
Abstract
Abstract
Background:
It is necessary to fortify human milk to promote optimal growth of the very preterm infant. However, the addition of non-human milk components to human milk is not ideal because of the risk of feeding intolerance and necrotizing enterocolitis. Human milk products (HMP) are an alternative to commercially available fortifiers, but their preparation is likely to result in modifications to the qualities of human milk.
Methods:
Ten batches of HMP were prepared with the aim of meeting a desired protein:energy ratio of 3.0 g of protein/100 kcal. Ultrafiltration was used to produce a skim milk concentrate, to which cream was then added to produce the final HMP. Characterization of HMP and human milk fortified with commercial human milk fortifiers (Nutriprem® [Cow & Gate, Limerick, Ireland] and S-26 SMA human milk fortifier [Wyeth Nutrition, Baulkham Hills, NSW, Australia]) included quantifying macronutrient content, osmolality, microbial content, and particle distribution.
Results:
Average protein:energy ratio of the final batch was 2.93 ± 0.10 g of protein/100 kcal, equating to an inaccuracy of 2.5% relative to the desired ratio of 3.0 g of protein/100 kcal. Significantly greater fat (P < 0.01), lower lactose (P < 0.001), and lower osmolality (P < 0.001) were characteristic of the HMP compared to human milk fortified with either commercial fortifier. Microbial growth occurred during preparation of HMP but did not exceed 105 colony-forming units/mL, and pasteurization of human milk prevented contamination in 80% of batches.
Conclusions:
HMP can be designed to accurately target the protein and energy requirements of the preterm infant, but modifications of the macronutrient, biochemical, structural, and microbial characteristics of human milk may affect the quality of the final product.
Introduction
Commercially available human milk fortifiers (HMF) contain casein and whey proteins derived from bovine milk, lipids from both plants and microbial sources, and carbohydrates derived from plants. 8 Although the addition of non–human milk-derived components to human milk is beneficial for promoting the growth of the preterm infant, bovine milk proteins have a different amino acid composition 9 and are not as efficiently digested as human milk proteins. 10 Furthermore, infants fed fortified human milk may also exhibit higher rates of feeding intolerance 11 and necrotizing enterocolitis. 12
An alternative to fortifying human milk with commercially available HMFs is human milk products (HMPs) that are derived from human milk. Human milk products are prepared by separating the cream and skim milk, the latter of which is then subjected to ultrafiltration to increase protein concentration. 13 The skim milk concentrate (SMC) and the cream can then either be freeze-dried to form a powder or added directly to human milk in amounts required to meet the protein and energy requirements of the preterm infant. As such, this process of “lactoengineering” allows the composition of human milk to be manipulated to meet the macronutritional requirements of the individual preterm infant without the addition of non-human components.
Several randomized clinical trials have assessed the efficacy of feeding preterm infants HMP. Preterm infants fed HMP containing added human milk protein exhibited improved growth metrics compared to preterm infants fed just human milk. 14 Other studies have also shown that preterm infants fed HMP with either added human milk protein and fat or added protein only had higher growth rates than infants fed HMP containing added fat only. 15 Preterm infants fed HMP with added human milk protein also have growth rates similar to infants fed preterm formula 16 or human milk fortified with bovine whey protein. 17
These studies have assessed the growth outcomes of preterm infants fed various different preparations of HMP, but little is known about the modifications that occur to the characteristics of human milk during their preparation. Potentially, alterations to the biochemical, structural, and microbiological characteristics of human milk could affect the quality of the HMP. Therefore, it is important to investigate how the preparation of the HMP affects these properties.
Materials and Methods
Human milk samples
Samples of human milk were obtained from the Perron Rotary Expressed Milk Bank, King Edward Memorial Hospital, Subiaco, WA, Australia. All donors gave written consent for their donations to be used in research, and this study was approved by The University of Western Australia ethics review board.
