
Abstract
Background:
Bariatric surgery is well established as an effective long-term treatment for obesity. The addition of vagotomy to bariatric surgery is thought to control hunger and satiety, but its efficacy has not been fully assessed. This systematic review aims to elucidate the effectiveness of vagotomy added to bariatric surgical procedures on weight loss.
Materials and Methods:
This study was conducted according to PRISMA guidelines. Human studies (in the English language) investigating vagotomy added to bariatric surgery were included. We used the RoB2.0 model and ROBINS-I tool for assessing risk of bias in each study. A meta-analysis was performed using the meta package in R and the Mantel–Haenszel weighing method.
Results:
A total of 363 records were identified from the original search. Four studies were analyzed involving 1495 participants. Percentage excess weight loss was extracted as the primary outcome measure. There was no statistically significant difference in weight loss between patients undergoing bariatric surgery with and without vagotomy.
Conclusions:
Performing vagotomy with bariatric surgery does not lead to additional weight loss. This review only included four studies and the lack of a significant difference may be due to underpowering and heterogeneity. Further studies need to be adequately powered and the methodology and outcomes should be standardized.
Introduction
The prevalence of obesity is an overwhelming global health issue. A strong association with type 2 diabetes, ischemic heart disease, and stroke renders its control imperative for preventing premature morbidity and mortality. Conservative management of obesity has generally shown ineffective results for sustained weight loss, which has led to the rising demand for surgical alternatives.
Since identification of the relationship between the vagus nerve and hunger, 1 its potential role in the control of obesity has become increasingly recognized. This was clinically demonstrated by Dragstedt and Owens 2 who showed that patients being treated for ulcer disease by vagotomy reported earlier satiety. Following the work of Kral,3–5 vagotomy, as a stand-alone procedure for treatment of morbid and severe obesity, gained some interest.6,7 However, as a likely result of greater efficacy of newer bypass and restrictive procedures, vagotomy for the primary treatment of obesity fell out of fashion.
The vagus nerve is exclusively responsible for the parasympathetic innervation of the gastrointestinal tract to the level of the distal transverse colon, thus playing a critical role in gut–brain communication and regulation of gut function 8 —through its efferent rootlets projecting from the dorsal motor nucleus of vagus and the nucleus ambiguus and its afferent rootlets synapsing in the nucleus tractus solitarius. 9
Efferent fibers, which make up 20–30% of the subdiaphragmatic vagus nerve, initiate the release of gastric acid from parietal cells and govern the motility of the gastrointestinal tract. The afferent (sensory) fibers, accounting for the remaining 70–80%, provide important negative feedback signals through chemo- and mechanosensitive receptors, leading to orexigenic and anorexigenic effects. 10 The combination of both afferent and efferent fibers and their functions illustrate complex interactions of central and peripheral networks ultimately responsible for energy homeostasis.
Interest in combining peripheral and central control over obesity in the form of weight-reducing surgery with vagotomy has led to numerous clinical studies. The aim of this review is to assess the efficacy of adding vagotomy to bariatric surgical procedures in improving weight loss outcomes. We conducted a systematic review and meta-analysis of relevant studies.
Materials and Methods
Eligibility criteria
Studies investigating the effect of vagotomy with other bariatric procedures on weight loss were included in this study. The population included patients undergoing any form of bariatric procedure—defined as any operative management used to treat patients with a body–mass index (BMI) greater than 30 following failure of medical treatment. The exposure intervention was vagotomy, compared with the control group of bariatric surgery without vagotomy. Studies included in this review ranged from randomised controlled trials (RCTs) to observational studies. All variations of vagotomy were included.
For inclusion, articles must have reported the weight loss data of more than two patients at least 12 months after the initial surgery and expressed weight outcome as percentage excess weight loss. For eligible articles, data were taken at the earliest point that met the inclusion criteria regarding participant numbers and weight outcome measurement. Extraction of data on operation and vagotomy type as well as secondary observations was performed from eligible articles. Studies of surgical procedures with vagotomy without a comparison group were excluded.
Information sources
Search items were applied to electronic databases with the last search run on June 20, 2021, for PubMed/MEDLINE (1946–present), Ovid EMBASE (1980–present), and Cochrane Central Register of Controlled Trials (CENTRAL). Reference lists of included articles were examined together with hand searching of articles published on similar subjects.
