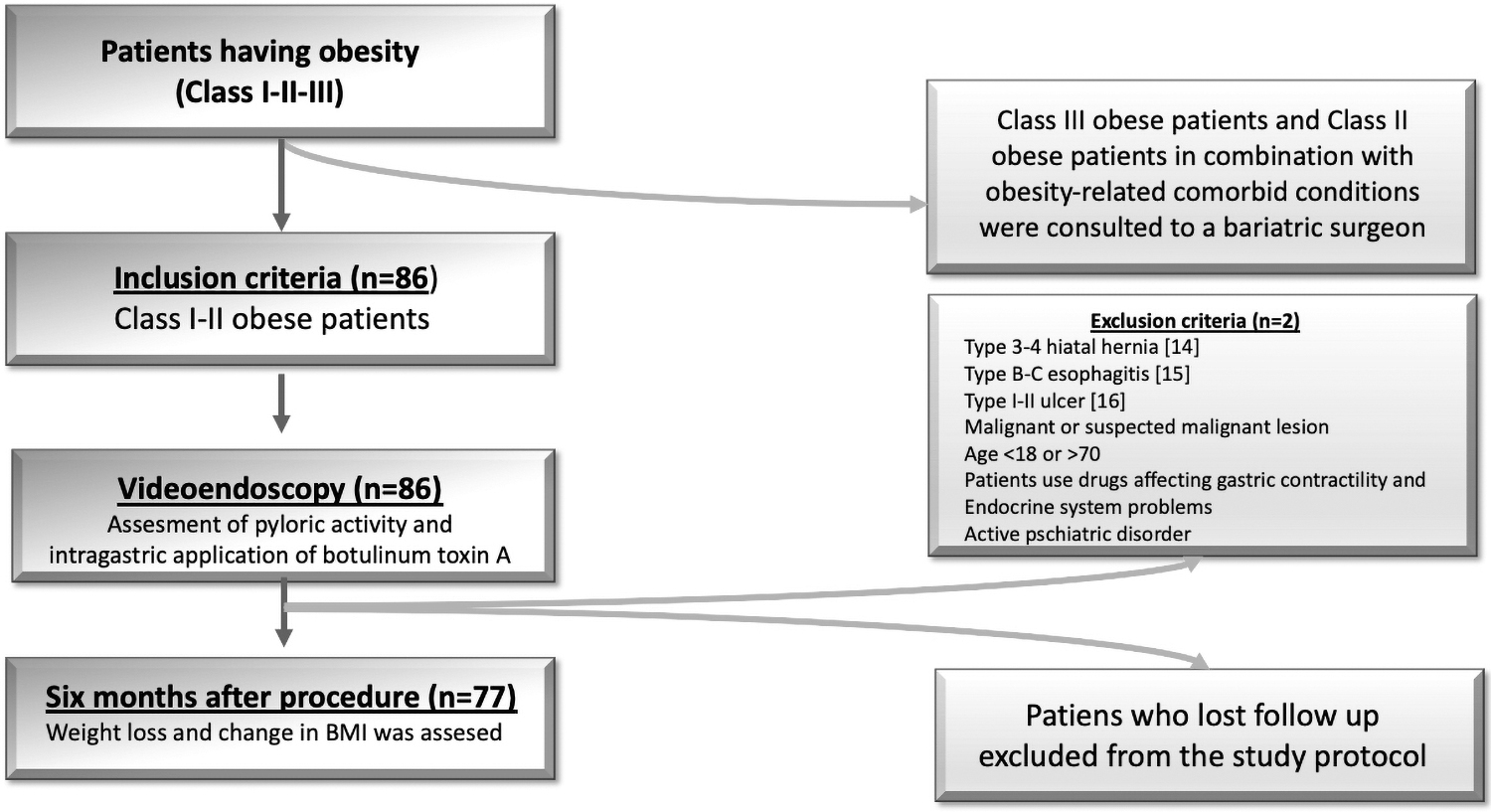
Scheme of this study.
