
Abstract
Abstract
Evidence continues to accumulate showing the benefits of breastfeeding to infants, mothers, and society as a whole. However, breastfeeding success rates nationwide have consistently fallen short of recommendations set forth by the American Academy of Pediatrics. There are several potential barriers to successful breastfeeding, and many of these could be magnified in the demanding careers of military members and their families. We surveyed 254 women at a regional military medical facility, both active duty members and dependents of active duty members, regarding their ability to successfully breastfeed their infants. We found that American Academy of Pediatrics target goals in this population as a whole were indeed nearly met at this facility, but also found that active duty members and those who encountered military-related difficulty fell well short of these goals. These findings suggest potential barriers to breastfeeding success that warrant further study from the U.S. Department of Defense.
Introduction
Much has been done in recent years to strengthen the support for women to breastfeed. One important place for a woman to receive such support is through her hospital prior to and after delivery. The Baby-Friendly Hospital Initiative is a global program sponsored by the World Health Organization and the UNICEF to encourage and recognize hospitals and birthing centers that offer an optimal level of care for infant feeding. There are 10 steps outlined that must be accomplished in order to achieve the Baby-Friendly Award. These include having a written breastfeeding policy, training all healthcare staff in skills necessary to implement this policy, informing all pregnant women about the benefits of breastfeeding, helping mothers breastfeed their babies within 1 hour after birth, showing mothers how to breastfeed and how to maintain lactation even if separated from their infants, giving newborns no food or drink other than breastmilk unless medically indicated, practicing “rooming in” to allow mothers and infants to remain together 24 hours a day, encouraging “breastfeeding on demand,” giving no pacifiers to breastfeeding newborns, and fostering the establishment of breastfeeding support groups and referring mothers to them on discharge from the hospital or clinic. 4 On January 20, 2011, Surgeon General Regina M. Benjamin released The Surgeon General's Call to Action to Support Breastfeeding. This report encouraged education, support, additional research, and promotion of breastfeeding in the home, workplace and healthcare settings. 5 Because of the increased social awareness due to these types of initiatives, more women are choosing to breastfeed their infants after delivery. However, there is evidence that shows that many of these women fail to complete the recommended duration of breastfeeding set forth by the American Academy of Pediatrics. In 1996, 59% of U.S. women initiated breastfeeding after delivery, but only 22% continued to 6 months. 6 In 2000, 68% of mothers initiated breastfeeding in the early postpartum period, but only 31% continued to 6 months of age and 17% to 12 months. 7 More recent data (2006) show marginal improvement where 73.9% of U.S. women initiated breastfeeding, 43.4% continued to 6 months, but only 22.7% continued to 12 months. 7
The U.S. Department of Health and Human Services has set forth goals to increase the incidence of breastfeeding. In a Surgeon General's report, titled Healthy People 2020, the recommended goal based on previous percentages and realistic increases as determined by the authors was to have 82% of mothers' breastfeeding at the early postpartum period, 61% at 6 months, and 34% at 12 months. 7 This was increased from the goals set in the preceding report written in 1998, Healthy People 2010, the guidelines used during the time frame of this study; the recommended 2010 goals were to have 75% of women start breastfeeding in the early postpartum period, 50% continue to 6 months, and 25% continue breastfeeding at 1 year. 8 Data show that many women fail to reach the Healthy People 2020 goals. 7 There are several possible reasons for this failure both at home and at work. Patients have cited short maternity leave, inadequate milk supply, inability or lack of access to a pump, insufficient time and support at work, pressure from others to wean, fatigue, and lack of time among other reasons for termination. 9 These same factors are relevant to the military population, for both active duty members and dependents of active duty members. However, the military is unique in the fact that there are additional factors relating to deployment, mission requirements, limitations on maternity leave, extra duty, extended hours, and potential exposure to a predominantly male work environment that may further hinder a patient's ability to successfully breastfeed for the desired duration. Although the military hospital we studied does not meet all of the criteria to be recognized by the Baby-Friendly Hospital Initiative, there are military hospitals on the list, such as Naval Hospital Jacksonville and Weed Army Community Hospital. Indeed, the potential to fall short of the goals set forth may prove to be greater among patients in a military population. Demographic statistics alone show lower rates of breastfeeding in lower-income mothers, minority mothers, and in those with less than a college education. 6 These subgroups of the population are well represented in the military. Military job requirements could also provide a barrier to a breastfeeding mother. Active duty mothers are required to return to duty at 6 weeks postpartum and are eligible for deployment (worldwide qualified) as early as 4 months postpartum. 6 The dependent wife of an active duty member may also find that the deployment of her spouse eliminates the needed support at home to continue breastfeeding. In a series of interviews of active duty women conducted by Stevens and Janke, 10 several different barriers to breastfeeding were noted. Of those unique to the military lifestyle, temporary duty separations or fear of such ranked as a common hindrance, as well as additional duties and required exercises/war games. 10