Search strategy
The search strategy used is presented in Table 1 for the Ovid EMBASE (1980–present) database. Articles were only included if they were published in the English language and were studies on human subjects. The same search strategy was applied to the remaining two databases.
Search Strategy for Ovid EMBASE (1980–Present)
Study selection
Assessment for eligibility of studies was performed independently in an unblended standardized manner by one reviewer (H.U.). H.U. performed hand searching of all referenced studies for further articles that fulfilled inclusion criteria. The final study inclusion was agreed by consensus by a second and third author (J.J. and M.M.-W.).
Data collection process
A data extraction worksheet was developed using Microsoft Office Excel 2010 for all final included studies. The first author (H.U.) extracted data from all included articles. The second and third authors (J.J. and M.M.-W.) subsequently checked the data.
Data items
From each individual study, data were extracted with predefined variables. Weight loss data were expressed as pre- and postoperative weight, change in BMI, percentage total weight loss, and percentage excess weight loss. Percentage excess weight loss was the only outcome provided in all articles and hence was used for the meta-analysis. All definitions of percentage excess weight loss were included. Data taken were at baseline and the earliest date from which the outcome met the inclusion criteria. Secondary outcomes for each study were also reported. Finally, the study characteristics were extracted, including the setting, type of study, sample size, type of surgical procedure, vagotomy type, and follow-up time.
Study risk of bias assessment
Randomized and nonrandomized studies were rated as low, moderate, or serious concern of bias according to two tools: the Cochrane Risk of Bias 2.0 (RoB2.0) 11 tool for assessing RCTs and the ROBINS-I tool 12 for assessing nonrandomized studies. Assessment of risk of bias was performed independently by three reviewers to reach a consensus (H.U., J.J., and M.M.-W.).
Synthesis of results
Data extracted were synthesized using percentage excess weight loss. For studies that did not include standard deviation for percentage excess weight loss, the missing standard deviation was calculated and converted to a percentage value using the Cochrane Method 16.1.3.2, “Imputing standard deviations for changes from baseline.” 13
A correlation coefficient was calculated (estimated as 0.5) and applied across all studies to obtain the standard deviation of excess weight loss change. A meta-analysis was performed using the meta package in R with the Mantel–Haenszel weighing method. 14 Qualitative analyses were performed on an intention-to-treat basis. Continuous data are reported as mean difference with 95% CI. Heterogeneity was assessed using the I-squared (I 2 ) value. An I2 score of 25%, 50%, and 75% represented low, moderate, and high heterogeneity, respectively. Random effect was used as the analysis moderator in the case of between-study heterogeneity.
Results
Study selection
The PRISMA flowchart 15 is shown in Figure 1. An initial search yielded 363 articles. Studies were explored by hand searching through references of articles with zero studies added. Following the removal of duplicate articles, a total of 281 articles were screened based on title and abstract. Of these, 12 articles were identified as fulfilling the inclusion criteria. A further eight articles were excluded for the reasons shown in Figure 1. A final total of four articles were used in this meta-analysis.
