
Abstract
Abstract
Purposes:
Skin-to-skin care after birth often is absent, interrupted, or delayed for routine procedures. The purposes of this project were to improve skin-to-skin care and exclusive breastfeeding at hospital discharge.
Methods:
For Part 1, we used a descriptive observational design, with video-ethnography and interaction analysis (PRECESS—
Results:
In Part 1, 11 mothers and babies participated: 10 (91%) received immediate skin-to-skin care, eight (73%) received uninterrupted skin-to-skin care, nine (82%) planned to breastfeed, six (67%) of these babies were exclusively breastfeeding at hospital discharge, and five (83%) of the six babies who completed all nine instinctive stages during skin-to-skin care were exclusively breastfeeding at hospital discharge. In our subsequent review (Part 2), we found a significant improvement (25% above baseline) in the overall rate of skin-to-skin care across post-intervention months (Pearson χ2=23.798, df=5, p<0.000), predominantly from improvements in the cesarean section population. The rates of exclusive breastfeeding showed no significant change.
Conclusions:
The PRECESS immersion method may help to rapidly improve skin-to-skin care. Babies who undergo all nine stages during skin-to-skin care may be more likely to exclusively breastfeed. Mothers need support during skin-to-skin care to recognize their baby's readiness to breastfeed. Skin-to-skin care during cesarean surgery may reduce maternal stress and improve satisfaction with the surgical experience.
Introduction
Evidence in support of skin-to-skin care
Mothers who held their babies skin-to-skin after birth were more likely to breastfeed sooner, more effectively, and for longer durations compared with mothers who did not have skin-to-skin care.3–8 After skin-to-skin care, mothers were more likely to care for their babies with more confidence and to recognize and respond to their baby's needs sooner.3,8–10 Babies who had skin-to-skin care during the first hour after birth cried less,3,8,11,12 stayed warmer,3,7,13,14 had more stable blood glucose levels and cardiorespiratory function,8,9,12 had lower stress hormone levels, 15 were more likely to leave the hospital having been exclusively breastfed, and were more likely to have been exclusively breastfed at various intervals during the first 6 months after birth.3,4 Babies who had uninterrupted skin-to-skin care during the first hour after birth typically went through nine distinct stages, from the birth cry through suckling and sleep (Table 1). 16 Skin-to-skin care had a dose–response effect, with immediate and longer durations associated with higher rates of exclusive breastfeeding at hospital discharge. 4
From Widström et al. 16
Lack of skin-to-skin care in the United States
Despite significant health benefits, in the United States, skin-to-skin care often is absent, delayed, or interrupted for routine procedures, 17 such as repairing an episiotomy, obtaining infant weights, or completing cesarean surgery. Among the 82% of hospitals and birth centers that report maternity practices in the United States, only 43% indicated that “most” mothers and babies experienced skin-to-skin care for at least 30 minutes within 1 hour of an uncomplicated vaginal birth; 32% indicated that “most” experienced skin-to-skin care for at least 30 minutes within 2 hours of uncomplicated cesarean surgery. 17
Purposes
The purposes of this quality improvement study were: (Part 1) to describe the rate of exclusive breastfeeding at hospital discharge among healthy mothers and babies who experienced immediate skin-to-skin care after vaginal or cesarean birth during a 5-day quality improvement intervention (PRECESS—
Subjects and Methods
Institutional Review Board approval
This study was approved by the Institutional Review Board at the study site and at an affiliated university. We obtained written informed consent from mothers and a separate written consent to be video-recorded from all persons (family and staff) who were in the room during video-recording of skin-to-skin care.