To the credit of the U.S. Department of Defense (DoD), there have been measures implemented to provide assistance to breastfeeding mothers. In 2001, breastfeeding counseling became part of TRICARE's (the military's health insurance provider) well-child program. 6 A survey performed by Bell and Ritchie 6 showed that 95% of military installations employed a lactation consultant and that a similar number had prenatal breastfeeding classes available to the population. All of these surveyed facilities allowed for “rooming in” of an infant with the mother (allowing the infant to stay in the mother's room postpartum), and 68% had a designated lactation room set aside for proper privacy for both patients and staff. All of these policies should improve breastfeeding, but have they actually been effective? In an unpublished Naval study cited by Bell and Ritchie, 6 65% of respondents did indeed initiate breastfeeding early in the postpartum period, but only 21% were able to continue for more than 3 months. These numbers were well below the national average and fell far short of the Healthy People 2020 goals. 7 This may confirm that military mothers do indeed encounter more difficulties in maintaining proper duration of breastfeeding than nonmilitary mothers; however, follow-up data on the subject have been rather lacking.
The purpose of this study is to evaluate breastfeeding rates in a military population at a regional military medical center, both active duty and dependents, with attention to duration of breastfeeding and potential factors relating to military job requirements that could hinder a mother's ability to achieve proper breastfeeding goals.
Subjects and Methods
Eglin Air Force Base Hospital in Florida is a regional teaching facility that supports an average of 70–80 deliveries per month and is home to a family medicine residency program. The facility offers prenatal counseling and education for mothers who choose to breastfeed and also employs a full-time lactation consultant. Postpartum patients are allowed to room in with their infants, and the hospital has a designated lactation room for patients and staff. In addition, several of the affiliated outpatient clinics have designated lactation liaisons that work in cohort with the lactation consultant to answer specific questions from patients regarding breastfeeding. Active effort is used to ensure that patients initiate breastfeeding within 1 hour of birth, and pacifier use is discouraged.
We chose a 13-month time period extending from October 2001 to October 2002 to select our study population. This time period was ideal because we felt that with increasing deployments and mission readiness after the September 11, 2001 tragedy, the hindering factors unique to the military lifestyle would be prominent. The measures mentioned above implemented by the DoD would therefore be put to the test. Appropriate Institutional Review Board protocol was followed to gain approval for the study. The target population was mothers who delivered at the facility during this time period and chose, either prenatally or immediately after delivery, to breastfeed their newborn. K.B. and J.W. personally contacted each woman meeting these criteria by telephone using labor and delivery records and computerized information on the Composite Health Care System database. The telephone survey period of October 2003–April 2004 was chosen to ensure all participants were at least 12 months postpartum. The women verbally completed a brief telephone survey regarding their breastfeeding experience. The questions focused on how long each patient was able to breastfeed, if the patient achieved her personal breastfeeding goal (which was subjectively determined by each participant), which one specific factor most contributed to her decision to stop breastfeeding, if she was seen by a lactation consultant within 48 hours of delivery, and if she completed the prenatal breastfeeding class offered by the hospital. The patients were also asked specifically if the military job requirements of either themselves or their spouse hindered their ability to successfully breastfeed. Each answer was recorded, and each survey was labeled with a code in order to protect confidentiality and avoid distortion of results. Prior to initiating the telephone survey each patient gave verbal consent. In addition to the questions above, patients were given the opportunity to provide any other feedback or comments relating to their breastfeeding experience. Patients were excluded from the study if their newborn had experienced any prolonged separation from the mother during the perinatal period, such as extended stays in the Neonatal Intensive Care Unit or transfer to a specialty hospital.