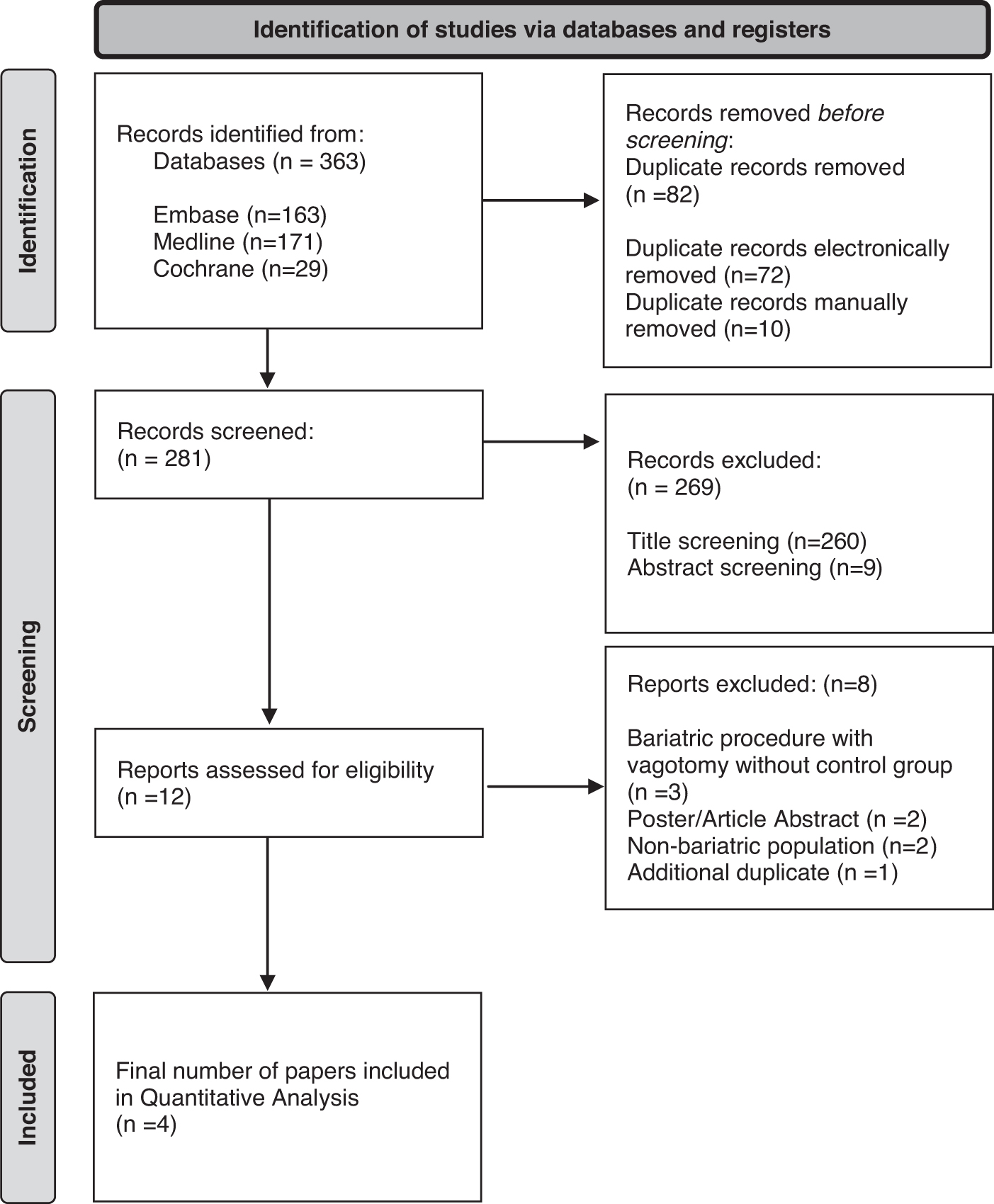
PRISMA search flowchart.
Study characteristics
Two studies investigated laparoscopic gastric banding (LGB). Angrisani et al. 16 conducted a randomized trial, assigning a total of 50 patients to LGB with or without vagotomy. Follow-up time was 12 months. Martin and Earle 17 conducted an observational study with 98 patients undergoing LGB with and without vagotomy. Follow-up time was a mean of 33.6 and 36.5 months in the exposure group and control group, respectively.
Roux-en-Y gastric bypass was reviewed by Okafor et al., 18 who included 1278 patients in a retrospective study. Follow-up time was 12 months. Kral et al. 19 investigated 69 patients undergoing vertical banded gastroplasty (VBG) with and without vagotomy. Follow-up time was a mean of 55 and 66 months in exposure and control groups, respectively. Truncal vagotomy was performed in all exposure groups apart from Okafor et al. 18 who performed a highly selective vagotomy. The study characteristics of the final four included studies in this meta-analysis are summarized in Table 2.
Study Characteristics
Risk of bias
Figures 2 and 3 depict the use of the Cochrane Collaboration risk of bias tools, ROBINS-I and RoB2.0, to assess the risk of bias in the included studies. The results for all included articles were either performed by or adjusted to intention-to-treat analysis.