Conceptual model to promote change
We used the PRECESS immersion model18–20 as our conceptual framework. This model helps to identify and integrate best practices through formal and informal education, expert mentoring during clinical care, video-recording of clinical care, viewing and reflecting on recorded interactions, and continued application of new practices.18–20
Video-recording of clinical care with interprofessional reflection and analysis has been used to describe how clinicians interact during patient handoffs and resuscitation, to assess clinician–patient and interprofessional communication, and to map clinician work. This emerging and promising practice for improving patient safety and healthcare quality provides an opportunity for more accurate conclusions than self-reflection alone and potentially leads to practice change in shorter periods of time.21–26
Background
The study took place at a nonprofit private medical center in the Southwest United States that averages 6,000 births per year. The mixed methods study included two parts. The design for Part 1 was descriptive, observational, and nonexperimental, using the PRECESS immersion method. PRECESS involves hospital staff education about the process of skin-to-skin and newborns' nine instinctive stages during skin-to-skin care, observation and informal mentoring of physicians and nurses in their routine clinical work setting, video-recording of mothers and babies during skin-to-skin care in the labor–delivery–recovery room (LDR) or the operating room (OR), interprofessional reflection and interactive analysis of recordings, and continued application of skills. For Part 2, we tested for differences in monthly skin-to-skin care rates at hospital discharge using medical records reviewed before and after the PRECESS intervention.
Study team
The PRECESS immersion method was used previously in Egypt.18,20 The current study represents the first time, to our knowledge, that the PRECESS method was used in the United States. The study team for the 5-day intervention included three PRECESS specialists and five nurses from the study site. The PRECESS specialists included two nurse–midwife/researchers from Sweden and a video-ethnographer/researcher from the United States with expertise in skin-to-skin care, breastfeeding, normal birth, and work practice ethnography. The nurses from the study site included a researcher/family educator (principal investigator), a clinical education specialist from the labor and delivery and high-risk obstetrics units, two direct care nurses from the labor and delivery unit, and a lactation consultant from the postpartum unit.
Sample
English-speaking women 18 years of age or older who were expected to give birth to healthy infants were recruited for the study. The convenience sample included pregnant women admitted to the hospital labor and delivery unit for a vaginal birth or an elective scheduled cesarean surgery, who agreed to have skin-to-skin care, and who were eligible for skin-to-skin care after birth. “Healthy” and “eligible” were defined as those mothers whose healthcare providers agreed that skin-to-skin care immediately after birth was feasible. “Immediate” was defined as skin-to-skin care beginning in ≤2 minutes of birth.
Data analysis
Descriptive and inferential statistics were used for analysis. Data analysis was conducted using the PASW® Statistics Grad Pack, version 18.0. 27 We used descriptive statistics (mean, SD, range, percentage) to describe the sample in Part 1. We used Pearson χ2 for Part 2 to test for differences in monthly rates of skin-to-skin care and exclusive breastfeeding at hospital discharge.
Procedures
Part 1
We conducted the PRECESS immersion method between August 13 and 17, 2010. On the first day of the intervention, we invited obstetricians, neonatologists, pediatricians, anesthesiologists, nurses (anesthetists, managers, unit supervisors, and nurses from labor and delivery, postpartum, the nursery, and lactation), OR technicians, and childbirth educators to optional formal educational sessions about the evidence in support of skin-to-skin care, the process of clinical care during skin-to-skin care after vaginal birth and during and after cesarean surgery, and the newborn's nine instinctive stages (Table 1) during skin-to-skin care. None of the physicians or nurse anesthetists (Certified Registered Nurse Anesthetists) attended the formal sessions.
Between formal training sessions on the first day and from approximately 6:30 a.m. to 10:00 p.m. during the 5-day intervention, the principal investigator and PRECESS team were present on the unit. Hospital team members encouraged clinicians and staff to support their patients' participation, obtained consents from patients, provided clinical care during skin-to-skin care, and coached their colleagues in providing skin-to-skin care and overcoming potential barriers. We distributed tear sheets 28 to clinicians, staff, and parents that illustrated a newborn's nine instinctive stages during skin-to-skin in the first hour after birth.
We waited until birth was imminent and then entered the LDR or the OR. Mothers and babies were recorded with a video-camera during skin-to-skin care. Video-recording began at birth and continued during the skin-to-skin care period. We discontinued video-recording if a complication occurred and resumed with problem resolution. Direct care nurses dried the babies on the mother's abdomen with warmed blankets, placed them skin-to-skin on the mother's chest, covered them with dry warmed blankets, and placed a cap on the head of some babies. Babies born by cesarean surgery were either dried with warmed blankets on the mother's chest, above the sterile field, or dried with warmed blankets in a cart as babies were moved from the surgical site to the mother's chest. The staff did routine assessment and care procedures during skin-to-skin care. The PRECESS experts and the study team verbally coached clinicians, staff, and families during skin-to-skin care.