Patients with type 3–4 hiatal hernia according to flap-valve grading system, 14 Los Angeles type B–C esophagitis, 15 type I–II ulcer, 16 malignant or suspected malignant lesion, and age <18 or >70 years, using drugs affecting gastric contractility and pyrokinesis, and who have endocrine system problems (hypothyroidism and Cushing syndrome) and active psychiatric disorder were not accepted as a candidate for GBI therapy.
The presence of gastritis was not accepted as a contraindication (in patients with gastritis, a biopsy was taken from incisura angularis, and urease test was performed for Helicobacter pylori detection. If H. pylori positive; 1000 mg amoxicillin +500 mg clarithromycin +30 mg lansoprazole, twice a day, medical treatment was given after GBI therapy. Omeprazole 40 mg once a day was given if H. pylori negative).17,18
Preparation of botulinum toxin A
Two hundred units of botulinum toxin A transported in a temperature-controlled supply chain is diluted with 10 mL % 0.9 sodium-chloride solution +0.1 mL of methylthioninium chloride (20 U of botulinum toxin A per milliliter).18,19
Preparation of the patient
The patients had 8 h of fasting period before the procedure. Ondansetron HCl (8 mg)+esomeprazole (40 mg) was intravenously administered to the patient 30 min before the toxin application to prevent postprocedure nausea and emesis.
Anesthesia technique
Before the upper gastrointestinal system endoscopy, a medical doctor specialized in anesthesiology administrated sedoanalgesia 1.5 mg/kg propofol (PROPOFOL-PF %1 200 mg/20 mL, IV; Polifarma, Istanbul, Turkey) and 0.05 mg/kg midazolam (DORMICUM 50 mg/10 mL; Deva Ilac, Tekirdag, Turkey).
Assessment of pyloric activity
