
Abstract
Background:
Individuals with obesity frequently contend with pain, but few studies address the clinical impact of comorbidity within this population. This study compared the early weight loss outcomes and complications of bariatric surgery for participants with and without presurgical pain.
Methods:
A retrospective analysis of data stored in a registry of patients who had undergone bariatric surgery was conducted. Patients completed a routine preoperative psychological and medical evaluation. Participants were grouped based upon the presence of at least one pain condition and/or pain site: pain (n = 184) or no pain (n = 30). Participants completed questionnaires regarding 21 psychological and 17 medical complications and reported their weights at their 1- and 3-month postoperative psychological appointments.
Results:
The majority of the final sample (n = 214) identified as 69% female and 66% Caucasian. Contrary to the hypothesis, results indicated no significant mean differences in 1- and 3-month postoperative medical and psychological complications, or percentage excess and total weight loss between the groups.
Conclusions:
In the early postoperative period, participants with preoperative pain and comorbid obesity lose weight and experience complications to a degree comparable with participants without preoperative pain. Implications for clinical interventions and future research are discussed.
Introduction
One in five adults have chronic nonmalignant pain. 1 Furthermore, the prevalence of many chronic pain conditions has risen from 2006 to 2016. 2 Risk factors for chronic pain include female gender, older age, 3 lower socioeconomic status, history of abuse, number of pain sites, severity of pain, depression, anxiety, and obesity.4,5 Previous research has shown that there are many individuals whose pain has been unsuccessfully treated, despite numerous attempts at pharmacologic treatment and a high utilization of health services. 6 The treatment of chronic pain presents many challenges to today's health care system due to the complex interaction of biological, psychological, and social factors that constitute the pain experience.
A growing body of literature identifies increasing body mass index (BMI) as a significant predictor of chronic pain.4,7 A multistate study showed pain complaints become more prevalent as BMI rises. 8 Relative to those in the normal weight category, chronic pain is 20% more common in individuals with overweight, 68% higher for people with class I obesity, 136% higher for people with class II obesity, and 254% greater for people with severe obesity. 8 Obesity may increase the risk of pain through multiple mechanisms, including increased load on weight-bearing joints, inflammation, 9 and psychological distress. 10 Common characteristics shared by persons with obesity and pain conditions include fatigue, lethargy, poor sleep, social withdrawal, and psychological symptoms (e.g., depressed mood and problematic eating habits).11–13 This confluence of pain and weight-related physical discomfort leads to decreased physical functioning, which, in turn, contributes to a loss of muscle strength and worsening joint pain. Body deconditioning and lack of movement can also contribute to depression and social isolation,14,15 and as a result lead to weight gain. 16 The lack of energy, sedentary behavior, and psychological sequelae that often accompany these conditions can be significant barriers to patients following postoperative protocols and achieving significant weight loss. 17
Bariatric surgery leads to long-term weight loss and improvements in obesity-related comorbidities and is considered the most efficacious treatment for severe obesity. 18 However, a sizeable percentage of patients regain a significant amount of weight at extended follow-up.19,20 A large body of research has identified predictors of weight loss outcomes.20,21 However, few studies have examined postoperative weight loss differences for patients with and without chronic pain. Kubat et al. completed a retrospective review of 254 bariatric surgery patients at a veterans affairs medical center, 59.1% of whom had a confirmed diagnosis of osteoarthritis. 22 Compared with patients without osteoarthritis, patients who had osteoarthritis demonstrated a lower percentage excess BMI loss at all time points (i.e., 1, 3, and 5 years after bariatric surgery). Similarly, patients with severe pain lost significantly less weight in a behavioral program at 12 months compared with patients with moderate or no pain. 23 Although limited, the results of these two studies provide preliminary evidence that chronic pain negatively impacts weight loss.
Current study
Although evidence suggests that many areas of psychological functioning improve with bariatric surgery, 24 chronic pain predisposes many patients to psychopathology, poor coping, and substance use. 9 These factors may make patients with chronic pain more susceptible to early complications and poorer early outcomes after surgery. For example, chronic pain can negatively impact a patient's physical and mental health and may increase the risks of inactivity and poor dietary habits. Therefore, this study aimed to examine potential differences on early postoperative weight loss, medical complications, and psychological complications between bariatric surgery participants with and without significant preoperative pain (i.e., at least one pain condition). No research to date has examined the impact of presurgical pain on early postoperative medical or psychological complications. It was hypothesized that participants experiencing preoperative pain would have greater postoperative medical and psychological complications and less weight loss compared with participants without preoperative pain.