Preparation of human milk products
Ten batches of pooled donor human milk were initially prepared, and the cream and skim milk of each batch were then separated by centrifuging at 5,000 g for 30 minutes. After centrifugation, the skim milk was carefully removed from below the cream layer using a pipette under vacuum. The batches of SMC were then prepared by centrifuging 60 mL of skim milk in a Jumbosep™ centrifugal device fitted with a 30-kDa molecular weight cutoff filter (Pall Corp., Ann Arbor, MI) at 2,500 g for 3–6 hours at 30°C.
The amount of cream required to adjust the energy and protein ratio to the desired target was calculated using the following equation:
where CP = cream to be added (in g/dL), PC = protein content of SMC (in g/dL), PE = desired protein:energy ratio (in g of protein/100 kcal), FF = energy conversion factor for fat (in kcal/g), FC = fat content of SMC (in g/dL), FL = energy conversion factor for lactose and glucose (in kcal/g), LC = lactose content of SMC (in g/dL), FP = energy conversion factor for lactose (in kcal/g), and CF = proportion of fat in cream (in g of fat/g of cream).
The vessel containing the SMC was then tared on a weighing scale, and the required amount of cream was carefully added with a pipette. The cream was heated to 30°C to increase fluidity and ease of resuspension. After addition, the cream was resuspended to produce the final HMP by agitation in an orbital shaker at 60 rpm for 15 minutes at 37°C (Fig. 1).
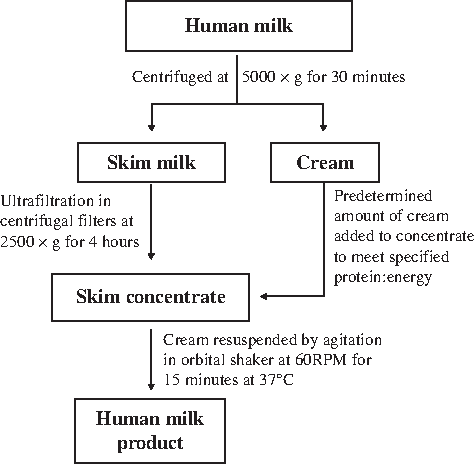
Flow diagram illustrating the steps involved in the preparation of the HMP.
Fortification of human milk with commercial HMF
One packet (2.0 g) of either Nutriprem® (Cow and Gate, Nutricia, Trowbridge, Wiltshire, UK) or S26-SMA (Wyeth Nutrition, Baulkham Hills, NSW, Australia) was added to 50 mL of each batch of unpasteurized pooled donor human milk. The HMF was then dissolved in the human milk by vigorous manual agitation for 5 minutes.
Macronutrient and energy content of human milk
Fat, protein, and lactose content were determined spectrophotometrically as previously described.18–21 The total energy content was calculated using the conversion factors of 4, 4, and 9 kcal/g of protein, lactose, and fat, respectively. 22
Osmolality
The osmolality of representative samples (15 μL) of the 10 batches of pooled donor human milk, SMC, and HMP was measured in duplicate by freezing point osmometry using a Fiske One-Ten Osmometer (Advanced Instruments Inc., Norwood, MA).
Pasteurization of samples
Samples of the 10 batches of pooled donor human milk, SMC, and HMP were pasteurized in 50-mL Falcon tubes (BD Biosciences, North Ryde, NSW, Australia) by the Holder method (62.5°C for 30 minutes) in a precision water bath (Huber AG, Berching, Germany) with a resolution of ±0.1°C. Pasteurization temperature was adjusted to ensure that a minimum temperature of 62.5°C was maintained during the holding time. Temperature was monitored via a data acquisition system (Delta Ohm, Padua, Italy) connected to a type K thermocouple (sampling rate 1 Hz) in a Falcon tube containing 50 mL of water that was submerged at the same time as the samples to be pasteurized.