The endoscopist viewed the pyloric orifice with Fujinon EG600WR video-endoscope for 1 min. If pyloric ring contraction was observed at the end of 1 min, it was accepted as normal pyloric orifice structure. If no contraction was observed for 1 min, tactile stimulation was given to the pyloric ring with the video-endoscopy device's head and remained for an extra 30 s. Endoscopists still saw no contraction despite the tactile stimulus, which was accepted as abnormal pyloric orifice structure (pylorus contraction was not seen after tactile stimulation in any patient).
Application of botulinum toxin A
After completing an upper gastrointestinal system endoscopy, 0.5 mL solution injection to the muscular layer of the gastric wall was performed at four different cardinal points (3-6-9-12 o'clock) starting 2 cm from the pyloric ring (Fig. 2) and repeated three times with a distance of about 2 cm toward incisura angularis (10 U of botulinum toxin A per injection) by using an Endo Flex needle, 2.3 mm thickness and 230 cm length (Endo Flex GmbH, Voerde, Germany). And 0.5 mL of toxin solution was also applied to the submucosal layer of the gastric wall at four different points on gastric fundus and four different points ∼2 cm above the gastric cardia (10 U of botulinum toxin A per injection) (Fig. 3). All injections were performed under the direct vision of the endoscope. Mark of methylene blue prevented repetitive injections to the same point. 18
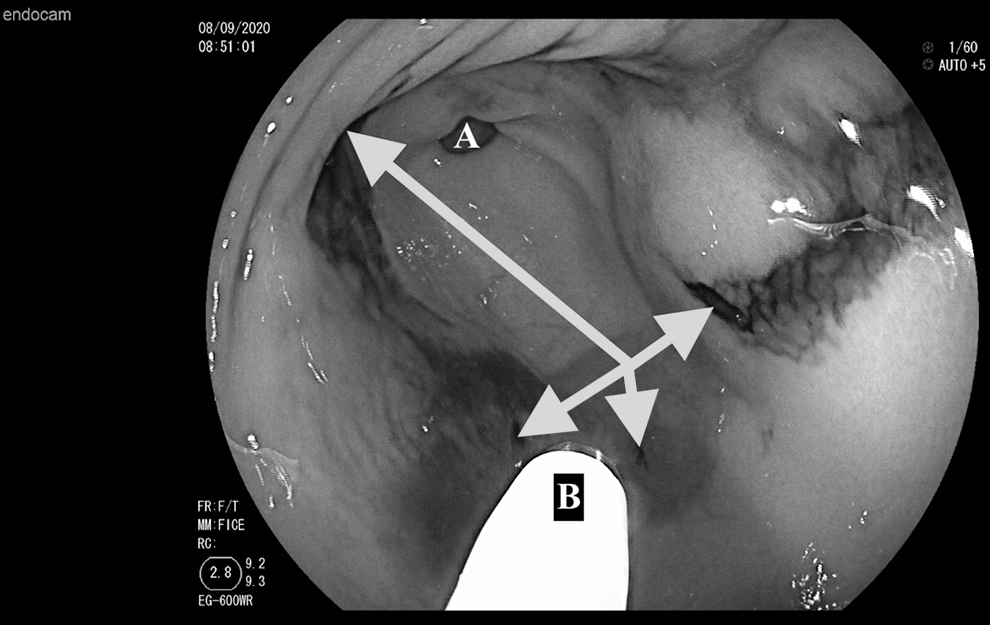
Injection of botulism toxin A to the submucosal layer of the stomach antrum at 3-6-9-12 o'clock direction, beginning 2 cm from the pyloric orifice (red arrows) (
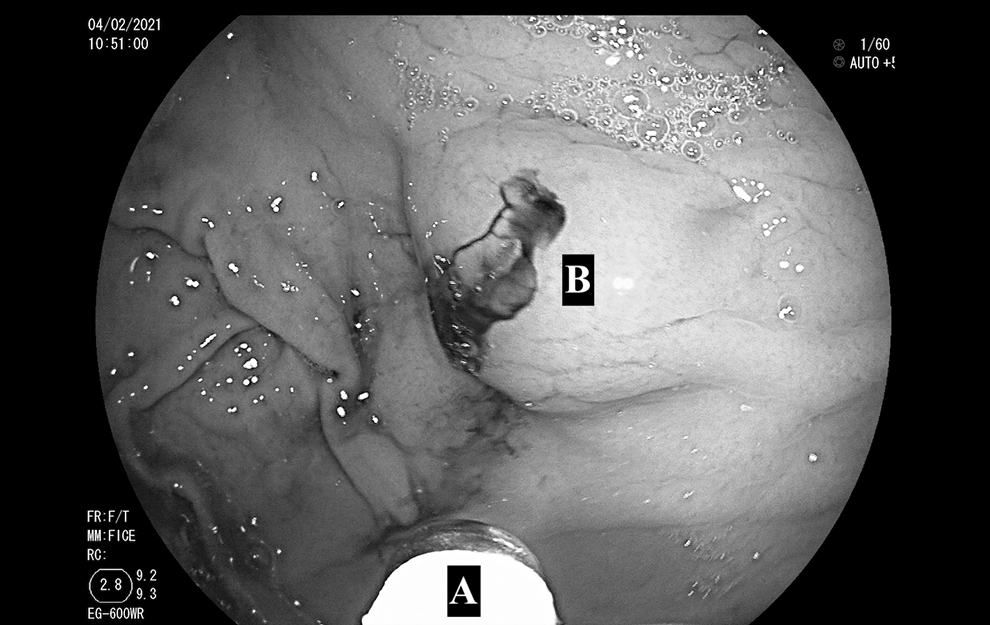
Injection of botulism toxin A to the submucosal layer of the stomach fundus (
Study groups
Eighty-six obese patients applied for GBI therapy. Following upper gastrointestinal system endoscopy, we did not apply botulinum toxin A to two patients (one had type III hiatal hernia, and one had type B esophagitis).15,16 The patients were categorized according to pyloric orifice structure: Group A: individuals who had normal pyloric orifice structure and Group B: individuals who had abnormal pyloric orifice structure.