Materials and Methods
Participants
This study retrospectively analyzed data obtained as part of an ongoing data collection project within the bariatric surgery center of an academic medical center. Data were abstracted from patients who had bariatric surgery between January of 2010 and December of 2012. None of the patients had undergone revision surgery. All bariatric surgery candidates completed comprehensive preoperative evaluations with members of the medical, psychological, and nutrition teams, and were scheduled for postoperative follow-up appointments with the same clinicians. Participants were retained from an initial database of 529 patients if they had undergone bariatric surgery, were an adult (i.e., age >18 years), and had information available regarding both their presurgical pain status and their postoperative 1- and 3-month psychological visits (Fig. 1). The final study sample included 214 participants (Table 1). Chi-square and t-test analyses revealed no significant differences in age, gender, race, surgery type, or presurgical BMI between the initial and final study samples. This study was approved by the institutional review board.
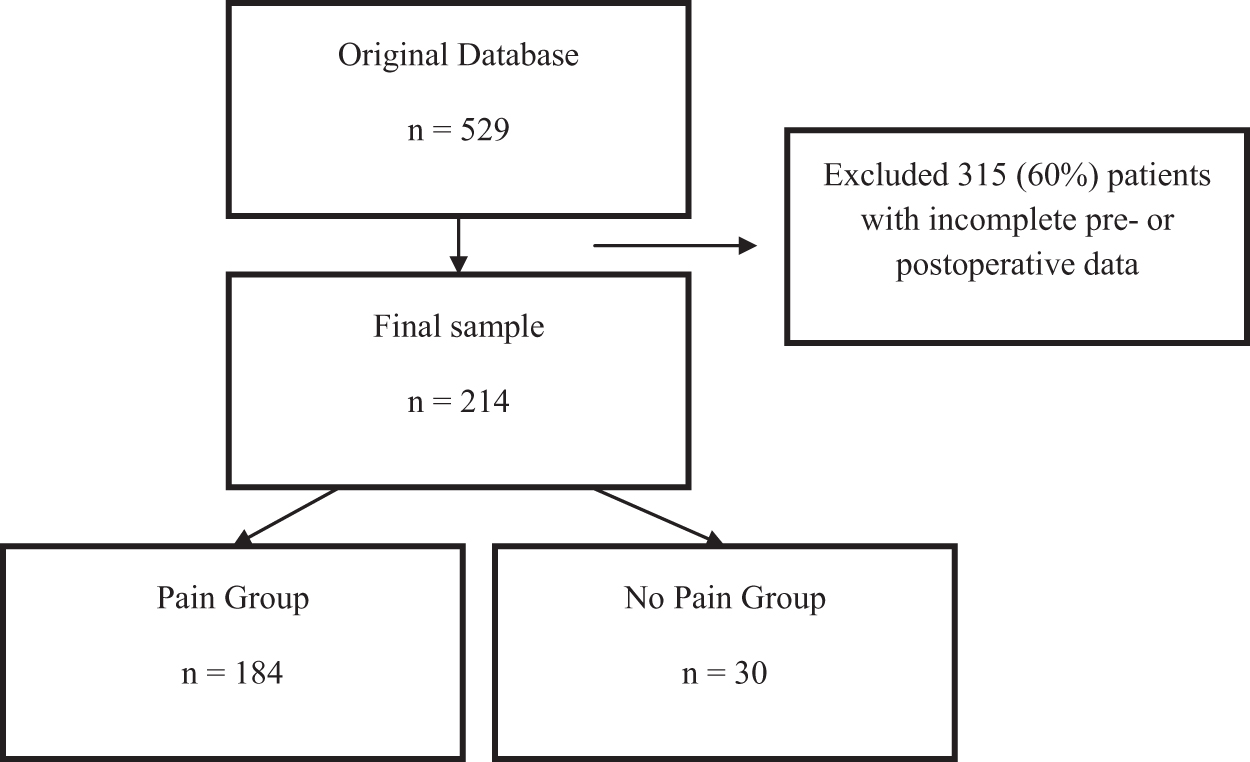
Final sample selection process.
