
Abstract
Background:
Serious postoperative complications such as leakage, bleeding, or gastric obstruction may occur in laparoscopic sleeve gastrectomy (LSG). There is no ideal method or technique to avoid these mishaps. The purpose of this study was to evaluate the effectiveness of modified omentopexy (MOP) added to LSG in reducing postoperative complications.
Materials and Methods:
This study included retrospective analysis of medical charts of 567 morbid obesity patients who underwent LSG. The patients were divided into two groups: group A of 180 LSG patients with MOP, and group B of 387 LSG patients where no omentopexy (OP) was done.
Results:
Leakage was detected in one (0.2%) patient in group B. Symptomatic stenosis requiring surgical intervention was detected in four (0.7%) patients, who were all in group A. Sleeve stricture was detected in one (0.2%) patient and gastric twist in three (0.5%) patients. It was found that LSG with MOP significantly increased the risk of gastric twist (p < 0.05).
Conclusions:
OP, which we created with our own technical modification in LSG, did not reduce the risk of postoperative complications.
Introduction
Obesity is a serious chronic disease that has already reached epidemic proportions. It is becoming one of the leading causes of death and disability worldwide. The surgery-induced weight loss has proven to be very effective in treating obesity and its comorbidities. 1 Laparoscopic sleeve gastrectomy (LSG) is the most popular bariatric procedure in many countries. 2 LSG is a highly feasible technique and has a shorter learning curve compared with other surgeries, such as laparoscopic Roux-en-Y gastric bypass (LRYGB) and biliopancreatic diversion with duodenal switch.3,4 Factors contributing to the popularity of LSG include preservation of normal anatomy and absorptive capacity of the intestine. There is no particular risk of vitamin or mineral deficiency as seen in the gastric bypass. 5 The results regarding the percentage of total weight loss and resolution of comorbidities are quite satisfactory.6,7
Although LSG is relatively a safe surgical option, various possible complications have been reported in the literature
Materials and Methods
This study was approved by the Institutional Review Board for Ondokuz Mayis University Faculty of Medicine, “IRB approval number 352/2020.” Medical records of patients undergoing bariatric-metabolic surgery at the Ondokuz Mayis University Faculty of Medicine General Surgery Clinic between December 2012 and March 2020 were retrospectively analyzed. A total of 567 LSG patients who were operated by a single surgeon in a single center were included in the study. Patients were divided into two groups: group A of 180 LSG patients with MOP, and group B of 387 LSG patients where no OP was done. Patients in group A were operated between October 2015 and January 2018. Patients in group B were operated between the remaining dates.
Age, gender, body mass index (BMI), comorbid conditions, concomitant surgery, operation time, and postoperative outcomes were recorded as data. The criteria for bariatric surgery include patients with a BMI >40 kg/m2, or a BMI >35 kg/m2 associated with at least one comorbidity, in which surgically induced weight loss is expected to improve the disorder, such as, hypertension, ischemic heart diseases, type 2 diabetes, obstructive sleep apnea syndrome, dyslipidemia, severe arthropathy, and obesity-related severe psychological problems. All the patients were assessed by a multidisciplinary bariatric team that consists primarily of the following: bariatric surgeon, psychiatrist, endocrinologists, anesthesiologist, and dietitians.
Written consent was obtained from all patients, including the risks and possible complications of the operation. Upper gastrointestinal (GI) endoscopy was routinely performed before the bariatric surgery. Biopsy was taken if suspicious lesions were seen. All patients were started on a proton pump inhibitor once a day 2 weeks before surgery. In addition, preoperative liquid diet was applied in this period. On postoperative day 2, routine upper GI contrast studies were performed for early detection of gastric leak and stenosis (Figure 1). Enoxaparin sodium was administered the night before operation and was continued for 2 weeks after the surgery for the venous thromboembolism prophylaxis.