Microbiology
The microbiological content of the 10 batches of pooled donor human milk, SMC, and HMP was quantified by plating either 100 μL of unpasteurized samples or 10-μL aliquots of pasteurized samples on nutrient agar or blood agar and enumerating the number of colony-forming units (CFU)/mL after incubation at 37°C for 24 hours. Nutrient agar was prepared from sterile 2.5% Nutrient Broth No. 2 and 1.5% agar (Southern Biological, Nunawading, VIC, Australia) and blood agar prepared from 4% Difco™ tryptic soy agar (BD Biosciences, Australia) and 5% defibrinated sheep's blood (Serum Australis, Manilla, NSW, Australia).
Particle distribution
The particle distribution of the 10 batches of pooled donor human milk, SMC, and HMP was quantified using a Mastersizer 2000 fitted with Hydro SM sample dispersion system (Malvern Instruments, Westborough, MA). Absorbance was adjusted to meet a target-weighted residual of 1%, a dispersant refractive index of 1.33 was used, and sample added to the dispersion unit until an obscuration target of 10–15% was achieved. Each scan was performed 10 times, and averaged data were collected for further analysis with Dispersion Technology Software version 4.02 (Malvern Instruments).
Statistical analysis
All data are presented as mean ± SD values. Comparison of mean composition and osmolality was performed assuming analysis of variance with the Tukey-Kramer multiple comparisons post-test (Graph InStat version 3.0, GraphPad Software Inc., San Diego, CA). Graphical modeling of data was performed using SigmaPlot version 11.0 (Systat Software Inc., San Jose, CA).
Results
Protein and lactose content of human skim milk during ultrafiltration
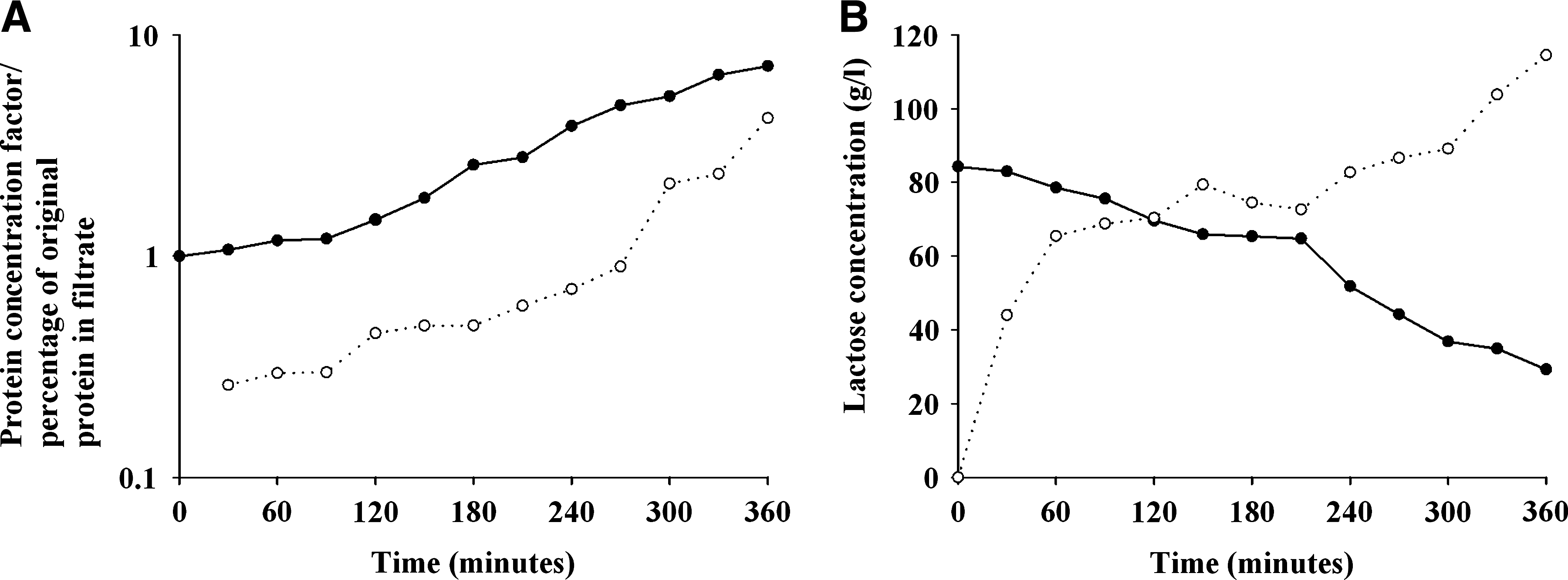
The protein content of the SMC increased proportionally during the course of ultrafiltration with a 7.2-fold increase in protein content achieved after 6 hours of ultrafiltration. Protein content in the filtrate also increased over time in a similar manner but did not exceed 4.2% of the original protein content after the same processing time. Conversely, lactose concentration decreased in the retentate and increased in the filtrate over time (Fig. 2).