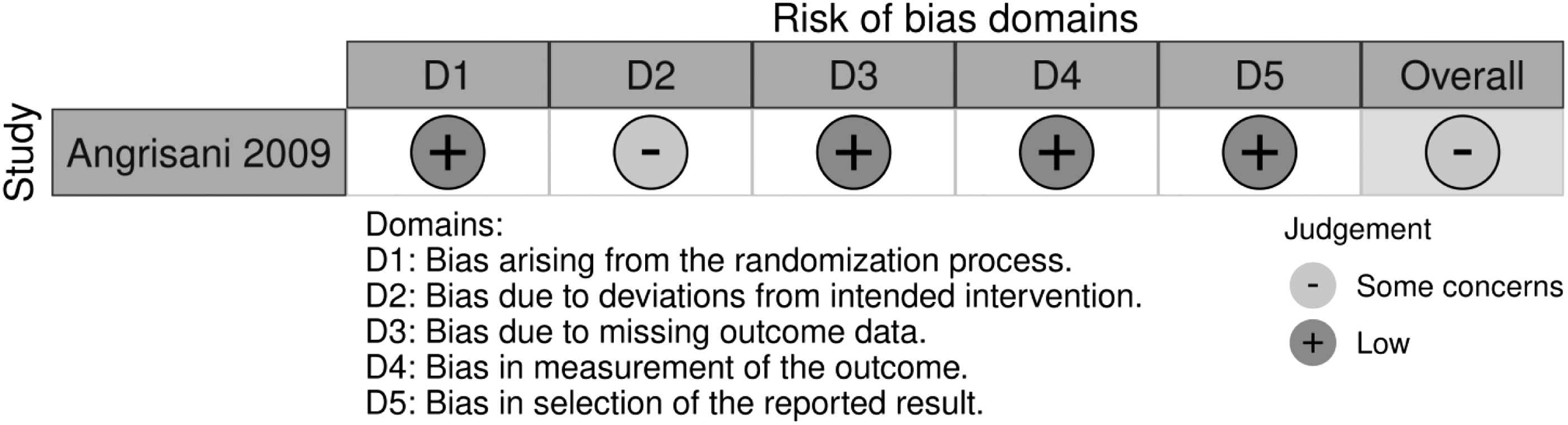
Risk of bias—RoB2.0 tool for RCTs. RCTs, randomised controlled trials.

Risk of bias—ROBINS-I tool for non-RCTs.
The RoB2.0 tool was used to assess RCTs; application by Angrisani et al. 16 is shown in Figure 2.
The study by Angrisani et al. 16 had an overall moderate risk of bias. Moderate concern was regarding deviations from the intended intervention. Patients were made aware of study group allocation during the trial 24 h before intervention delivery. Failure in implementing the intervention was possible, which may have affected the outcome. This was evidenced by vagal tissue being resected with no additional attempt to identify more vagal fibers intraoperatively. Of the 25 patients allocated to the vagotomy group, a total of 4 patients were not included in the 12-month follow-up. Two patients were excluded due to previously unrecognized intraoperative findings, while another two patients were lost to follow-up. However, there is no evidence that the result was not biased by missing outcome data.
The Cochrane Collaboration risk of bias tool, ROBINS-I, was used to assess the risk of bias for the following three observational studies, illustrated in Figure 3.
An overall serious risk of bias was present in the study by Kral et al. 19 Of the 30 patients in the vagotomy group, 11 had vagotomy before enrollment into the study due to insufficient weight loss and were then allocated to the exposure group. In this way, the start of intervention and follow-up did not coincide. Follow-up time varied considerably between groups. No statistical differences in weight, age, BMI, or comorbidities were found preoperatively. Comparison of weight loss between polypropylene and fascia bands, as well as men and women, showed no statistically significant differences. Although the classifications of interventions were well defined, some aspects of assignment to intervention status were determined retrospectively.
Martin and Earle 17 demonstrated a moderate overall risk of bias in their study. Confounding was expected, with important domains such as age, sex, race, smoking status, baseline weight, and follow-up time being controlled for in the analysis. With regard to selection of participants, an observational control group of 49 patients was added at the 6-month mark for interim analyses to obtain a preliminary efficacy assessment. One patient was pathologically confirmed to have an incomplete vagotomy at the time of intervention; however, this was unlikely to have affected the result of the outcome. Of the 98 patients, 16 were lost to follow-up. The proportion of missing data between groups was similar.