Raw data were entered into a spreadsheet for analysis. Frequency distributions were run to calculate simple percentages. In addition, several relationships were tested using χ2 analysis. Power calculations were performed to determine if appropriate power was achieved for medium effect size for each group comparison. All analyses were performed using SPSS version 11.0 software.
Results
During the time period specified, there were a total of 973 deliveries, averaging 74.8 per month. Of those women who delivered, 76.9% (749) elected to breastfeed. Use of a standard survey test revealed that in order to be able to generalize our results to the total population of breastfeeding mothers who delivered during the research period, with a 95% confidence interval of±5%, a total of 254 surveys would be needed. 11 Of those, 234 answered as to whether or not their personal duration goal was met (the remaining 22 were still breastfeeding at the time of the survey and did not give an answer to this question). In this subgroup, 63.2% stated that their personal goal was not met. Eighty-six (36.8%) patients met their goal, but only 55 of these actually stopped breastfeeding because they met their predetermined goal; the other 32 patients gave a different reason for cessation.
Reasons for cessation of breastfeeding were as follows: maternal difficulty (pain, infection, illness), 23.7%; predetermined goal met, 23.3%; job-related difficulty, 14.7%; mechanical difficulty (latching on, biting, no longer taking breastmilk), 13.1%; too inconvenient, 10.3%; too stressful, 3.6%; deployment of spouse, 2.4%; feeling that formula was more beneficial, 2.4%; deployment of mother, 1.6%; no access to pump, 0.4%; and lack of family support, 0.4% (Fig. 1).