(
Composition during preparation of HMP and comparison with commercial HMF
Ten batches of HMP were prepared with the aim of achieving a protein:energy ratio of 3.0 g of protein/100 kcal. The protein concentration of the human milk ranged from 0.85 to 1.36 g/dL. Human SMCs were prepared by ultrafiltration for 3 hours, which was suitable to increase the original protein content by two- to 2.5-fold, whereas lactose decreased to an average concentration of 5.95 ± 0.47 g/dL (Table 1).
Data are mean ± SD values (range) (n = 10). Protein:energy ratio (P:E) is in g of protein/100 kcal.
Mean values are significantly different as indicated: abdefgP < 0.01, cP < 0.001.
The proportion of fat in the cream fraction was found to be 80.2 ± 12.3 g of fat per 100 g of cream (n = 10). This mean value was used as the correction factor (CF) in calculation of the amount of cream required to meet a desired protein:energy ratio of 3.0 g of protein/100 kcal (Table 1). The range of cream that was added to batches was large (2.21–9.26 g/100 mL) with the volume of cream added proportional to protein content of the SMC. After the cream was resuspended in the concentrate to form the HMP, the concentration of protein, lactose, and fat in the final HMP was 2.58 ± 0.38 g/dL, 6.09 ± 0.28 g/dL, and 5.94 ± 1.21 g/dL, respectively. This equated to an average energy content of 88.2 ± 12.4 kcal/dL and a final of protein:energy ratio of 2.93 ± 0.10 g of protein/100 kcal. This was equivalent to an inaccuracy of 2.5% relative to the desired protein:energy ratio of 3.0 g of protein/100 kcal.
Significant variations in the composition of the human milk samples fortified with either commercial HMF or HMP (P < 0.001) were observed. Significantly higher concentrations of fat (P < 0.01), lower lactose concentrations (P < 0.001), and a greater protein:energy ratio (P < 0.01) were characteristic of the HMP as compared to human milk fortified with commercial HMF (Table 1). Lactose was the only component that varied significantly between human milk fortified with either HMF and was greatest for those samples fortified with S-26 SMA HMF.
Osmolality of fortified human milk
Significant variation (P < 0.001) occurred between the osmolality of the human milk, SMC, and HMP compared with human milk samples fortified with commercial HMF (Fig. 3). The average osmolality of the human milk prior to ultrafiltration was 292 ± 2.99 mOsm and increased significantly (P < 0.001) to an average of 314 ± 8.26 mOsm after ultrafiltration. This pattern of increase in osmolality from the whole human milk to the SMC was observed in all batches (Fig. 3). A slight decrease in the osmolality of the HMP (311 ±7.60 mOsm) was observed relative to the SMC, but the level remained significantly higher (P < 0.01) than the osmolality of human milk.