The video-ethnographer/researcher edited the video-recordings daily and labeled newborns' instinctive stages and the minutes after birth that the stage occurred. We used an LDR next to the nurses' station for informal education and to provide opportunities for clinicians and staff to analyze and reflect upon video-recordings. We compiled strategies identified by hospital staff to implement skin-to-skin care and documented comments about skin-to-skin experiences from patients, family members, clinicians, and direct care nurses. We documented mother and newborn demographic data, birth and skin-to-skin care experiences, and breastfeeding status at hospital discharge.
Part 2
We determined the monthly rate of skin-to-skin care using a convenience sample of 60 patients (vaginal birth, n=30; cesarean surgery, n=30). We used quality improvement data routinely collected by an advanced practice registered nurse on 1 day each month from active electronic health records. This nurse chose a convenient day each month, based on her schedule, to review medical records. She reviewed medical records by room number and included the first 30 women she found who gave birth vaginally and the first 30 women who gave birth by cesarean surgery; she excluded women if admission documentation showed that they did not plan to breastfeed. She noted whether skin-to-skin care was “present-yes” or “not present-no.” She collected the intervention month (August 2010) skin-to-skin data after the PRECESS intervention.
By contrast, the rate of exclusive breastfeeding was based on all babies each month who were eligible for exclusive breastmilk feeding at hospital discharge, one of The Joint Commission Perinatal Care quality performance core measures. 29 The Joint Commission defines exclusive breastmilk feeding as a term infant “receiving only breast milk and no other liquids or solids except for drops or syrups consisting of vitamins, minerals, or medicines.” 30 A masters-prepared nurse, knowledgeable about the detailed Joint Commission guidelines for exclusive breastmilk feeding at hospital discharge, routinely collected these data, noting “present-yes” or “not present-no.” We based the pre-intervention monthly rates of skin-to-skin care and exclusive breastmilk feeding at hospital discharge on the rate from July 2010. We based post-intervention monthly rates of skin-to-skin care and exclusive breastmilk feeding at hospital discharge on the rates for August–December 2010. August was defined as a post-intervention month, although the intervention occurred August 13–17, 2010, as only monthly data were available. We used the monthly data to assess for improvements and sustainability in rates of skin-to-skin care and exclusive breastmilk feeding at hospital discharge.
Results
Part 1
Sample
Eleven mothers (mean age, 29.3 years; SD, 6 years; range, 20–39 years) and babies participated in the 5-day PRECESS intervention (Table 2). A 12th mother consented to participate but was subsequently withdrawn because her anesthesiologist did not consent to be video-recorded.
A, Asian; C, Caucasian; AA, African American; H, Hispanic.
Stage at end of skin-to-skin prior to transfer from labor and delivery.
Apgar 1/5, 1- and 5-minute Apgar score; Ces, cesarean; Dyad, mother–baby pair; EBMF, exclusively breastmilk fed at hospital discharge; Epi, epidural; F, female; Fam, familiarization; GA, gestational age (in weeks); G/P, gravida/para; IV, intravenous opioids; M, male; NA, not available; NCB, natural childbirth; S2S, skin-to-skin; Vag, vaginal; Wt, weight (in grams).
Labor anesthesia and analgesia
Five women had scheduled cesarean surgery; six delivered vaginally, two after elective induction with oxytocin and four following spontaneous labor. Eight women received epidural anesthetic blocks for labor anesthesia or for cesarean surgery, with most receiving 100 μg of fentanyl prior to the start of their blocks. The epidural anesthesia consisted of local anesthetics (lidocaine, bupivacaine, or ropivacaine) in combination with short-acting synthetic opiates (sufentanil or fentanyl). One woman received spinal anesthesia consisting of a local anesthetic (bupivacaine) without opioids for cesarean surgery, one received analgesia consisting solely of intravenous opioids (three doses of 100 μg of fentanyl) during labor, and one chose natural childbirth.