The study by Okafor et al. 18 was deemed to have a moderate risk of bias. Allocation to the vagotomy group was dependent on the surgeon's preference. Analyses performed to account for age, gender, initial weight, and initial BMI were considered, but confounding bias could not be excluded. Missing data for more than 20% of participants at the 12-month follow-up could account for moderate bias. This was proportionally similar between groups and adjusted for in the final analysis.
Synthesis of results
Four studies were combined in a meta-analysis involving 1495 patients. This meta-analysis revealed high heterogeneity, indicated by an I2 value of 86%. Figure 4 summarizes the results of weight loss from these studies. Weight loss outcomes and additional outcomes for each study are summarized in Table 3. The overall pooled mean weight loss percentage difference was not statistically significantly different between groups.
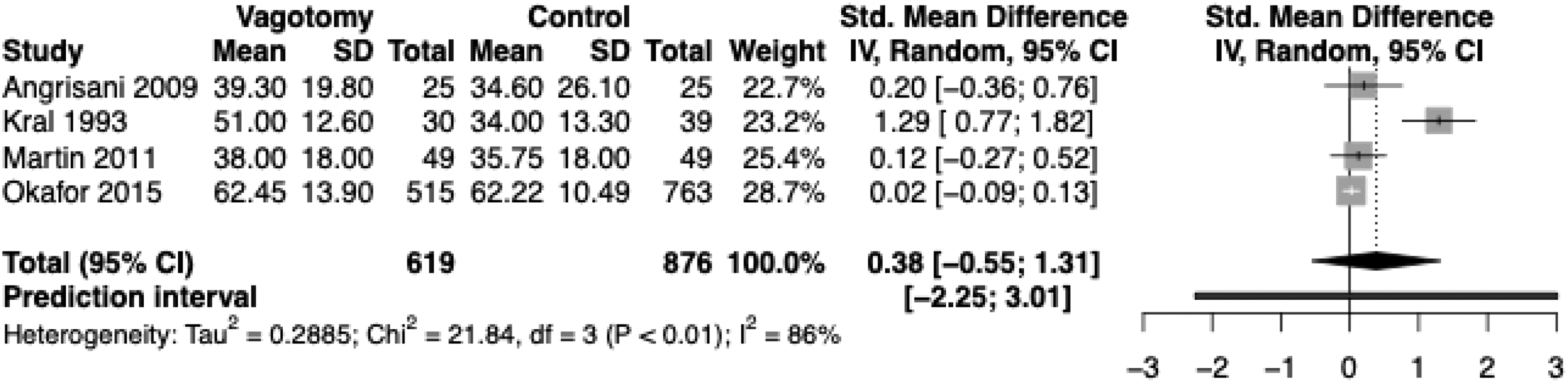
Synthesis of results.
Study Outcomes
Discussion
This systematic review has investigated adding vagotomy to bariatric surgical procedures and its effect on weight loss. A total of four articles were included in this review with 1495 patients. There was no statistically significant difference in weight loss with vagotomy.
Existing human clinical trials on this particular topic are both scarce and mixed. Kral et al. 20 described three studies where vagotomy was performed during gastric bypass procedures for the prevention of stomal ulcers and reflux esophagitis. Retrospective chart reviews in each instance comparing vagotomy patients with obese nonulcer patients did not reveal a significant difference in weight loss.21–23
de Lartigue 24 highlighted the limitations of subdiaphragmatic total vagotomy and emphasized that vagotomy negates the ability to discriminate three important factors: the effect of afferent and efferent nerve fibers on energy metabolism and their possible opposing functions, the variable contribution of fibers from specific organs, and suppression of the stimulatory signals of hunger. The argument for the modern utility of vagotomy in bariatric surgery is still debated—some surgeons find use in its antireflux and ulcer prevention properties, 20 while others do not.