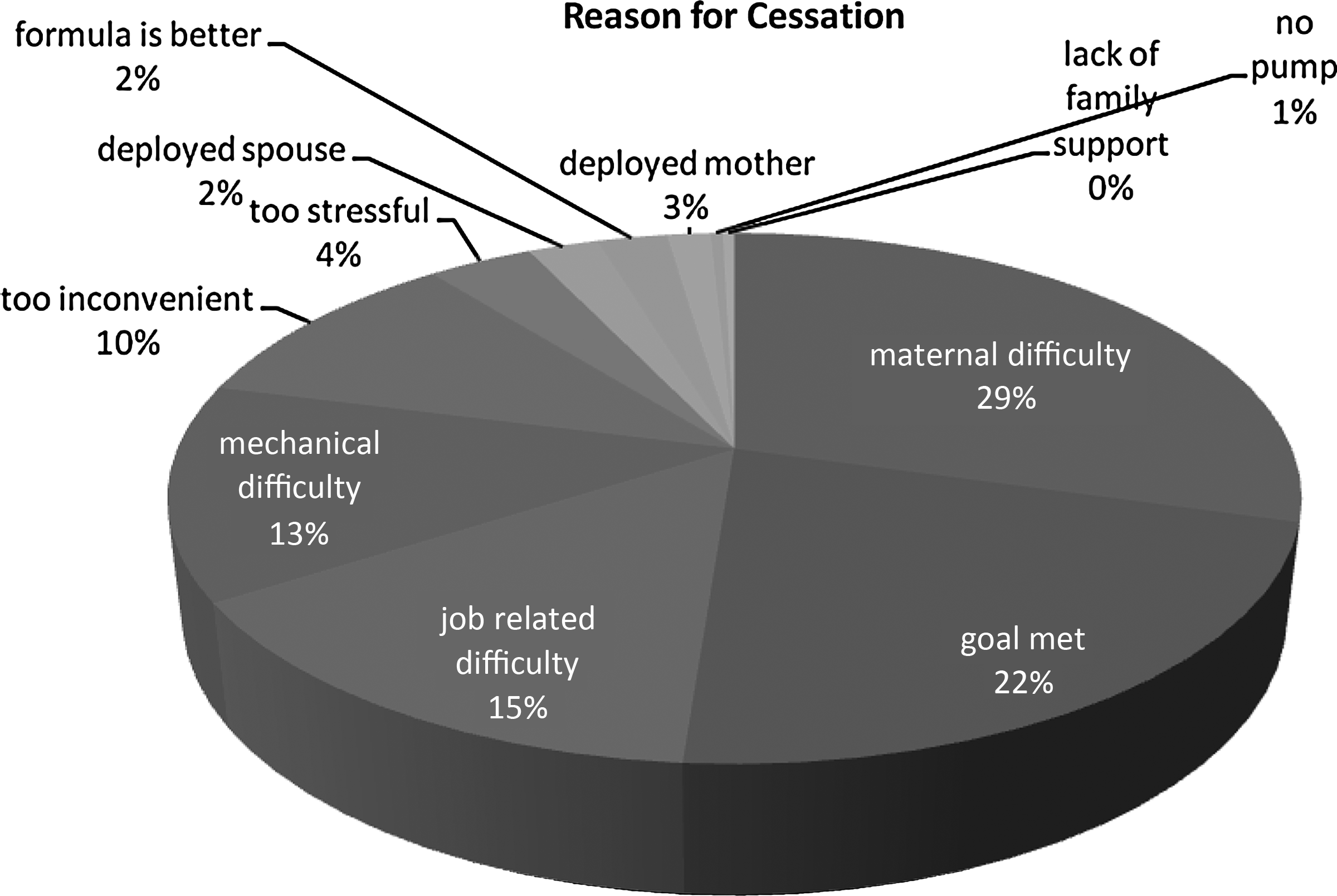
Reasons given for cessation of breastfeeding.
Of the 254 patients surveyed, 136 (53.5%) were able to breastfeed for 6 months or longer, whereas 71 (27.9%) were able to breastfeed for 12 months or longer (Fig. 2). All surveyed patients answered as to whether or not the military job requirements of themselves or their spouse hindered breastfeeding. Two hundred fifteen (84.6%) felt that the military was not a hindrance in any way. Forty-three (16.9%) of the total patients surveyed were on active duty.
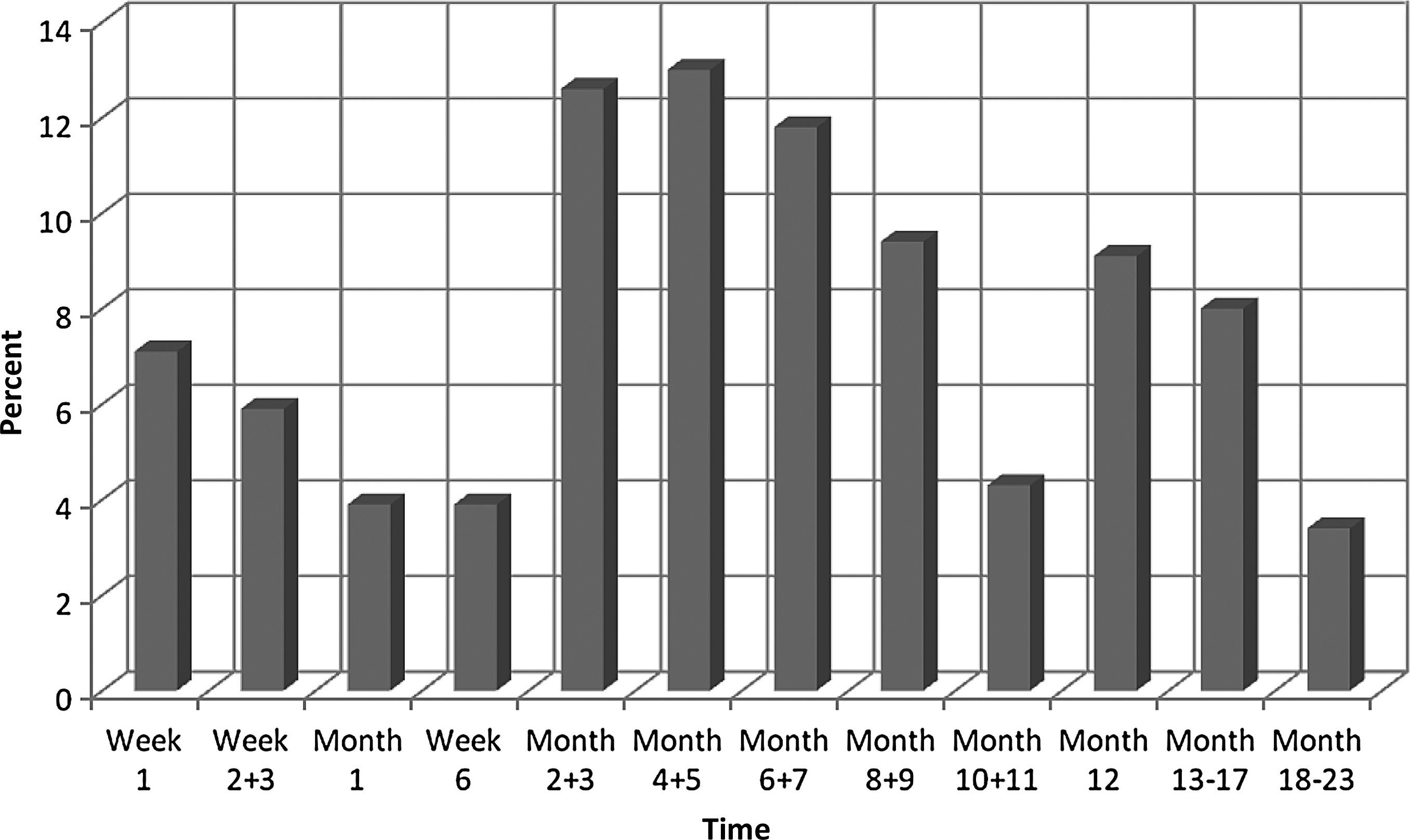
Percentage of women who stopped breastfeeding at any given time.
Of the active duty patients, 31% (13) stated that they were able to meet their breastfeeding goal, whereas 37.9% (72) of the non–active duty population stated the same. A χ2 analysis showed no statistical significance between being active duty and achieving a personal breastfeeding goal. Power calculation confirmed that we were unable to achieve adequate power for medium effect size because of the disproportionate distribution of patients between the two groups.
Of the active duty patients, only 17 (39.5%) stated that they were able to breastfeed for 6 months or more, whereas six (13.9% of total) were able to continue to 12 months or more. In the non–active duty population, 118 (56.5%) were able to breastfeed for 6 months or more, and 65 (31%) continued to 12 months. A χ2 analysis was performed and showed statistical significance between being active duty and breastfeeding for 6 months or more [χ2=4.107(1), p=0.043].
All patients answered as to whether or not they were seen by a lactation consultant within 48 hours of delivery, the usual time period spent in the hospital prior to discharge. Of these, 86.2% (n=219) stated that a lactation consultant within this time frame saw them. Of the patients who were seen by the lactation consultant, 37.9% (n=78) met their goal, whereas 28.6% of the patients not seen met their goal. Again, a χ2 analysis was performed, and there was no significant difference found in relation to being seen early by a lactation consultant and achieving a personal breastfeeding goal, but a power calculation showed that again we were unable to achieve adequate power for medium effect size because of disproportionate distribution between the two groups.
Of the patients who were seen by a lactation consultant within 48 hours of delivery, 116 (53%) were able to breastfeed for 6 months or longer, whereas 57 (26%) continued for 12 months or longer. Twenty (57.1%) patients not seen by a lactation specialist within 48 hours were able to continue for 6 months or longer, whereas fourteen (40%) continued for 12 months. A χ2 analysis was performed and showed no significant difference in relation to being seen early by a lactation consultant and breastfeeding for 6 months or longer; but again adequate power for medium effect size was not achieved because of disproportionate distribution between the two groups.