Skin-to-skin care
Ten (91%) mothers and babies received immediate skin-to-skin care. One baby required an initial assessment at the warmer following cesarean surgery after an unpreventable 5-minute delay between uterine incision and delivery; the baby was placed skin-to-skin 10 minutes after birth and then had uninterrupted skin-to-skin care and moved through all stages of skin-to-skin care. Eight (73%) mothers and babies received uninterrupted skin-to-skin care. Skin-to-skin care was interrupted for the neonatal intensive care team to assess a baby for potential meconium aspiration and resumed 34 minutes later; the newborn suckled before transfer from the labor and delivery area. Skin-to-skin care of two babies was briefly interrupted for fathers to hold their babies; the babies resumed skin-to-skin care and suckled before transfer from the labor and delivery area. The mean duration of skin-to-skin care was 83 minutes (range, 44–129 minutes) (Table 2).
Breastfeeding and newborn stages during skin-to-skin care
Nine (82%) mothers planned to breastfeed. Six (67%) of the babies whose mothers planned to breastfeed were exclusively breastfeeding at hospital discharge. Six (67%) of the babies whose mothers planned to breastfeed went through all nine stages during skin-to-skin care. Five (83%) of the six babies who went through all nine stages were exclusively breastmilk feeding at hospital discharge. Two babies fell asleep after the activity phase, two after the familiarization phase, and one after the crawling phase (Table 2).
Barriers and solutions
Clinicians and staff identified barriers to skin-to-skin care after vaginal birth and cesarean surgery and developed strategies to overcome barriers during formal and informal education and during clinical care (Table 3). Clinicians and staff shared strategies with each other during subsequent births.
Part 2
Skin-to-skin care rates
Skin-to-skin care rates were recorded as present (yes) or not present (no) after birth. Skin-to-skin care start and end times were not recorded consistently in the electronic health record so we did not analyze those data.
We analyzed the overall rate of skin-to-skin care using a convenience sample of n=60 (n=30 vaginal; n=30 cesarean) electronic health records per month (Table 4). Based on a medical record review of 60 patients during July 2010, the baseline skin-to-skin rate was 58% (n=35). Based on a medical record review of 60 patients per month during August–December (n=300), a total of 250 patients (83%) received skin-to-skin care during post-intervention months (Table 4). The post-intervention monthly rate ranged from n=45 (75%) to n=53 (88%) (Fig. 1). Visual inspection of month-to-month rates showed the increasing rate of skin-to-skin care. The overall post-intervention rate (August–December 2010) of skin-to-skin care increased by 25% compared with baseline (July 2010), suggesting clinical improvement. We found a significant difference (Pearson χ2=23.798, df=5, p<0.000) in the rate of skin-to-skin care across the 6 months (July–August 2010).