Contrarily, Miyato et al. 25 and Kim et al. 26 supported the additional weight loss effect of vagotomy. Comparisons were made between 30 patients undergoing distal gastrectomy with truncal vagotomy and 33 patients undergoing distal gastrectomy with vagus nerve preservation. 25 Kim et al. 26 compared seven patients undergoing subtotal gastrectomy and truncal vagotomy with nine patients having subtotal gastrectomy alone. The aim of their studies was to observe the adverse weight loss effects from vagotomy for cancer patients. Results showed both a significant reduction in the visceral fat area (not subcutaneous fat area) and greater weight loss in the vagotomy group (−11% ± 7.8%) compared with the vagus nerve preservation group (−7.2% ± 7.2%). Kim et al. 26 also demonstrated a greater percentage weight reduction in the vagotomy group (12.4% ± 2.48%) compared with the control group (8.97% ± 3.61%). They hypothesized that the primary energy-saving function of the vagus nerve may mean that vagotomy may not be as effective in an obese population.
Miyato et al. 25 proved that the vagal system controls visceral fat metabolism and, in fact, supported the idea of its denervation, leading to excess weight loss for pathological obesity. Both articles were excluded from the meta-analysis.
Furthermore, Inci et al. 27 compared nondiabetics receiving VBG with and without vagotomy. Findings of weight and BMI reduction were significantly greater in the vagotomy group (19%) compared with the control group (9%). Similar results have been reproduced. 28 Truncal vagotomy with VBG caused a reduction in excess weight (44%) compared with VBG alone (33%), with no difference in long-term mortality or complications. Unfortunately, these data were extracted from a conference abstract only and full text was not available.
Many theories have arisen regarding the direct role of the vagus nerve in weight loss. One hypothesis is that vagotomy prevents aberrant orexigenic vagal afferent signaling in obesity, 24 where the loss of neurochemical plasticity is caused by excessive and repetitive feeding. Neuropeptides and receptors associated with increasing food intake are promoted. Preventing this signaling in obesity may subsequently reduce body weight. Kral et al. 19 initially believed that the effect of vagotomy causing delayed gastric emptying would explain a reduction in weight. Their results revealed that gastric emptying was inversely proportional to weight in the gastroplasty group alone, but surprisingly no relationship was found in the vagotomy group. A prior observation 29 of vagotomy causing reduced liquid consumption became their primary belief for the role of the vagus nerve in weight loss, although through unknown mechanisms.
Kral et al. 20 later proposed that the primary effect of vagotomy was on the hormone, ghrelin, which affects both short- and long-term regulation of body weight. Since the vagus nerve may need to be intact for ghrelin to increase appetite and food intake in humans, vagotomy may decrease ghrelin's orexigenic effect and completely abolish a rise in plasma ghrelin in response to a fasting state. Other neuropeptides and mediating molecules have proven to have some influence in satiety, including cholecystokinin, peptide YY, and glucagon-like peptide 1. 30
There are several limitations to this study. First, significant heterogeneity was present in the included trials for the quantitative assessment, which restricts the generalizability of this analysis. This may be attributed to the variable risk of bias and study methods between articles. Variations in how weight loss data are defined have been identified as an issue, 31 explaining how these differences can have significant and even erroneous effects on outcome results. Applying various definitions in their patient cohorts elicited weight regain ranging from 9% to 91%. For our included studies in this review, weight outcome data were expressed as pre- and postoperative weight, change in BMI, percentage total weight loss, or percentage excess weight loss.
Percentage excess weight loss was the only outcome consistently used across all articles and hence it was used in the meta-analysis. The calculation of percentage excess weight loss was different among some of the included articles, while some did not explicitly explain its calculation at all. Another limitation was the inclusion of observational studies along with RCTs. This resulted in high heterogeneity and reduced the certainty of evidence as observational studies inherently have a serious risk of bias.
Conclusions
Our study has shown that the addition of vagotomy to bariatric surgical procedures does not appear to significantly augment weight loss. Further research is needed in the context of other common bariatric procedures, including sleeve gastrectomy. Future work should include adequately powered randomized trials and robust standardized methodology.
Footnotes
Authors' Contributions
The study was designed by Dr. Unasa. Data acquisition was performed by Drs. Unasa, Jin, and Mauiliu-Wallis. Statistical reports were generated by Drs. Unasa and Jin. Statistical analysis/interpretation was performed by Drs. Unasa, Jin, and Mauiliu-Wallis. Manuscript drafting was performed by Dr. Unasa. Critical review of the manuscript was performed by Prof. Hill and Drs. Jin and Mauiliu-Wallis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.