All patients answered as to whether or not they attended the prenatal breastfeeding class offered by the medical facility. Of these, 36.6% (93) stated that they did attend the class. Twenty-eight (30.1%) of the patients who attended the class were able to meet their goal, whereas 36% (n=58) of the patients who did not attend were able to do the same. A χ2 analysis showed no statistical significance between attending the class and achieving a personal breastfeeding goal, and a power calculation confirmed adequate power for medium effect size and thus served as validation for this finding.
Of the patients who attended the breastfeeding class, 46 (49.5%) continued for 12 months or longer. Ninety (55.9%) of the patients who did not attend the class continued breastfeeding for 6 months or longer, whereas 49 (30%) continued for 12 months or longer. A χ2 analysis showed no statistical significance between attending the class and breastfeeding for 6 months or longer, and power calculation confirmed adequate power for medium effect size and thus could also validate this finding.
A final subgroup was put together in order to determine if the DoD could potentially improve breastfeeding numbers with policy. This group consisted of all patients who answered that the military job requirements of themselves or their spouse acted as a hindrance to successful breastfeeding, any active duty patient who stated that she ceased breastfeeding because of work-related difficulty, patients who ceased because of their own deployment, patients who ceased because of the deployment of their spouse, and patients who ceased because of lack of access to a breast pump. There were 48 patients who fit the criteria for this group. Of those, 19 (39.6%) were able to breastfeed for 6 months or longer, whereas four (8%) continued for 12 months or longer. One hundred seventeen (56.8%) of the patients who did not fit into this category were able to breastfeed for 6 months or longer, whereas 67 (32%) were able to continue for 12 months or longer. A χ2 analysis calculation was performed and showed statistical significance between the two groups [χ2=4.64(1), p=0.031].
Discussion
Our data show that in the time period specified, Eglin Hospital almost met the goals set forth by the U.S. Department of Health and Human Services and the U.S. Surgeon General as outlined in Healthy People 2010, 8 the goals used at the time of our data collection. At this facility, 76.9% of new mothers elected to breastfeed in the early postpartum period. Also, 53.5% of these patients were able to continue breastfeeding for 6 months or longer and 27.9% for 12 months or longer. These numbers surpass similar data regarding the general U.S. population. This implies that the measures implemented by the DoD at Eglin Hospital have indeed been beneficial. One limitation of this study is that it is specific to only one regional military medical facility, so it therefore should not be extrapolated to represent all military medical facilities or the DoD as a whole. Additional studies comparing various populations, such as variations in different branches of service, would be beneficial to obtain additional detailed information.
Our data also suggest that the active duty population served by Eglin Hospital may require additional measures to help them achieve breastfeeding targeted goals, as only 39.5% and 13.9% were able to continue breastfeeding for 6 and 12 months, respectively. This population fell significantly short of the Healthy People 2010 target. 8 We chose the immediate “post 9/11” time period, thinking it was an ideal time to showcase the prominent hindering factors of increased deployments. In retrospect, however, this may in fact be a limitation because the immediate time period after September 11, 2001 was an extraordinary time period that does not necessarily portray the typical military operations tempo. However, over the last decade, the military operations tempo has been in a state of flux and constant change. It would be difficult to define what the “typical” military operations tempo is. Our study sought to evaluate two groups of women: active duty personneland dependents of active duty members. We did not further specify demographic data such as ethnicity, age, education, income, maternity history (such as number of previous children delivered and breastfeeding after previous deliveries), marital status, or branch of service (although being an Air Force base, it consisted of predominantly Air Force members and their dependents). Because the survey was conducted via an unannounced telephone call, brevity was important. Although we felt that, in general, a military population encompasses a wide variety of demographics, none of the data was delineated along those lines. This could be an area of future research.
Further research could also include a survey of women who chose to bottle feed from the beginning. Why did they choose to avoid breastfeeding? Were military factors involved? It would be interesting to compare a bottle feeding study with our survey results. However, this study did not seek to compare bottle feeding versus breastfeeding.