Demographic and Surgical Information for the Entire Sample (n = 214)
BMI, body mass index; RYGB, Roux-en-Y gastric bypass; SD, standard deviation; SG, sleeve gastrectomy.
Preoperative BMI and pain information
Information regarding preoperative BMI and pain was obtained through a retrospective chart review of the participants' electronic medical records (EMRs). The last recorded preoperative BMI from any appointment in the bariatric center was abstracted from each patient's EMR. The documented presence of each pain condition and/or pain site was abstracted from the EMR and coded as 1. A total score was calculated for pain by adding up the number of individual pain conditions and/or pain sites in each participant's EMR. The chronic pain total score was then dichotomized so that participants with a score of 1 or more were included in the pain group.
Participants were grouped based upon the presence of at least one pain condition and/or pain site: pain (P+; n = 184) and no pain (P−; n = 30). Table 2 contains a summary of the pain groups' demographic and surgical information. The P− group was slightly younger than the P+ group (t = −2.67, p < 0.05). Chi-square and t-test analyses revealed no other significant differences in preoperative BMI, surgery type, race, or gender between the chronic pain groups. Table 3 contains a list of the pain experienced by the P+ group and the number of participants who experienced each.
Demographic Information for the Pain Groups
Number of Chronic Pain-Related Conditions Experienced by the Chronic Pain Group
All patients in the chronic pain group experienced at least one or more of the following conditions/syndromes.
DJD, degenerative joint disease.
Measures
Postoperative complications
Patients completed a packet of self-report questionnaires at their 1- and 3-month postoperative shared psychological appointments. Patients completed the questionnaires before beginning the group appointment and their answers were reviewed by the psychologist during the appointment. The same questionnaires are administered across all shared postoperative psychological appointments (e.g., 1- and 3-month appointments). The packets include commonly administered and validated measures of psychological functioning (i.e., General Anxiety Disorder-7 and Patient Health Questionnaire-9). The packets also include checklists created by the study institution asking participants to endorse whether they have experienced any of 21 psychological or 17 medical complications listed since undergoing surgery.25–28 Table 4 contains a list of each psychological and medical complication assessed. Each medical or psychological complication endorsed by a patient was coded as 1. A total score was then calculated for medical complications (maximum 17) and psychological complications (maximum 21) by adding up the number of individual complications endorsed for each category. For example, a patient who reported experiencing 1-month postoperative anxiety, sleep problems, body image problems, and relationships problems would get a score of 4 for 1-month psychological complications.
Postoperative Psychological and Medical Complications
Weight loss
Preoperative weights were obtained through a review of the participants' EMRs. Trained staff members recorded preoperative weights using the same scale at each appointment in the bariatric center. The last recorded weight before surgery was obtained for this study. Participants' postoperative weights were self-reported at 1- and 3-month follow-up appointments. Percentage excess weight loss (%EWL) and percentage total weight loss (%TWL) were calculated for each participant.
Statistical analyses
Multivariate analyses of covariance (MANCOVAs) were computed to examine mean differences in 1- and 3-month postoperative medical and psychological complications. Analyses of covariance (ANCOVAs) were computed to examine mean differences in 1- and 3-month postoperative %EWL and %TWL between the pain groups. Because there was a significant difference in age between the two groups, age was entered as a covariate in all analyses. An a priori power analysis was conducted based on the desired effect size (f = 0.25), alpha level (0.05), and power (0.95). Based on these criteria, a minimum of 210 participants would be necessary to detect a statistically significant effect. This indicates that the available sample size (n = 214) was sufficient to test the proposed hypotheses.
Results
Table 5 contains a summary of the pain groups' average medical complications, psychological complications, %EWL, and %TWL at 1- and 3-months postoperative visits. The results of the MANCOVA and ANCOVA indicated no significant mean differences in 1-month postoperative medical complications [F (2, 210) = 0.53, p = 0.47], psychological complications, [F (2, 210) = 0.56, p = 0.45], %EWL [F (1, 204) = 1.12, p = 0.29], or %TWL [F (1, 204) = 1.72, p = 0.43] between the groups, after controlling for age (Table 5). The results of the MANCOVA and ANCOVA indicated no significant mean differences in 3-month postoperative medical complications [F (2, 136) = 0.24, p = 0.62], psychological complications [F (2, 104) = 0.27, p = 0.60], %EWL [F (1, 124) = 3.14, p = 0.08], or %TWL [F (1, 124) = 1.60, p = 0.19] between the groups, after controlling for age (Table 5).