Follow-up of the patients
All patients' vital signs (blood pressure, heart rate, and capillary SpO2) were observed for 4 h following the procedure, and patients were discharged after taking a soft-liquid diet. They were suggested to take a soft-liquid diet for the following 48 h. After the first 48 h of GBI, the liquid diet period, the patients were included in a calorie-restricting high-protein diet program specially prepared for each patient by the dietitian. After that, the dietitian followed up on the weight loss of the patients during the 6-month period.
All patients were appointed for control visits at the end of the first and sixth month. Patients who did not appear for control visits were contacted by phone call. During the follow-up period, no significant severe acute side effect, such as anaphylactic reactions, severe dysphagia, allergic reactions, cardiac arrhythmias20,21 was recorded (one patient had severe left shoulder pain for 2 days and one patient had diarrhea for 5 days, which was medically treated).
Measured variables
Preprocedure and postprocedure (first and sixth months) total body weight and BMI of the patients were noted. We assessed the weight loss and BMI change of the patients. Postprocedure weight loss was also expressed in the percentage of excess BMI (E-BMI%) loss and total body weight loss (TBWL%). The ideal weight was deemed equal to a BMI of 25. 22
Ethical approval
All procedures performed in studies involving human participants followed the Helsinki declaration and its later amendments or comparable ethical standards. This is also public on ClinicalTrials.gov (NCT04948177).
And the ethics committee of Istanbul Okan University approved the study (19.08.2020/56665618-204.01.07).
Informed consent
Informed consent was obtained from all individuals.
Statistical analysis
We used the GNU operating system-PSPP software program to record and analyze the study's obtained data. Demographic and categorical data are expressed as absolute or as frequencies. Continuous variables are presented as mean values and standard deviation. We applied the Student's t-test to analyze the differences among study groups, and p < 0.05 was accepted as statistically significant. In addition, Cohen's d is an effect size used to indicate the standardized difference between two means. If the d (magnitude) is <0.5, the effect size is considered small; if it is between 0.5 and 0.8, the effect size is medium, and if >0.8, it is considered large. 23
Results
Eighty-six obese patients applied for GBI therapy. Following upper gastrointestinal system endoscopy, we did not apply botulinum toxin A to two patients (one had type III hiatal hernia and one had type B esophagitis), and seven (8.3%) patients lost follow-up. Fifty-six (72.7%) female and 21 (27.2%) male patients completed the follow-up period (Fig. 1).
The mean BMI decreased from 36.4 ± 5.4 to 32 ± 7.2 kg/m2 in females and from 37.7 ± 7.1 to 34.8 ± 5.02 in males at the end of 6 months. The BMI change was significant in females (p < 0.05).
Also, the BMI decrease in Group A was higher than in Group B (p = 0.03) (Fig. 4). In addition, the BMI changes in female and male patients with normal pyloric orifice structure were significant (p = 0.001 and p = 0.04, respectively) (Table 2).