Surgical technique
The patient was positioned supine with the legs and both arms in abduction (French position). Two grams of intravenous cefazolin was administered as antibiotic prophylaxis before the induction of general anesthesia. Elastic compression stockings were used for prevention of deep vein thrombosis. In laparoscopy, we routinely used five trocars. Dissection of the greater omentum started at the point measured 2–3 cm proximal to the pylorus with a 5 mm LigaSure Technology (Covidien, Mansfield, MA). The dissection was continued to the point of His angle and left diaphragmatic crus. The stomach fundus was completely released, and the gastroesophageal fat pad was mobilized. The stomach was lifted anteriorly, and any adhesions between the stomach and anterior aspect of the pancreas were divided with LigaSure. A 38 French bougie was placed orally to guide us in forming the tube.
Four or five staplers (Endo GIA™ reloads with Tri-Staple™ technology, Covidien Europa, Dublin, Ireland) were used for gastric tube formation. The first stapler was fired at a point 2–3 cm proximal to the pylorus for antral resection of the stomach. Purple cartridges (4 mm staple height) were used for the first two or three firings. In super-obese, especially in male patients, cartridges with a staple height of >4 mm were used, since the thickest part of the stomach was in the antrum. Tan cartridges (3 mm staple height) were used for the resection of the upper stomach. Resection was performed on the lower and upper walls of the stomach, evenly away from the bougie and preserving the curvature line in the cartridges passage. The last stapler was fired >1 cm away from the Hiss angle. We preferred to keep the stapler fully closed for ∼10 s before firing and ∼30 s after firing. Any staple line bleeding was reinforced with clips.
Intraoperative methylene blue test was performed in all patients. In all surgeries, synthetic tissue adhesive material (Tisseel Lyo; Baxter Healthcare Ltd., England) was applied to the stapler line. In addition, the gastroesophageal fat pad, which had been previously mobilized, was attached to the stapler line with tissue adhesive. In the MOP group, the omentum was sutured to the new greater curvature of the stomach at two different points in the corpus and antrum with using absorbable 2.0 vicryl sutures (Figure 2). The resected stomach was removed from the abdominal wall through the dilated 15-mm trocar incision in a specimen retrieval bag. A negative pressure drain was placed near the stapler line.
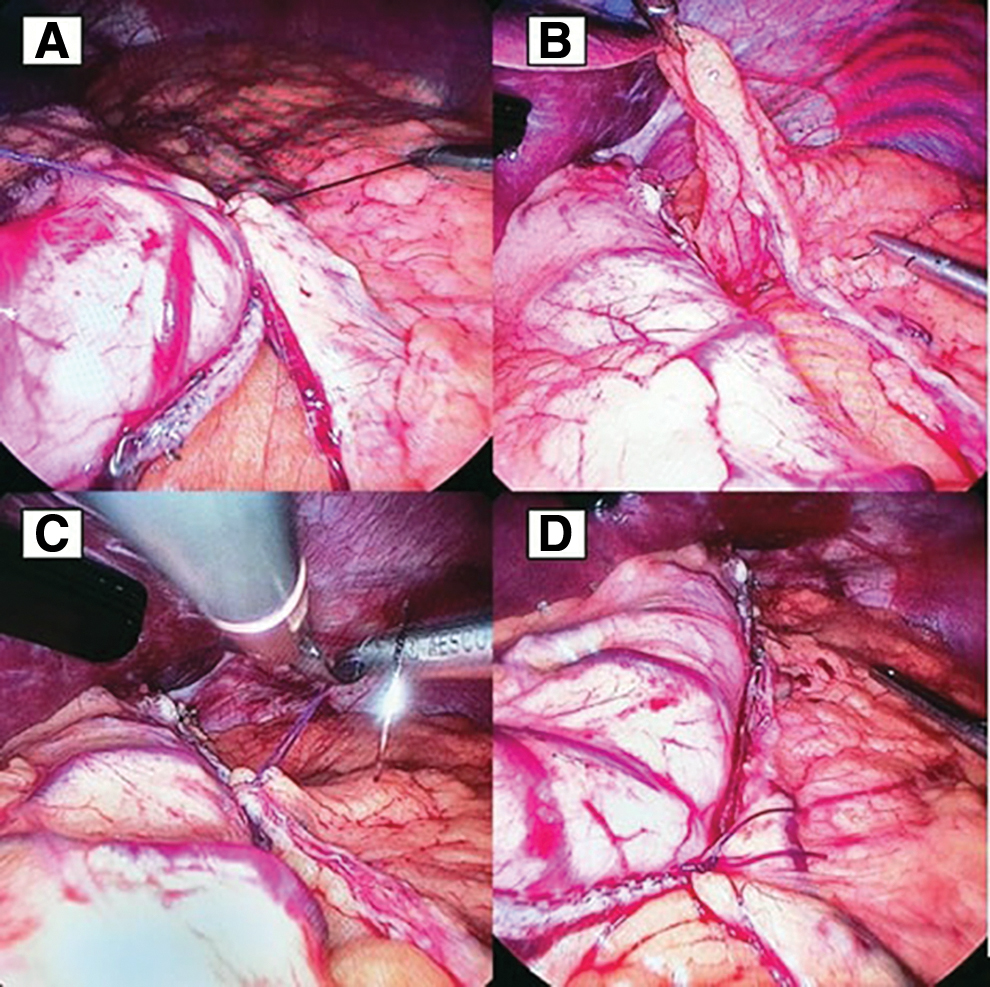
Showing steps of performing MOP.
Statistical analysis
