
Abstract
Abstract
Aim:
The aims of this study were to analyze the relationship between the LATCH score assessed in the first 24 hours after delivery and non-exclusive breastfeeding at discharge and to identify a cutoff for the LATCH score in order to identify women with higher risk of non-exclusive breastfeeding who may need additional breastfeeding support.
Subjects and Methods:
We conducted a prospective observational study in the Maternity Ward of the Institute for Maternal and Child Health “Burlo Garofolo” (Trieste, Italy) and collected data from 299 mother–infant dyads.
Results:
The rate of nonexclusive breastfeeding was inversely related to the LATCH score (p<0.001) with non-exclusive breastfeeding infants scoring less (6.9) than infants exclusively breastfed at discharge (7.6) (p=0.001). In multivariate analysis, non-exclusive breastfeeding was also associated with cesarean section, primiparity, and infant phototherapy. In order to support maternity staff in providing targeted interventions, we identified four LATCH score cutoffs associated with as many risk groups for non-exclusive breastfeeding at discharge.
Conclusions:
The LATCH score is a useful tool to identify mother–infant pairs who might benefit from additional skilled support in specific subgroups at risk of non-exclusive breastfeeding at discharge. Future research is needed to explore if the LATCH score assessed in the first days of life can also predict the duration of breastfeeding.
Introduction
In developed countries, most deliveries take place in hospital settings. On the one hand, the hospital setting may hinder breastfeeding as a result of ward practices and protocols (i.e., separation of mother and newborn, scheduled feeds, unnecessary breastmilk supplements) 5 and of obstetric management of delivery (vaginal delivery vs. cesarean section [CS], analgesia, etc.). On the other hand, skilled professional and lay interventions provided in the hospital and in community settings during the first days of life have a strong positive influence on both initiation and duration of breastfeeding.6,7 Improved promotion and support of breastfeeding in maternity facilities and the implementation of the Baby-Friendly Hospital Initiative (BFHI) can therefore be effective interventions. 8
Helping mothers breastfeed also entails assessing the latch-on to the breast because this aspect is strongly related to the success of breastfeeding.9,10 An accurate assessment of infant position and latch-on to the breast is an essential task of health professionals 11 also because it provides a subjective assessment of the neurobehavioral development of the newborn, of the mother's ability to manage breastfeeding, and on adequateness of milk intake. All of these factors need to be considered for hospital discharge after childbirth. 12
Therefore, maternity health professionals need reliable, reproducible tools to assess the effectiveness of the feed and to identify mother–infant pairs who need extra support and follow-up. Our Institute for Maternal and Child Health in Trieste, Italy has chosen to adopt the LATCH charting system 13 because of its simplicity.
To date, only two studies have examined the predictive value of LATCH assessment during the hospital stay on the duration of breastfeeding at 6 weeks,14,15 identifying the dyads at risk of non-exclusive breastfeeding who need to be followed up. Nevertheless, to our knowledge neither of the two studies explored the predictive value of LATCH scores on successful breastfeeding at hospital discharge. Moreover, there is no established LATCH score cutoff that can adequately identify the dyads at risk of non-exclusive breastfeeding.
The objective of the present study is to analyze the relationship between the characteristics of the feed assessed using the LATCH score during hospitalization (within 24 hours after delivery) and the failure to exclusively breastfeed at hospital discharge and to identify a cutoff for the LATCH score related to difficulties with exclusive breastfeeding.
Subjects and Methods
LATCH score
The LATCH charting system was developed by Jensen et al. 13 in 1994 based on the model of the Apgar scoring system. Its simplicity makes systematic documentation and communication easy. The system assigns a numerical score (0, 1, or 2) to five key breastfeeding components identified by the letters of the acronym LATCH: “L” is for how well the infant latches onto the breast, “A” is for the amount of audible swallowing noted, “T“ is for the mother's nipple type/condition, “C” is for the mother's level of comfort, and “H” is for the amount of help the mother needs to hold her infant to the breast. The total score ranges from 0 to 10, with the higher score representing successful breastfeeding.