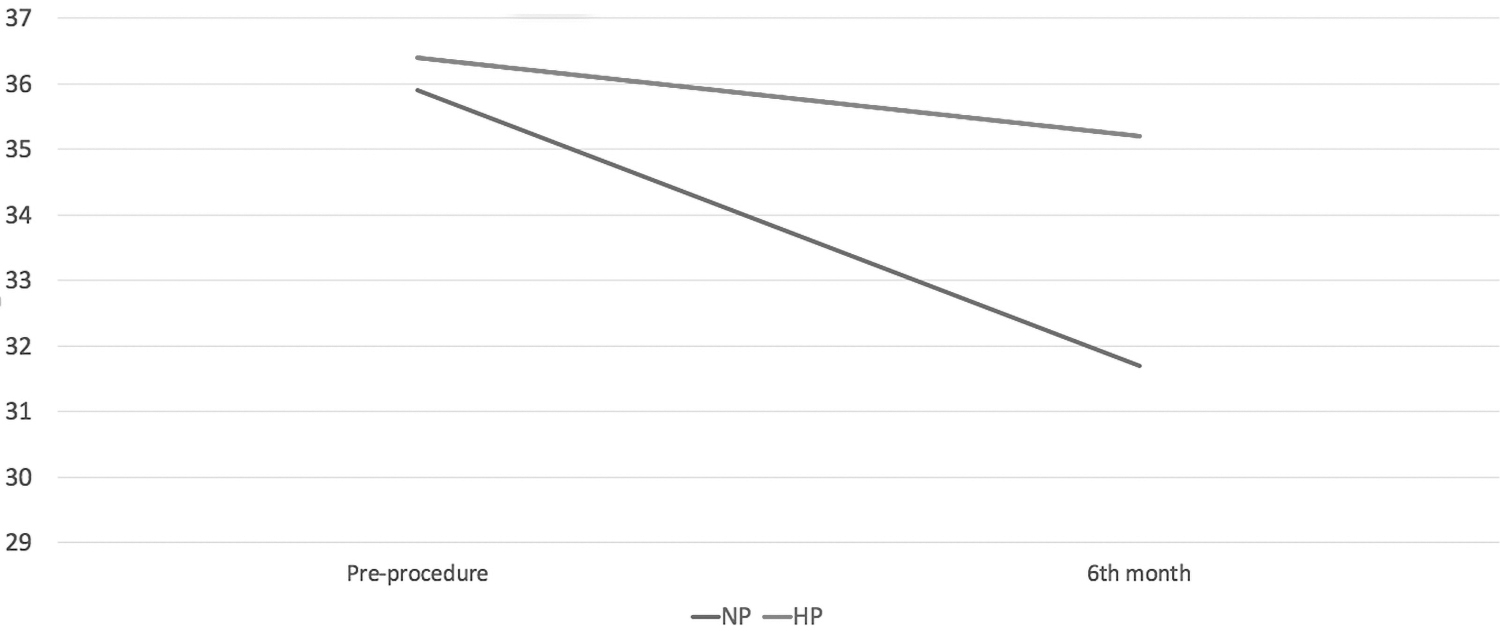
BMI loss for 6-month follow-up. BMI, body mass index.
Assessment of Results of Botulinum Toxin Type A Application in Terms of Tonus of Pyloric Orifice Continence
Student's t test.
p < 0.05, **p < 0.001.
The effect size for this analysis (d = 0.657) was found to exceed Cohen's convention for a medium effect. These results indicate that Group A (M = 35.9, SD = 7.4) experienced better weight loss following GBI treatment than Group B (M = 31.7, SD = 5.2) (Fig. 5).