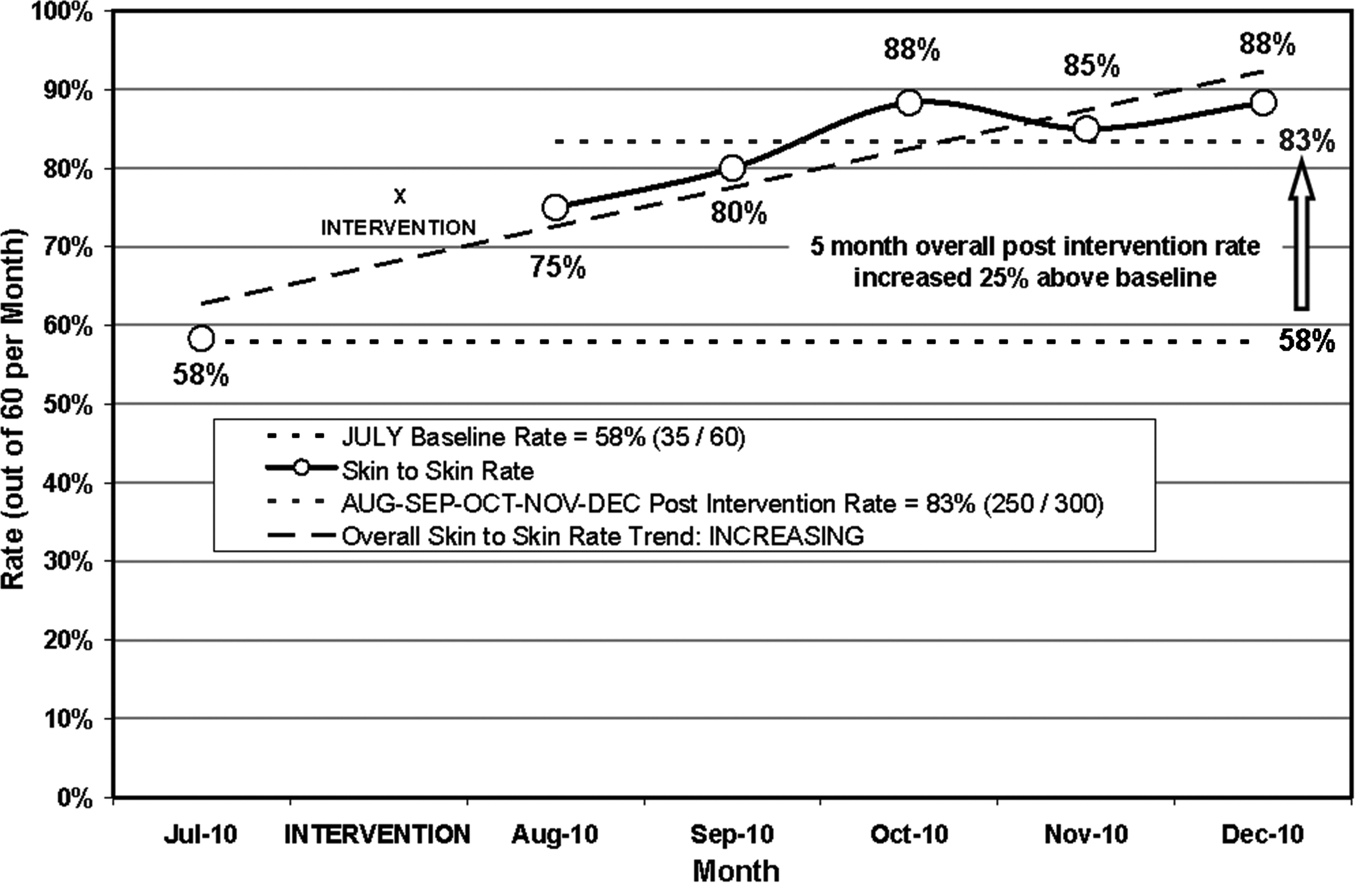
Pre- versus post-intervention skin-to-skin monthly rate in 60 medical records per month (Pearson χ2=23.798, df=5, p=0.000). Pre-intervention (baseline), July 2010; post-intervention, August–December 2010).
The convenience sample consisted of 60 births per month (30 Vag, 30 Ces).
Baseline/pre-intervention month=July 2010.
Skin-to-skin care: Vaginal birth versus cesarean surgery
The trend line of month-to-month rates by birth mode was steeper in births by cesarean surgery versus vaginal birth—suggesting improvements were in the cesarean population. Based on a medical record review of 30 vaginal births during July 2010, the baseline skin-to-skin rate in vaginal births was 93% (n=28) (Table 5). Based on a medical record review of 30 vaginal births per month from August–December (n=150), a total of 139 (93%) received skin-to-skin care during the post-intervention months. In contrast, based on a medical record review of 30 cesarean surgeries, the baseline skin-to-skin rate (July 2010) was 23% (n=7) (Table 5). Based on a medical record review of 30 cesarean surgeries per month from August to December (n=150), a total of 116 (77%) received skin-to-skin care during the post-intervention months. We found a significant difference (Pearson χ2=31.197, df=5, p<0.000) in the rate of skin-to-skin care in the cesarean surgery sample across the 6 months. We did not find a significant difference in the overall rate of skin-to-skin care in vaginal births across the 6 months (Pearson χ2=6.384, df=5, p=2.71), suggesting that the difference in monthly skin-to-skin care rates in cesarean births was responsible for the significant difference in overall skin-to-skin care rates.