We conducted a prospective observational study from January 1 to March 31, 2010 at the Maternity Ward of the Institute for Maternal and Child Health “Burlo Garofolo.” Training courses on breastfeeding (the BFHI 20-hour course for maternity staff) are periodically held at the Institute. Breastfeeding support skills are provided by registered nurses trained in the BFHI; at present, however, no lactation consultant is employed in the Maternity Ward. Since October 2009, the LATCH card has become part of the medical records of each baby admitted to the Ward.
The new medical record was used to collect data for all newborns and their mothers admitted to the Ward during the study period, with the exclusion of preterm newborns with <36 complete gestational weeks, infants of low birth weight (<2,500 g), and newborn infants with clinically relevant congenital malformations. The nurse staff routinely assessed the LATCH score for each mother–child pair within 24 hours after birth. Partial scores for each item (L, A, T, C, and H) and the total score were recorded for each mother and child pair in a form that was attached to the medical records.
Feeding categories
Infant feeding was assessed at discharge and took into account the whole period from birth to discharge. Four infant feeding categories were used, according to the World Health Organization's definitions 16 : exclusive breastfeeding (only breastmilk, including expressed milk), predominant breastfeeding (breastmilk, including expressed milk, plus other non-nutrient liquid [i.e., water or glucose solution]), complementary feeding (breastmilk sucked or expressed from the breast plus formula), and no breastfeeding (only artificial milk). The study outcome was non-exclusive breastfeeding, defined as the sum of the three categories (predominant breastfeeding, complementary feeding, and no breastfeeding) not included in exclusive breastfeeding.
Data collection
The following data were collected from medical records: (1) infant's date of birth; (2) mother's date of birth, nationality, and schooling; (3) parity and twin pregnancy; (4) birth weight and gestational age; (5) type of delivery (vaginal, elective CS, or emergency CS); (6) Apgar score at 1 and 5 minutes; (7) the LATCH score calculated once within 24 hours after delivery (partial scores for each breastfeeding component and total score); (8) phototherapy (yes vs. no); (9) type of feeding at discharge (exclusive breastfeeding, predominant breastfeeding, complementary feeding, or no breastfeeding); and (10) date of hospital discharge.
All procedures adopted followed the ethical standards of our Institute's Review Board, which approved the study.
Analysis
After a descriptive analysis of the characteristics of the study sample, we conducted a bivariate analysis to study the relation between maternal and newborn characteristics and nonexclusive breastfeeding at discharge. In the analysis, variables were dichotomized: For most variables we followed clinical criteria (type of delivery [CS vs. vaginal delivery], complete gestational age in weeks [≤37 vs. 37], parity [primiparous vs. multiparous], minute 1 and 5 Apgar scores [≤7 vs. >7], phototherapy for neonatal jaundice [yes vs. no]). For maternal age we used a value close to the mean in years (30 vs. ≤30); for mother's schooling, we used the cutoff of the basic formal education in Italy (>8 years vs. ≤8 years); and for nationality of the mother we distinguished Italian versus foreign. The LATCH score was considered as an interval variable ranging between 0 and 10. Differences were evaluated with a χ2 test for categorical variables and with an unpaired nonparametric Wilcoxon's test for continuous variables not distributed normally (verified both visually and with the Kolmogorov–Smirnov test). To identify variables significantly and independently associated with the study outcome (non-exclusive breastfeeding), we performed a multivariate logistic regression analysis, including all the factors previously analyzed. Starting from a saturated model, we adopted a step-down procedure excluding one at the time the factors with the highest p value ≥0.05.