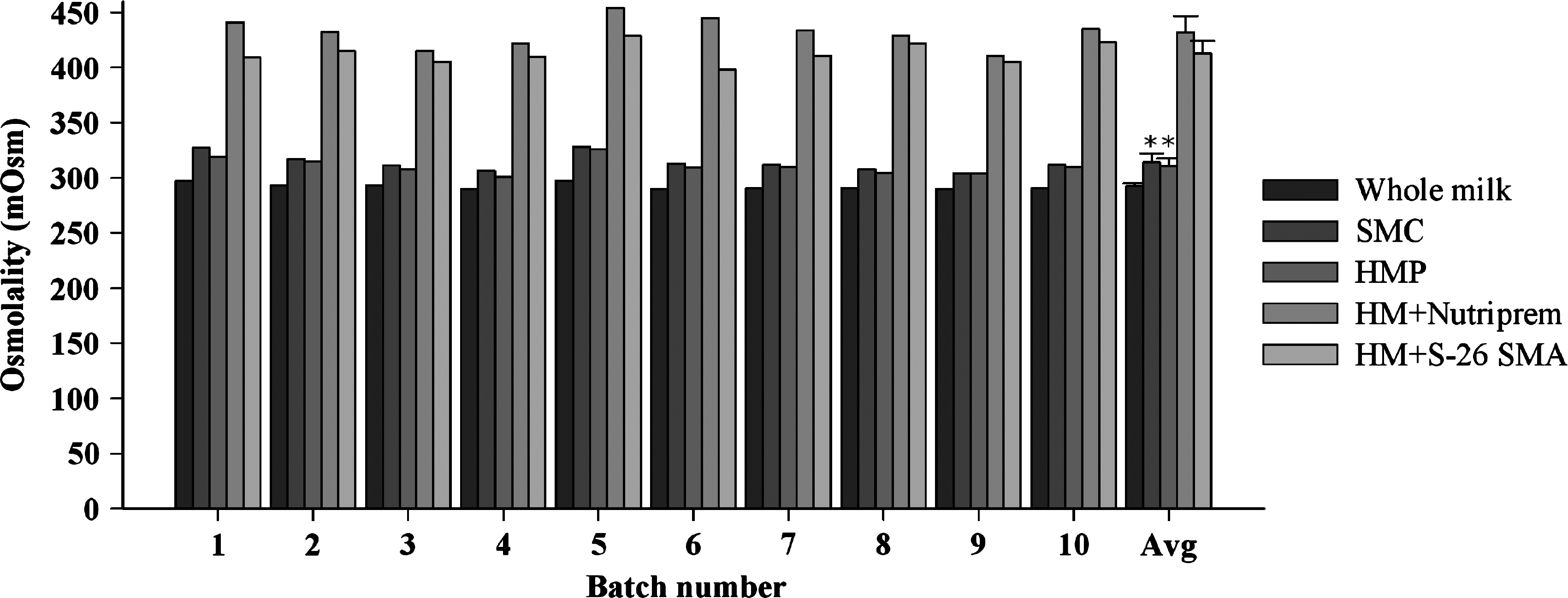
Variation in the osmolality (in mOsm) of 10 batches of pooled donor human milk (HM), SMCs, HMP, and whole HM with added commercial fortifier. *Mean values were not significantly different (P > 0.05); all other mean values were significantly different (P < 0.01).
Fortifying whole milk with commercial fortifier increased the osmolality significantly (P < 0.001) to 431 ± 14.6 mOsm and 413 ± 11.8 mOsm when either Nutriprem or S-26 SMA HMF was added, respectively. The osmolality was also significantly greater (P < 0.001) in human milk fortified with Nutriprem rather than S-26 SMA HMF, and this trend occurred in all batches (Fig. 3).