The convenience sample consisted of 60 births per month (30 Vag, 30 Ces).
Baseline/pre-intervention month=July 2010.
Exclusive breastmilk feeding rates
Based on a medical record review, 373 babies were eligible to have been exclusively breastfed at hospital discharge during July 2010 (baseline month) (Table 6). The baseline rate (July 2010) of exclusive breastmilk feeding was 52% (n=194). Based on a medical record review, 1,928 babies were eligible to have been exclusively breastfed at hospital discharge during the post-intervention months of August–December. In total, 988 babies (51%) were exclusively breastmilk feeding at hospital discharge. The monthly rate ranged from 49% (n=195 of 397 eligible babies) to 53% (n=184 of 350 eligible babies). We found no significant difference (Pearson χ2=2.690, df=5, p=0.748) in the rate of exclusive breastmilk feeding across the 6 study months.
Eligibility for exclusive breastmilk feeding was as defined by The Joint Commission; exclusive breastmilk feeding was defined as term infants receiving only breastmilk and no other liquids or solids except for drops or syrup consisting of vitamins, minerals, or medicines during the entire hospitalization. 29
Baseline/pre-intervention month=July 2010.
Discussion
This study and the previous findings from Egypt 18 suggest that the PRECESS immersion method is an effective method for changing practice in a short time. We adhered to the PRECESS process during the 5-day intervention; fidelity was maintained through the onsite presence of the experts who had developed and used PRECESS in Egypt. We believe the synergistic effect (hospital staff education about the process of skin-to-skin and newborns' nine instinctive stages during skin-to-skin care, observation and informal mentoring of clinicians and staff in their routine clinical work setting, video-recording of mothers and babies during skin-to-skin care in the LDR or the OR, interprofessional reflection and interactive analysis of recordings, and continued application of skills) is more important to improving outcomes than the individual steps.
Clinicians and staff identified and implemented strategies for overcoming barriers to immediate skin-to-skin care after vaginal and cesarean births (Table 7). Comments from clinicians, staff, and parents suggested satisfaction with the skin-to-skin care experience and reflected improvements in practice (Table 7).
L&D, Labor and Delivery; OR, operating room.
The effect size was unknown when we designed the model. The post hoc power calculation for rate of skin-to-skin care based upon the total sample size (n=360) and the medical records reviewed (60 medical records per month from July to December) is high (0.99). The effect size was small to moderate (0.23). The sample size was adequate for the model, at the given parameters, to achieve detection of the small to moderate effect in a sample of 360 medical records and to assess significance of that effect with high power.
The overall rate of skin-to-skin care increased by 25% across post-intervention months compared with baseline. This improvement resulted from the cesarean population. The overall observed rate of skin-to-skin care before the intervention was higher in vaginal births (n=28; 93%) than in cesarean births (n=7; 23%), indicating the need for a larger sample size to identify significant improvements in the vaginal population.
Skin-to-skin care during cesarean surgery had not been offered at the study site prior to this study, although sometimes it was offered during recovery. Little research has been conducted on skin-to-skin care after cesarean surgery,3,31–33 despite recent BFHI standards. 1 According to the national coordinator of Baby-Friendly USA, several hospitals have implemented skin-to-skin care during cesarean surgery (C. Turner-Maffei, personal communication, June 2010). The process of offering skin-to-skin during cesarean surgery may have raised awareness of the need to provide skin-to-skin care for all mothers undergoing cesarean section, at least during recovery, contributing to improvements and sustainability.
Differences in the rate of exclusive breastfeeding at hospital discharge may have been apparent had birth mode (vaginal versus cesarean) been available. Data now are collected by birth mode (beginning in January 2010).