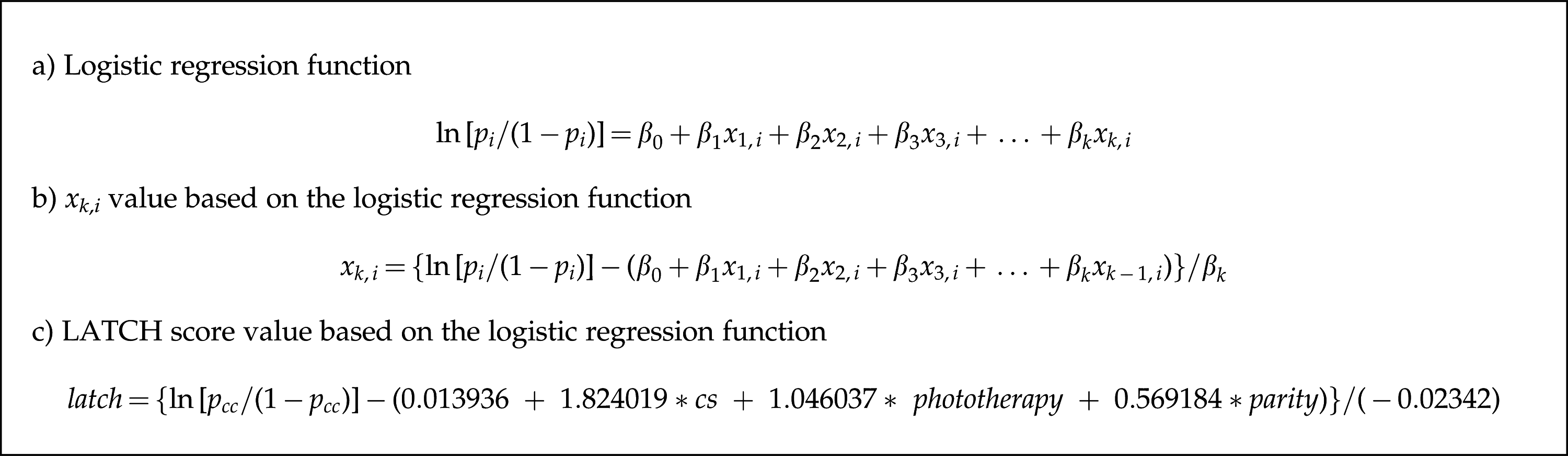
Receiver operating characteristic (ROC) analysis was used to evaluate the sensitivity and specificity of the LATCH score thresholds for predicting non-exclusive breastfeeding at discharge. Subsequently, to identify a cutoff in the LATCH score that could take into account other factors significantly associated with non-exclusive breastfeeding, an ROC analysis was conducted on the logistic regression model resulting from the step-down procedure. We first calculated the predicted probabilities of the outcome resulting from the logistic regression model. Subsequently, we selected the predicted probability value with the highest percentage of correctly classified (true positives and true negatives), and for such a cutoff we calculated the LATCH score value in each category determined by the factors retained in the logistic regression model (see Fig. 1c). We thus found, for each subgroup of women, a cutoff value for the LATCH under which extra support to mother–newborn pairs should be provided as they would be at risk of non-exclusive breastfeeding.
(
Results
Characteristics of the study population
We enrolled 299 consecutively admitted mother–infant dyads. The characteristics of the whole study sample and the feeding category at hospital discharge are reported in Table 1. The average LATCH score value was 7.3, and the non-exclusive breastfeeding rate at discharge was 37.5%.
Data are mean (SD) or number (%) values.
Analysis of the relationship between non-exclusive breastfeeding and potentially predictive variables
Bivariate analysis
The non-exclusive breastfeeding rate was higher among primiparous mothers (47% vs. 28%, p=0.001) and those who had delivered by CS (67% for CS vs. 29% for vaginal, p<0.001).
With regard to newborns, they were more likely to be non-exclusively breastfed if they had lower gestational age (56% among newborn with a gestational age ≤37 weeks vs. 36% among newborns >37 weeks, p=0.04), were subjected to phototherapy for neonatal jaundice (52% vs. 35%, p=0.02), and stayed longer in the hospital (69% for length of stay >4 days vs. 20% for length of stay <4 days, p<0.001).
The rate of non-exclusive breastfeeding was inversely related to the LATCH score (Fig. 2) (p<0.001, χ2 for trend). The mean LATCH score among non-exclusively breastfed newborns (6.9, SD 1.7) was significantly lower than that of newborns breastfed exclusively at discharge (7.6, SD 1.6) (p=0.001).