Statistical Package for Social Sciences (SPSS) for Windows 15.0 program was used for statistical analysis. In the evaluation of the study data, besides the descriptive statistical methods (mean, standard deviation), in the comparison of qualitative data, Pearson's chi-squared test was used. The p-value <0.05 was considered significant. Independent sample t-test was applied in the analysis of the significance of the difference between the averages obtained.
Results
A total of 567 patients undergoing LSG were selected for this study. Out of those, 180 underwent LSG with MOP and 387 underwent LSG without OP. The mean age was 36.8 ± 11.1 years and 72.8% of the population was women. The mean preoperative BMI was 45.3 ± 7.4 kg/m2. Comorbid conditions and concomitant surgeries are presented in Table 1. Simultaneous laparoscopic cholecystectomy was performed during LSG for gallbladder stones in 47 patients (8.3%). Mean operating time was 75.3 ± 23.2 min, and there was no conversion to open surgery in both groups. No intraoperative leak was identified during methylene-blue test in our series. Postoperative complications are summarized in Table 2. There were no significant differences between the two groups regarding bleeding, postoperative leakage, gastroesophageal reflux disease, persistent vomiting, stricture, neuropathy, and portal vein thrombosis. All postoperative bleeding cases recorded were resolved with blood transfusion and conservative treatment. Leakage was detected in one (0.2%) patient in group B in the early postoperative period. Laparotomy was performed on postoperative day 4 and the abdominal cavity was irrigated. Endoscopic stent was used to control the leak and total parenteral nutrition was given for a long time.
Patient Characteristics and Perioperative Data
BMI, body mass index; M, mean; n, number of patient; SD, standard deviation.
Postoperative Outcomes
GERD, gastroesophageal reflux disease; PVT, portal vein thrombosis.
Upper GI system contrast study was performed in 23 (4.1%) patients with suspicion of stenosis such as persistent vomiting and gastroesophageal reflux in the postdischarge period. Oral and IV contrast-enhanced abdominal tomography and upper GI endoscopy were performed on eight (1.4%) patients with suspected stenosis in the upper GI system contrast study. Four patients (0.7%) had symptomatic stenosis requiring surgical intervention. Sleeve stricture was detected in one (0.2%) patient and gastric twist in three (0.5%) patients. RYGB was applied to three patients who were operated due to stenosis, and mini-gastric bypass was applied to one (Table 3). Other patients' symptoms disappeared after dietary recommendations, medical treatment and conservative follow-up. It was found that LSG with MOP significantly increased the risk of gastric twist (p < 0.05).
Gastrointestinal Obstruction and Their Management
RYGB, Roux-en-Y gastric bypass.