Nine instinctive stages during skin-to-skin care
While experiencing skin-to-skin, newborns move through nine observable stages, awakening breastfeeding reflexes and leading to self-attachment and suckling 16 (Table 1). With the help of the PRECESS experts and the study team, staff and parents identified stages as babies exhibited the behaviors and staff began discussing skin-to-skin care and the nine stages during admission to labor and delivery. After the PRECESS intervention, the childbirth educators began teaching parents about the nine instinctive stages and providing informational tear sheets 28 during prenatal education classes.
Skin-to-skin stages and breastfeeding
During the PRECESS intervention, five of the six babies who experienced the nine stages during skin-to-skin care were exclusively breastfed at hospital discharge. Although the sample was small, these results are consistent with the new skin-to-skin care standard1,2 that calls for staff to support mothers and newborns as newborns move through the instinctive stages at their own pace. Labor and delivery nurses from the study site and from other hospitals within the healthcare system applying for Baby-Friendly designation reported feeling pressure to document that babies breastfed within an hour of their birth. Because breastfeeding reflexes may be depressed at birth, 16 this practice hinders rather than enhances breastfeeding outcomes. Additionally, duration of skin-to-skin has been shown to have a dose–response effect—with longer durations (up to 3 hours) associated with higher rates of exclusive breastfeeding at hospital discharge. 4 This implies that supporting the process of skin-to-skin care may be as important, or more important, than documenting that breastfeeding occurred within 30–60 minutes of birth.
Staffing barriers
Safe care requires nurses' undivided attention while mothers hold their babies skin-to-skin after vaginal and cesarean births. Labor and delivery nurses frequently described staffing issues as one barrier to immediate, uninterrupted skin-to-skin care. In the current study, although a second registered nurse had been added to standard staffing in LDR or OR to assist the primary nurse, this second registered nurse typically left shortly after birth to assist with another birth when no problems were apparent. Some nurses, when left alone with the typical responsibilities surrounding birth (e.g., completing maternal and newborn assessments, managing high-alert medications, documenting), may think that they do not have the time to adequately monitor newborns during skin-to-skin care and may choose to leave newborns in a warmer with protective sides.
Recently published guidelines for safe staffing recommend that two registered nurses be present during vaginal and cesarean births and during the immediate recovery period—one for the mother and one for the baby. 34 The immediate recovery period was not defined by a specific length of time, but as patient-specific. The nurse assigned to the baby during cesarean surgery should remain in the surgical suite.
The primary care nurse accepts the newborn as part of her patient assignment only after the initial maternal assessment has been documented, maternal repair, if required, has been completed, and the baby's nurse has documented the newborn's initial assessment, given report, and safely transferred the newborn's care to the mother's nurse. 34 These guidelines were endorsed by the American Nurses Association, American College of Nurse Midwives, the National Association of Neonatal Nurses, and the March of Dimes. 34 Following these guidelines would enhance implementation of optimal skin-to-skin care after vaginal birth and cesarean surgery.
Other outcomes
Clinical staff at the study site were concerned about the rate of maternal hypothermia following cesarean surgery. Although monitoring maternal or newborn temperatures was not a component of this study, staff noted that the five mothers who held their babies skin-to-skin during surgery and recovery maintained their body temperatures—as did their babies. With this observation as part of the stimulus, direct care nurses conducted educational sessions to promote skin-to-skin care after cesarean surgery, 2 months after the PRECESS intervention. They used a poster with photographs from the PRECESS intervention to illustrate strategies for safe skin-to-skin care during cesarean surgery. The education was like a “booster shot” and built on the momentum of the PRECESS intervention—possibly contributing to the sustainability of improvements.
Limitations
Results from our sample of 11 women were clinically relevant. The small sample size is appropriate for ethnographic projects. For Part 2, we obtained rates of skin-to-skin care and breastmilk feeding at hospital discharge from monthly quality improvement data routinely collected by electronic record review. The data were originally collected for reasons other than our research and thus have weaknesses common in retrospective studies. Because the individuals providing the data were not trained to collect the information in a consistent manner for the purpose of our research, the quality of the documentation varied and was sometimes incomplete or unavailable. Some of the data may have been inaccurate. Although the monthly exclusive breastmilk feeding rates were based on all eligible babies, the monthly skin-to-skin rates were based on a convenience sample of only 60 electronic health records each month. A larger sample size was needed for women having vaginal birth to identify differences in skin-to-skin monthly rates before and after the intervention because the rate of skin-to-skin prior to the intervention already was high (93%). Data on start time of skin-to-skin care following birth and duration of skin-to-skin care were not precisely recorded, so a determination of the average time after birth that skin-to-skin care began or the average duration (dose) of skin-to-skin care was not possible.