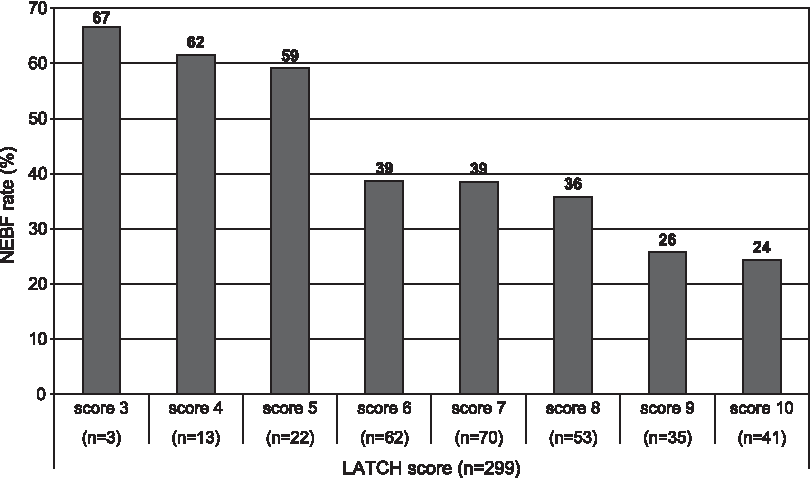
Relationship between LATCH score assessed within 24 hours after delivery and rate of non-exclusive breastfeeding (NEBF) at discharge (χ2 per trend, p=0.001).
Multivariate analysis
In the entire study population (n=299) non-exclusive breastfeeding at hospital discharge was associated with type of delivery (CS vs. vaginal, odds ratio=6.20, 95% confidence interval 3.32–11.57), parity (primiparity vs. multiparity, odds ratio=1.77, 95% confidence interval 1.02–3.07), phototherapy (yes vs. no, odds ratio=2.85, 95% confidence interval 1.45–5.59), and the LATCH score (range 0–10, odds ratio=0.82, 95% confidence interval 0.69–0.96). Considering that non-exclusive breastfeeding was not a rare outcome, we calculated the approximate relative risks corresponding to the adjusted odds ratios 17 : CS versus vaginal, relative risk=2.5, 95% confidence interval 2.0–2.9; phototherapy yes versus no, relative risk=1.7, 95% confidence interval 1.3–2.2; primiparity versus multiparity, relative risk=1.5, 95% confidence interval 1.0–2.0; and LATCH score (range 0–10), relative risk=0.7, 95% confidence interval 0.6–0.8. Gestational age and Apgar at minute 1 were taken into account in the logistic regression model but were not retained in the final model as they lacked statistical significance. Length of stay was excluded from the model because of collinearity.
ROC analysis
At ROC analysis, a LATCH score of <6 identified the highest percentage of correctly classified (true positives and true negatives), with sensitivity and specificity related to the identification of non-exclusive breastfeeding of 20% and 92%, respectively. When considering a LATCH score of <7, as suggested by the literature, we found a sensitivity of 42% and a specificity of 72%.
Because a single cutoff was not sensitive enough to detect non-exclusively breastfed newborns in the bivariate analysis, an ROC analysis was carried out on the multivariate logistic regression model resulting from the step-down procedure. We selected the cutoff that had the highest rate of correctly classified (73.2%), reaching a sensitivity of 66.0%, a specificity of 76.8%, a positive predictive value of 58.9%, and a negative predictive value of 81.7%. The LATCH score was then calculated for this cutoff value for each subgroup generated by the other factors retained in the logistic regression. In this way we found a cutoff value for the LATCH score for each subgroup under which it would be necessary to provide extra support because the mother–newborn pair is at risk of non-exclusive breastfeeding (Table 2).
The major risk factor was cesarean section delivery. Minor risk factors were phototherapy and primiparity.