In group A, subacute axonal distal symmetric sensorimotor neuropathy in one patient, lumbar plexopathy in one patient; In group B, burning feet in one patient and small fiber neuropathy in two patients were detected. The neurological complication rate in the two groups was 1.1% and 0.8%, respectively, and this was not statistically significant. Portal vein thrombus was observed in two (0.4%) patients in group B and there was no statistically significant difference between the groups. The thrombotic event was controlled with prompt anticoagulation therapy. There was no statistical difference between groups for length of hospital stay (4.1 days for group A vs. 3.9 days for group B, p > 0.05). Reoperation rates were significantly higher in patients undergoing LSG with MOP (p < 0.05). No peri- and postoperative mortality was encountered at a mean follow-up of 40.4 months for group A, and 28.9 months for group B.
Discussion
LSG has been increasingly used in the past decade due to its growing popularity and comparable weight loss outcomes. LSG is less complex bariatric procedure when compared with gastric bypass or biliopancreatic diversion. It does not involve any digestive anastomosis, and there are no mesenteric defects that pose a risk of internal herniation. However, it can be converted to other bariatric procedures in the future if necessary. The advantages of LSG include a low rate of complications, maintenance of GI integrity, and absence of malabsorption.3,9 The most feared complication of sleeve gastrectomy is a staple line leak. The literature reported that the worldwide incidence of post-LSG leak ranged from 0.5% to 7%.10,11 Early leaks within 2 days of surgery are caused by mechanical factors, such as stapler misfire, or wrong staple size for the tissue. Late leaks appearing after several days are usually related to tissue ischemia caused by tension on the anastomosis, distal bowel obstruction, or hematoma. 12
Although most surgeons prefer to staple line reinforcement, such as oversewing, buttressing, OP, and fibrin sealant to reduce the risk of leakage after LSG, some surgeons leave the staple line untouched. 13 Staple line reinforcement has been a controversial issue that has been frequently discussed. 14 All major randomized prospective studies and meta-analysis did not show a significant difference between reinforcement by (oversewing or buttress on stapler) and untouched section, in terms of leakage rate.10,15 We only encountered leakage in a patient who underwent LSG without MOP. The leak occurred in the corpus of the stomach and was about 4–5 cm in size. We treated this complication, which was observed in one of our first patients, by laparotomic drainage, and endoscopic placement of a covered stent.
The most serious other complications are the bleeding (2–2.5%), and stenosis (0.26–4%).16–18 Depending on the severity of the hemorrhage and the surgeon's judgment, reoperation or a conservative approach may be followed. There are ongoing discussions regarding the effect of staple line reinforcement on hemorrhage. Berger et al. 19 showed that patients who underwent buttressing with or without oversewing of the staple line had significantly lower bleeding rates than did those patients with no reinforcement. Musella et al. 20 found that using fibrin sealant significantly reduced risk of postoperative bleeding after LSG compared with no reinforcement. In our own case series, hemorrhage complications were observed in 1.6% of cases. None of the patients required reoperation. Vital signs and complete blood count were used to monitor patients who developed postoperative bleeding after SG. In clinical observation, transfusions of blood and blood products were provided when necessary. In these patients, drains were kept longer than usual. Patients were discharged without requiring additional interventions.