The presence of experts who attended each birth and provided advice and coaching during clinical care might have modified the behavior of those present. The video-recording also may have influenced behavior.
Recommendations
Based on our clinical experiences and those of colleagues, many healthcare professionals and parents do not know that skin-to-skin care improves outcomes for all women—not just those who plan to breastfeed. We must ensure that all clinicians, nurses, and parents know the health benefits of immediate, uninterrupted skin-to-skin care with their babies after birth for at least an hour—and until after the first feeding for breastfeeding women. We should include information about immediate skin-to-skin care and the newborns' nine instinctive developmental stages in formal and informal staff and parent education.
Hurrying the baby to the breast is a misunderstanding of Step 4 (early initiation of breastfeeding after birth) of the BFHI. 1 Healthcare professionals should help mothers to position their baby so that their baby can move to the breast and latch, when ready, and to recognize when their babies are ready to breastfeed.
The international experts were surprised by the frequency of medication use during labor and the number of babies who did not complete the nine stages during skin-to-skin. We recommend studying the relationship between labor anesthesia and analgesia and newborns' nine instinctive stages during skin-to-skin care.
The PRECESS method may help identify barriers to and strategies for implementing change in short periods. We recommend studying the effectiveness of the PRECESS method for creating sustainable change in a short time. We also suggest increasing the use of video-feedback with reflection and interactive analysis for a variety of quality improvement efforts.
Research is needed in many areas to improve skin-to-skin care and breastfeeding. We recommend studying skin-to-skin rates for all women and babies, regardless of feeding choice. It is important to assess the relationship of skin-to-skin care duration, newborns' developmental stages during skin-to-skin care, exclusive breastfeeding at hospital discharge, and birth mode. Investigation of the effect of skin-to-skin care during cesarean surgery on maternal stress, nausea, hypothermia, satisfaction with the surgical experience, and exclusive breastmilk feeding at hospital discharge is needed.
Interprofessional communication among all stakeholders enhances the success of quality improvement initiatives. We discussed the project with, and obtained letters of support from, the directors of nursing, anesthesiology, and obstetrics departments. However, we did not discuss the project with the director of pediatrics because we had excluded compromised babies requiring pediatric care immediately following birth from the study. Several neonatologists learned of our project a week before it began and had concerns about the safety of skin-to-skin care during cesarean surgery. Their concerns could have been addressed sooner if we had discussed the project with them in advance.
Conclusions
The PRECESS method was effective for improving the rate of skin-to-skin care immediately after birth. Babies who undergo all nine stages during skin-to-skin may be more likely to be exclusively breastfed at hospital discharge. Clinicians and nurses, educated about the nine instinctive stages of the newborn during skin-to-skin care, may be more effective at providing appropriate clinical care. The focus needs to be changed from “getting babies on the breast” immediately after birth to supporting mothers and babies during skin-to-skin care and helping mothers to breastfeed when their babies show signs of readiness. Skin-to-skin care may reduce maternal stress and improve satisfaction with during cesarean surgery.
Footnotes
Acknowledgments
The authors thank Armara Dickey, B.S.N., Carol Gentry, M.S.N., Renee Jones, M.S.N., and Nuala Murphy for participating on the study team; LaVona Wilkes, M.S.N., for data support; Mary Ann Faucher, Ph.D., C.N.M., for reviewing and critiquing an early draft of the manuscript; Cole Edmonson, D.N.P., Debra Maitre, M.S., June Marshall, D.N.P., and the physician department directors for administrative support; nurses and physicians who supported the project; and the patients and their families who participated in the study.
Disclosure Statement
No competing financial interests exist.