In women who had had a CS (regardless of phototherapy and/or primiparity) (Group 1) the LATCH score cutoff was 10, meaning that this group should always receive extra support, regardless of the LATCH score. If primiparous women had had a vaginal delivery and the newborn had been subjected to phototherapy (Group 2), the LATCH score cutoff was 9, meaning that this group should be given extra support if the LATCH score is 9 or lower, which is almost always.
In primiparous women with a vaginal delivery and the newborn not subjected to phototherapy (Group 3) and in multiparous women with vaginal delivery and the newborn was subjected to phototherapy (Group 4), the LATCH score cutoffs were 4 and 6, respectively, indicating that maternity staff should consider providing special support to women with LATCH scores equal or lower than cutoff values.
In multiparous women with vaginal delivery whose newborn had not been subjected to phototherapy (Group 5), the LATCH score cutoff was 1, indicating that these women do not need additional support besides standard support to breastfeeding provided in maternity wards.
It is noteworthy that length of hospital stay varied for the different categories in Table 2: The mean length of stay in days was 5.6 (1.0 SD) for Group 1, 4.5 (1.1 SD) for Group 2, 4.2 (1.1 SD) for Group 3, 3.9 (1.2 SD) for Group 4, and 3.4 (1.2 SD) for Group 5. All differences between groups were significant (Mann–Whitney test, with Bonferroni's adjustment for multiple comparisons) except between Groups 2 and 3 and between Groups 3 and 4. This result determines that non-exclusive breastfeeding at discharge was assessed later in the more at-risk groups.
Discussion
In the present study, we chose the LATCH tool to explore the relationship between early breastfeeding assessment during hospital stay and rate of non-exclusive breastfeeding at discharge. The results indicate that the LATCH score in the first 24 hours after delivery can predict breastfeeding at hospital discharge (Fig. 2). Mothers with lower LATCH scores are more likely to feed their newborns in the first days of life with supplements other than their breastmilk, thereby affecting the short-term as well as the long-term success of breastfeeding9,10 and consequently limiting the benefits of breastfeeding to the health of the mother and the child. 1 This result confirms the usefulness of early breastfeeding assessment to identify mothers at risk of non-exclusive breastfeeding and possibly in need of extra support from maternity staff.
Several tools have been developed to assess breastfeeding. Howe et al. 12 have made an accurate review of the existing rating scales for feeding assessment in neonates (EFS, IBFAT, LATCH, MBA, Nomas, PIBBS, and SAIB), describing the main characteristics that make a particular tool useful in research and clinical settings. The first attribute is reliability, which can be measured with the inter-rater agreement at one point in time. The second attribute is validity (i.e., the extent to which the tool measures what it is supposed to measure). The third feature is responsiveness, defined as the ability of an assessment tool to detect changes over time. Unfortunately, evidence on reliability, validity, and responsiveness of each of the above-mentioned tools, including LATCH, is still limited. 12 For the LATCH, discrepancies among studies on its properties may be due to different study designs, sample sizes, and training of staff involved in the assessment. This last issue is particularly relevant as homogeneity in the assessment of LATCH score is essential to increase the reliability of the tool.
Beside those listed and discussed by Howe et al., 12 we should also mention two qualitative checklists: the B.R.E.A.S.T. scale, a 26-item grid developed by IBFAN/UNICEF 18 and recommended by World Health Organization/UNICEF training course on breastfeeding, 5 and the Mother–Infant Breastfeeding Progress Tool (MIBPT) developed to assess maternal and infant breastfeeding progress. 19 The B.R.E.A.S.T. scale has been widely used by experts in breastfeeding practice. Notwithstanding such a huge experience mostly due to the BFHI, this scale appears to be scarcely supported by evidence in literature.20,21 The MIBPT is an eight-item tool developed recognizing that both the mother and the infant contribute to the success of breastfeeding and, in our opinion, has the potential to be effective in assessing breastfeeding. However, to date no studies have been published on MIBPT after the article by Johnson et al. 19 and a report by some of the same authors not primarily intended to explore the validity of MIBPT. 22
Despite some inconsistencies in reliability and validity12,23 and some doubts on predictivity of breastfeeding duration, 24 the LATCH tool is widely used in clinical practice to identify areas that require intervention and to improve patient care and training, 13 as well as in scientific literature.25,26 For example, latch-on to the breast, assessed using the LATCH score, has been shown to be negatively influenced by labor epidural anesthesia and CS,25,27 whereas a higher LATCH score in the first days postpartum is positively related with maternal satisfaction.28,29 Recently, Geddes et al. 26 and Srinavasan et al. 30 in their studies, carried out in Australia and Canada, respectively, reported that the LATCH score increases after frenulotomy in infants with poor latch-on to the breast due to ankyloglossia, thus documenting that the LATCH tool is sensitive enough to detect differences before versus after treatment.