Sleeve stenosis can occur due to the intentional narrow tubularization of the stomach. It has been reported to occur in ∼0.26–4% of LSG operations.21,22 The diameter of the bougie used to calibrate the remnant stomach could impact the rate of gastric stenosis. Starting stapling too close to the pylorus may cause stenosis by excessively narrowing the sleeve tube at the incisura angularis level. A twisted or spiral sleeve, which is caused by the progressive rotation of the staple line in an anterior to posterior plane, can lead to a functional narrowing despite a fairly normal luminal diameter. Axial twist of the sleeved stomach, which mostly occurs at the incisura angularis, may occur within days or months later.23–25 Proper alignment of the staple line and the symmetrical division of the anterior and posterior walls of the stomach represent the main factor to prevent axial twist of sleeved stomach. Some surgeons advocate fixing the staple line to the pancreatic fascia, especially when the gastric tube tends to curl. 26
OP can prevent the gastric twist by stabilizing the posterior stomach wall. 27 Abdallah et al. 9 showed that staple line inversion and distal fixation to the transverse mesocolon can be a simple and effective strategy to prevent staple line bleeding and gastric axial rotation. However, in a prospective randomized study conducted by Afaneh et al. on 60 morbidly obese patients who underwent LSG with or without OP, it was concluded that fixing the gastric tube to the larger omentum did not significantly decrease postoperative complications. 28 Another study showed that fibrin sealant helps prevent twisting and narrowing of the sleeve stomach by providing adherence. 29 In the MOP group, one patient was operated for postoperative stricture and three patients for gastric twist. The patient who developed postoperative stricture had a history of gastric band, and the gastric band had been removed 2 months before the sleeve gastrectomy. Extensive scar tissue was detected at the gastric fundus level, and conversion to an LRYGB was performed just proximal to this area on the ninth postoperative day. Two of the three patients operated for gastric twist were converted to LRYGB at the 11th and 13th months, respectively, whereas one patient was converted to mini-gastric bypass at the 33rd month postoperatively. In all three patients, axial twist of the sleeved stomach was detected at the level of incisura angularis.
In our technique, the omentum was fixed to the sleeve tube with two stitches at the antrum and corpus level. In our study, the rate of gastric twist was found to be significantly increased in the MOP group. If the omentum was closed continuously along the sleeve tube, maybe the results would have been different, we do not know. Our technique changed 6 months before the last stenosis episode and has remained constant since that time. We carried out the proper alignment of the staples and the symmetrical division of the anterior and posterior walls of the stomach. We fixed the sleeve tube to the pancreas anterior surface with fibrin sealant. Endoscopic stenting appears to be effective tool in management of axial rotation of sleeved stomach. Balloon dilation can also be used in selected cases. 30 Some surgeons say endoscopic stenting is a successful option for such problems, whereas others state that surgical treatment is mandatory.31,32 We preferred surgical treatment in our own series.
Neurological complications such as encephalopathy, optic neuropathy, myelopathy or myeloneuropathy, radiculoplexus neuropathy, polyneuropathy, and mononeuropathy (resulting in carpal tunnel syndrome, meralgia paresthetica, or foot drop) can be rarely seen after SG. These patients usually have long-term GI symptoms, rapid and excessive weight loss, and vitamin supplementation deficiency. 33 Rare and colleagues 34 reported that seven (1.18%) of 592 patients who underwent SG had neurological complications after surgery. Neurological complications were observed in 0.9% of all patients after SG in our series. Although there were no GI symptoms in five patients with neurological complications, excessive weight loss was found in these patients during the first 3 months postoperatively. In these patients who did not have neurological diseases before SG, symptoms may have occurred due to rapid weight loss rather than oral nutritional disorder after surgery. Aggressive multivitamin and mineral replacement was used in the treatment. Oral multivitamin supplements were administered for at least 6 months after discharge. All patients responded to aggressive vitamin therapy with most of their symptoms resolving within a few months of treatment.
The limitations of our study were associated with the disadvantages caused by the retrospective feature. Although there were comparative control groups and the number of patients was sufficient to obtain statistically significant results, the study lacked randomization. The higher level of experience by the single surgeon may have affected the outcomes in the second group. In addition, the low rate of major complications after sleeve gastrectomy may have limited the strength of this study.
For better results after LSG, we recommend the proper alignment of the staple line and symmetrical division of the anterior and posterior walls of the stomach, as well as fixing the staple line to the pancreatic fascia using fibrin sealant.
Conclusions
OP, which we created with our own technical modification in LSG, did not reduce the risk of postoperative complications. On the contrary, these patients were found to have an increased risk of gastric twist.
Footnotes
Acknowledgments
The authors thank Ufuk Karabacak and Can Akgun for assistance with data analysis and interpretation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.