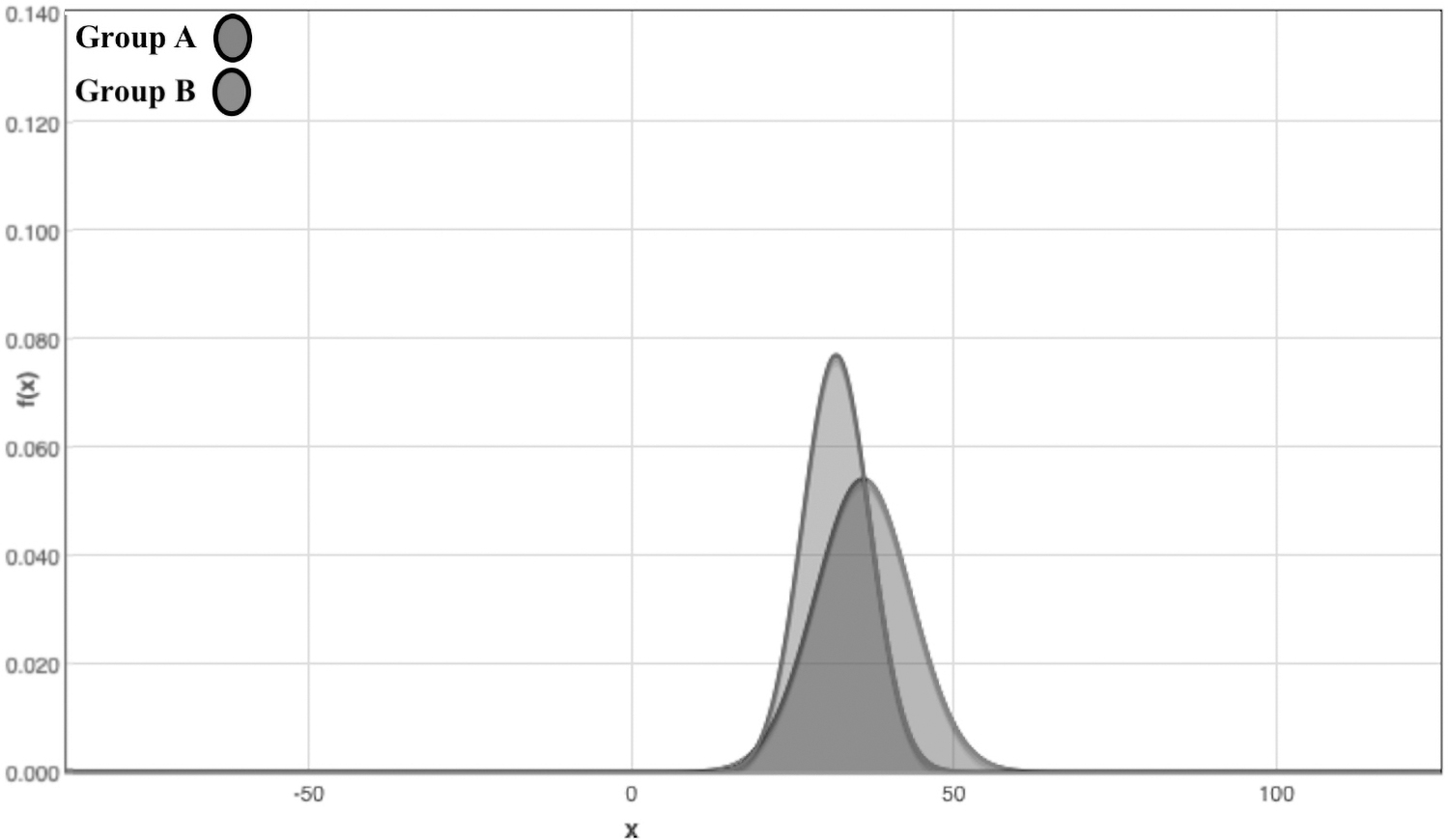
Cohen's d effect size according to BMI of groups.
The E-BMI% loss and TBWL% were significant in Group A (The mean E-BMI% loss was 39.3 ± 5.6 in Group A and 21.9 ± 5.2 in Group B, the mean TBWL% was 14.3 ± 4.1 in Group A and 11.3 ± 5.7 in Group B) (p < 0.01 and p < 0.05, respectively).
Discussion
In recent years, endoscopic botulinum toxin A injection to the stomach has become an emerging method in obesity treatment. In 2007, Foschi et al. first stated that botulinum toxin A injection had better results against the placebo group for treating obesity. 24 Following Foschi's pioneer research, various studies have been aired, supporting the botulinum toxin A application as a reliable treatment technique for obesity.10,18,19 Furthermore, this minimally invasive procedure has been widely accepted in daily practice worldwide.
As more obese patients were treated with this emerging method, more scientific studies on the subject increased. However, the inconsistency in the literature and methodological differences makes this method's effectiveness remain suspicious.