By focusing on specific military factors, we were able to show that there were hindrances at a regional military medical center that are unique to the military that indeed prevented women from achieving the targeted duration. Some of these factors, such as deployment of a member or spouse, and lack of access to a pump could potentially be corrected by a change in DoD policy. However, the other patients in this group—those who stated that the military job requirements of themselves or their spouse hindered their ability to successfully breastfeed and those active duty patients who stated that work-related difficulty was the primary reason for cessation—were somewhat vague in regard to their reported reasons, and additional information would be required before any corrective measures should be implemented. Other patients did comment specifically on what hindrance they encountered. We were told that often there was nowhere to pump, work hours were too long, they faced an upcoming temporary duty assignment, or they felt “uncomfortable” pumping at work. However, these specific comments were limited to a select few patients, and conclusions could not be derived from them. Thus, it seems reasonable for the DoD to perform a larger study, focused on incorporating many military medical facilities and aimed at evaluating the active duty population, as well as patients who encountered military-related difficulties, in order to determine if more effort or policy changes should be implemented to improve breastfeeding rates. So what are the specific policies in place for breastfeeding and pumping in the different DoD services? In 2006, long after the completion of this study, the U.S. Air Force published Air Force Instruction 44-102, 12 giving more specific guidelines on breastfeeding among active duty members. It is now recommended that supervisors of Air Force members who are breastfeeding work with the member to attempt to arrange their work schedules to allow 15–30 minutes every 3-4 hours to pump breastmilk in a room or an area that provides adequate privacy and cleanliness, if available. Restrooms should not be considered an appropriate location for pumping. This is definitely a step in the right direction.
The Army does not have specific guidelines in place for breastfeeding active duty mothers, but they do offer a memorandum for commanders that outlines a plan for the active duty member to pump while at work. In July 2008, the deferral time for deployment was extended from 4 to 6 months after having the baby, so leadership seems to be aware of this need and is making changes. 13 The Marine Corps has a policy in place that states that at a minimum, a woman choosing to breastfeed should be allowed a clean, secluded space in which to do so, and she will not be obligated to deploy until 6 months after the birth of the baby. 14 The Navy's policy is one of the more “mom friendly” of the services. The servicewoman is not required to deploy until 12 months postpartum, and facilities must be available for a clean, secluded place to breastfeed at work, as well as access to cold storage of expressed milk. The time allowed to breastfeed varies and is a collaboration between the servicewoman and her supervisor. 15
In regard to the prenatal breastfeeding class, we found that there was no statistically significant difference between attending the class and achieving appropriate personal goals or recommended target duration. This suggests that the breastfeeding class is not effective in improving breastfeeding rates. However, it should be noted that many of the respondents stated that they had attended the breastfeeding class during a prior pregnancy and therefore elected not to attend the class with their later pregnancy. This could have introduced a significant degree of error into our data. Further research is recommended before definitively determining whether a prenatal breastfeeding introductory class is beneficial to breastfeeding mothers.
A lactation consultant saw an overwhelming majority of our patients within 48 hours of delivery. Because of this disproportion between groups (seen within 48 hours vs. seen after 48 hours), we were unable to achieve adequate power to determine whether or not this had any effect on a woman's ability to achieve either a personal goal or recommended duration of breastfeeding. We did receive numerous comments relating to the lactation consultant, and the majority of these were favorable. While anecdotally the lactation consultant appeared to serve a vital role, more research is required to determine if a military population statistically benefits from access to such a specialist.
Conclusions
As the U.S. military continues to expand the roles of women in the workforce, it must also expand appropriate measures to improve the health and well-being of these women and their children. Breastfeeding has been proven to be beneficial in numerous ways, and increasing breastfeeding rates throughout the DoD will likely prove to be beneficial to the military as a whole. Even though this study shows that an Air Force facility nearly met the Healthy People 2020 goals, 7 it is clear that more can be done to assist our active duty population and to minimize as many barriers as possible within the military as more and more women choose to breastfeed their infants. In addition, although barriers do exist, more evidence is clearly needed, and more studies should be focused on this area before specific problems can be identified and appropriate measures can be implemented to assist our military breastfeeding mothers.
Footnotes
Disclosure Statement
No competing financial interests exist.