Processing influences on particle distribution of human milk and HMPs
To determine if preparation of HMP altered the particle distribution of human milk, particle size analysis of three batches (batches 1, 4, and 8) of whole milk, SMC, and HMP was performed (Fig. 4). The average particle size of whole human milk ranged from 2.71 to 4.52 μm. Two of the batches (batches 1 and 8) exhibited a tight distribution around these mean particle sizes, whereas batch 4 comprised a bimodal distribution, with the majority of particles approximately 4.5 μm and a minor population of approximately 11 μm. Mean particle size in the skim milk ranged from 1.31 to 1.71 μm with a mixture of unimodal and bimodal distributions of low abundance present between batches. Compared to the whole milk and SMC, a larger range of particle population sizes were present in the HMP with mean particle size ranging from 6.90 to 9.12 μm. Trimodal particle distributions were present in all three batches of HMP, with the larger particles dominating the total proportion of particles present (Fig. 4). In addition, one of the batches (batch 8) contained particles of greater than 1 mm in size due to visible fat clumping.

Comparison of particle distribution of three batches of whole milk, SMC, and HMP illustrating that preparation of the HMP alters the particle distribution and can result in fat clumping.
Microbial growth during HMP production
The microbial content of unpasteurized human milk samples averaged 42,900 ± 17,800 CFU/mL and 12,900 ± 5,020CFU/mL when samples were plated on either nutrient agar or blood agar, respectively. For all batches, microbial content increased during the production of the SMC and was decreased with the addition of cream (Fig. 5). Pasteurization of the human milk effectively eliminated bacterial contamination in eight out of the 10 batches and reduced the microbial content to ≤2,100 CFU/ml in the remaining batches (Table 2). Subsequently, bacterial contamination was only detected in those batches of SMC that were prepared from contaminated whole human milk. With the exception of one batch of HMP that appeared to have been contaminated during the addition of cream, microbial contamination remained in those batches of HMP that were prepared from contaminated human milk and SMC.

Microbial content of 10 batches of pooled donor human milk, SMC, and HMP. Samples were plated on either nutrient agar (NA) or blood agar (BA) to determine microbial count.
Samples designated with (–) did not exhibit any detectable growth.
Discussion
The application of ultrafiltration for the preparation of HMP for the preterm infant is a relatively recent innovation. Previous studies involved either the addition of the SMC directly to human milk14,16,23 or freeze-drying of the SMC prior to addition to human milk.15,17,24,25 These methods resulted in a protein concentrate of 8% and 51%, respectively, but the approach described here differed in that the cream was added into an SMC containing approximately 2.5% protein. Although it was possible to concentrate the human milk protein to 9.8% (concentration factor of 7.2; Fig. 2), the skimmed human milk was centrifuged for the required time (3 hours) to achieve this desired protein content. It was also observed that 4.2% of the original protein content is lost during ultrafiltration, which is likely to be proteins that are smaller than the molecular cutoff of the filter (30 kDa) that passed through the membrane into the filtrate.
Compared to other methods of HMP production, the preparation of a relatively low percentage protein SMC may be more appropriate for ensuring the quality of the final product. Studies on bovine whey protein concentrates have demonstrated that protein denaturation and aggregation occurs in high percentage concentrates.26–28 This suggests that the bioactivity of human milk proteins may also be compromised when prepared similarly. Freeze-drying is also known to affect the recovery of beneficial proteins like secretory immunoglobulin A, lactoferrin, and lysozyme. 24 Furthermore, the addition of cream directly to the SMC reduces the number of steps required to prepare the HMP, in turn decreasing the number of opportunities for contamination to occur.
The method described here allowed for relatively accurate targeting (2.5% error) of protein:energy as compared to fortifying human milk with commercial HMF. This method effectively standardized the protein and energy content of the HMP, but regular fortification regimens with commercial fortifiers are influenced by the compositional variation of human milk. Furthermore, fat contributes a greater proportion of the energy content of the HMP (60%) than in the human milk fortified with commercial fortifiers (46–47%). This may be advantageous as previous studies suggest that the glucose derived from lactose is not effectively utilized in the liver of the preterm infant,29,30 and therefore fat may be a superior energy source for these infants. However, because lactose content is reduced during ultrafiltration, 13 it may still be necessary to add lactose to the HMP as it is required for non-nutritive functions. 3 Similarly, it would be necessary to add micronutrients to the HMP as ultrafiltration is likely to have decreased the already insufficient concentrations of small water-soluble molecules.