Park et al. and Li et al. set forth that GBI is an efficient technique in obesity treatment.25,26 Contrary to positive results, the meta-analysis of Bustamante et al. presented that GBI for obesity treatment did not provide a 5% loss of total body weight, which is the U.S. Food and Drug Administration's (FDA) target weight loss value for low-risk devices for bariatric procedures. 27 Gui et al. proclaimed that GBI provides no statistically notable results in obesity treatment. 28
The review of Sanchez Torralvo et al. reported that GBI might be a beneficial and reliable approach in obesity treatment. However, this review also pointed that the lack of well-designed, placebo-controlled, long-term studies with sufficient sample size is the obstacle to this promising minimal invasive technique. 29 Our previous research focused on the short-term benefits of GBI therapy combined with a low-calorie restricting- high-protein diet and showed success in weight loss and decrease in medication requirement for diabetes and hypertension. 18 Our study concluded that GBI treatment might be useful in patients with normal pyloric orifice structures. Considering this situation in new studies will reveal whether this treatment can be more beneficial in this specific patient group.
The heterogeneity in the application techniques increases suspicions about the efficiency of this method. The meta-analysis of Vargas et al., investigating five studies focusing on GBI, pointed to this problem. 30 In our previous study on GBI, we applied the toxin to both gastric antrum and fundus 18 ; however, Kanlioz and Ekici applied the toxin only to the gastric antrum, 10 and despite different application techniques, both investigations present beneficial outcomes on weight loss. Dosage variation in daily practice is another problem. Although Albani et al. used 500 UI botulinum toxin A, 31 García-Compean et al. used 100 UI of toxin, 32 and Kanlioz and Ekici applied 200 UI of botulinum toxin A. 10 The lack of standardization in concepts and application techniques has still been causing enduring questions about this promising technique.
In the scientific literature, we see that the study of Kanlioz and Ekici is the first study examining pyloric laxity and weight loss after GBI therapy. 10 Our results are consistent with Kanlioz and Ekici, but their injection technique is different from our study. This difference in practice brings us back to the issue we highlighted before; there is still no consensus about the intragastric botox application method.
In essence, this study shows that GBI in class I–II obese patients, who do not have normal pyloric orifice structure, has a low chance of benefit. And endoscopic examination of the pyloric orifice structure and selecting the appropriate patient may improve GBI therapy's success.
Nonobjective measurement and categorization of the pyloric orifice is a major obstacle in this research. Benzodiazepine medication applied for anesthesia initiation may have a relaxing impact on pyloric muscle, but no data about the influence of this anesthetic on pyloric tonus are found in the literature; studies only focus on the effect of benzodiazepines on the hepatopancreatic sphincter and distal esophageal muscles. 33 The second major limitation is that the intragastric botulinum toxin A therapy for treating obesity is still not recommended by the FDA. Like this one, new research heading this issue would engage the FDA's attention to reconsider this obesity treatment technique. This study's third weakness is that all patients included in this study had Caucasian ethnicity; implied results may not be generalizable to obese patients with different ethnicities. Also, the retrospective nature and the short-term follow-up period of this research and not to compare the given data with a control group are other weaknesses of our study. Despite all these limitations, the retrospective character of our research and including all intragastric botulinum toxin A-injected patients between June 2019 and June 2020 make it impossible to make bias during the creation of study groups.
Conclusion
Intragastric botulinum toxin A application therapy would become a trending bariatric therapy for patients suffering from obesity, who are not candidates for surgical treatment options with comparable clinical outcomes. Early results of this study show that this emerging endoscopic bariatric therapy technique provides better results in class I–II obese patients with normal pyloric orifice structure.
Footnotes
Authors' Contributions
M.F.F. and A.C.K. collected the information, reviewed the literature, and wrote the article. A.I.F. and A.K. critically reviewed the article, and approved the final form. All authors read and approved the final article.
Ethical Approval Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Also, Ethics committee of Istanbul Okan University approved study (19.08.2020/56665618-204.01.07).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.