Results of the Multivariate Analyses of Covariance and Analyses of Covariance for 1- and 3-Month Postoperative Outcomes
%EWL, percentage excess weight loss; %TWL, percentage total weight loss.
Discussion
This study examined the average percentage excess and total weight loss and frequency of medical and psychological complications after bariatric surgery among participants with and without preoperative pain. Pain was markedly common, affecting 85.9% of the sample. Contrary to the hypotheses, there were no significant mean differences in 1- and 3-month postoperative psychological or medical complications or percentage or total excess weight loss between the pain and no pain groups.
As previously discussed, there are a limited number of studies examining the relationship between chronic pain and weight loss.22,23 Overall, the prior studies indicated that chronic pain negatively impacts weight loss at medium- to long-term outcomes.22,23 A possible explanation for the discrepancy between these results is that this study assessed weight loss and complications early at the 1- and 3-month time points postsurgery. In the early postoperative period, participants may be highly motivated to achieve their goals and feel energized by the positive results they initially experience. They may follow the postbariatric surgery guidelines more carefully with regard to food and water intake as well as exercise. Surgery effects are most robust early on and higher adherence with a phased postoperative diet program more likely occurring during the early months. This may lead to significant and comparable weight loss with participants without pain. However, to the extent that their pain persists after surgery, patients with preoperative pain may find it more difficult than their pain-free peers to maintain an exercise program, leading eventually to diminished weight loss.
Conversely, because excess weight can exacerbate pain and lead to declines in functioning and well-being, early postoperative weight loss may reduce pain in those who previously suffered from it. 29 Indeed, previous research has demonstrated that patients experience significant decreases in pain after bariatric surgery.30,31 For example, Vincent et al. found at the 3-month postbariatric surgery follow-up, patients' low-back pain and knee pain had decreased 54% and 34%, respectively. 32 Moreover, Vincent et al. reviewed evidence showing that this reduction in pain after bariatric surgery is maintained in most joints into the long-term postoperative period. 33 Since this pain reduction would be expected only in those already experiencing pain, bariatric surgery may have narrowed the difference between the two groups, leading to their equivalence in short-term outcomes. In addition, given that patients with a pain condition can be high utilizers of health care resources, 6 they may have preemptively sought out more appointments (e.g., PT, OT, sessions with a psychologist, and appointments with the bariatric surgery team) before bariatric surgery, which may have contributed to them experiencing comparable results with patients without a pain condition. However, this hypothesis remains difficult to reconcile with the noted differences in medium- and long-term outcomes.
Limitations and future directions
There are several limitations of this study that have implications for future research. The lack of expected group differences may be a result from the paucity of participants without pain in the current sample. This may have limited the power to detect a genuine group difference. Further investigation with a more heterogeneous sample would be useful. In addition, this study's reliance on a simple self-report measurement of postoperative psychological and medical complications may have limited the ability to detect group differences. Future studies should aim to include validated measures of these outcomes. This study also relied on a mixed group of participants with pain, with some who experienced chronic conditions while others experienced significant pain at different pain sites without information regarding chronicity. Future research examining samples of single chronic pain conditions (i.e., just degenerative joint disease or just diabetic neuropathy), intensity of pain, and/or single medical and psychological complications may allow for a more nuanced understanding of how specific chronic pain conditions may impact specific surgical outcomes. The current data analyses were limited to participant outcomes at the 1- and 3-month follow-ups. It will be important for future research to use a well-controlled prospective longitudinal study to assess both the short- and long-term outcomes to evaluate whether and why pain groups may achieve different outcomes. Such a study would also benefit from more direct measurement of variables expected to influence weight loss, such as presurgical psychological and medical comorbidities, postoperative pain levels, exercise participation, and food intake. Lastly, data coding and abstracting errors should be considered.
Implications
These preliminary results do not support the use of pain as a prognostic variable for bariatric surgery candidates. However, given the discrepancies between these early results and prior studies' finding of lower weight loss at later follow-up periods, future research is warranted to provide greater clarity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.