As hyperosmolar feeds are a risk factor for NEC in the preterm infant, 31 the osmolality of the HMP and human milk fortified with commercial HMF was compared. Concentrating the skim milk components increased osmolality, whereas the addition of cream had a diluting effect (Fig. 3). Compared to either the SMC or HMP, fortifying human milk with commercial HMF increased the osmolality above what is considered to be safe for preterm infants (≤400 mOsm). In this regard, HMP may be better suited for the prevention of necrotizing enterocolitis in preterm infants.
The methods used in this study are similar to those used in the manufacture of dairy products like yogurts and cheese 32 ; hence the knowledge gained from the dairy industry can be used to explain other findings of this study. For example, the filtration rate is improved at elevated temperatures, 13 and it was therefore necessary that human skim milk was processed at 30°C. Consequently, the microbial growth that occurred at this temperature, in combination with the concentration effect, resulted in relatively high levels of contamination of the HMP. Although this microbial growth did not exceed human milk banking limits (105 CFU/mL),33–35 pasteurizing the human milk prior to preparation of the HMP effectively prevented microbial growth occurring during ultrafiltration in eight out of the 10 batches (Fig. 4), whereas only very low numbers of bacteria (≤2,100 CFU/mL) remained in those batches that had been heavily contaminated prior to preparation of the HMP (Table 2).
Ultrafiltration concentration efficiency is also affected by the presence of lipids that can lead to membrane fouling. 36 Subsequently, separators are used in the dairy industry to reduce the fat content of the skim milk to less than 1% and, in turn, improve concentration efficiency. 37 As varying amounts of fat remained in the skim milk after the cream was removed, this may have affected the filtration rate leading to the range of protein concentration factors observed (Table 1). Fat clumping after the addition of cream was also observed in this study (Fig. 4). This may be of concern as fat clumping may prevent adequate delivery of fat and energy to the preterm infant during continual feeding. 38 Homogenization is routinely used in the dairy industry to prevent fat separation during prolonged refrigeration and also when cows' milk is modified in a similar way to this study 37 and has been shown to improve outcomes of preterm infants who are fed by the continual feeding method.39,40 Therefore, it is likely that it would be necessary to homogenize the HMP prior to feeding to the infant.
Conclusions
Using the method described in this study, HMPs can be designed to meet the specific protein and energy requirements of the preterm infant while theoretically retaining greater amounts of bioactive proteins than other methods that are currently available. However, various modifications of the qualities of human milk occur during the preparation of these HMPs. This includes alterations of macronutrient composition such as increased lipid and protein content and reduced carbohydrate content as well as a possible decrease in the micronutrient content of lactose. Microbial growth occurs in the SMC, as a consequence of the ultrafiltration process, and it is therefore necessary to pasteurize human milk prior to the preparation of the HMP. Finally, the resuspension of the cream in the SMC to form the HMP results in a considerable modification of the particle distribution of human milk. Therefore, if HMP is used as a nutrition source for the preterm infant, supplementation of micronutrients and homogenization of the HMP prior to feeding should be considered.
Footnotes
Acknowledgments
The authors would like to thank Mr. Jorge Martinez for assistance with the particle sizing studies. We are also indebted to laboratory staff in the Department of Clinical Chemistry at Princess Margaret Hospital, Subiaco, WA, Australia, for kindly allowing access to their department's osmometer. The authors also acknowledge the ongoing support of Western Australian breast milk donors, without whom this research would not have been possible. This study was funded by the Rotary Clubs of Thornlie and Belmont (Western Australia), The Raine Foundation (University of Western Australia), The Perron Charitable Trust, and Medela AG (Switzerland).
Disclosure Statement
No competing financial interests exist.