Riordan et al. 14 and Kumar et al. 15 studied whether LATCH assessment during hospital stay predicted breastfeeding duration, evaluated at 6 weeks. The first study obtained LATCH scores from a single random feed between 24 and 72 hours after delivery; the second performed at least one score every 8 hours, including an assessment within the first 24 hours. They both concluded that higher LATCH scores were associated with longer breastfeeding duration. However, Kumar et al. 15 reported only a modest predictivity of the LATCH, stating that breastfeeding duration in influenced by multiple factors such as returning to work or having intended to breastfeed for only a short period of time.
Since the first days of life are crucial for the initiation and the duration of breastfeeding,6,7 we believe it is important to understand the role of an early LATCH score in the prediction of exclusive breastfeeding at discharge.
In the present study, breastfeeding success at discharge was predicted by assessment of the latch-on to the breast in the first 24 hours.
Like Kumar et al, 15 we also identified other independent predictors of non-exclusive breastfeeding: CS (which resulted to be the major risk factor [relative risk=2.5]), phototherapy (relative risk=1.7), and primiparity (relative risk=1.5). These conditions are possibly associated with breastfeeding problems often leading to the use of breastmilk substitutes and glucose solution.
CS may interfere in several ways with breastfeeding: Higher levels of pain and stress, delayed initiation of lactation, 31 longer interval between birth and first feed,32,33 and greater neonatal birth weight loss, 34 all of which may lead to the use of breastmilk substitutes. 35
The need for phototherapy is another relevant factor influencing the initiation of breastfeeding. In fact, intention to exclusively breastfeed associated with delayed lactogenesis and poor latch-on to the breast can increase the risk of early-onset hyperbilirubinemia to the extent that phototherapy may be prescribed, thereby interfering with continuous mother-to-baby contact and exclusive breastfeeding on demand.36,37
Parity also strongly influences breastfeeding success. Multiparae have shorter labor, less need for delivery analgesia, earlier lactation onset (lactogenesis II), and, possibly, previous experience with breastfeeding. All these factors can positively influence breastfeeding initiation and duration. 38
With respect to the identification of a cutoff value that could help identify mothers at risk of non-exclusive breastfeeding, Kumar et al. 15 reported that a LATCH score of 9 or higher, assessed between 16 and 24 hours of age, can identify mothers who will still breastfeed at 6 weeks with a sensitivity of 75% and specificity of 63.2%. This cutoff value, however, serves no useful purpose in clinical practice because it is so high in the scale that the vast majority of dyads would be at risk of non-exclusive breastfeeding.
In our study, we were not able to identify a single LATCH score cutoff that could consistently predict non-exclusive breastfeeding at discharge. In general, we observed that the LATCH score has a low sensitivity for non-exclusive breastfeeding, as reported by other authors. 15 Nevertheless, taking into account other risk factors associated with non-exclusive breastfeeding (CS, phototherapy, primiparity) we identified LATCH score cutoff values that performed better in terms of sensitivity and specificity. We identified three groups of mother–infant dyads at risk of non-exclusive breastfeeding at discharge, considering CS as a major risk factor and phototherapy and primiparity as minor risk factors (Table 2).
In the high-risk group (presenting the major risk factor or both minor risk factors), extra support should be provided regardless of the value of LATCH score, which becomes irrelevant in predicting non-exclusive breastfeeding if the woman delivered via CS, whereas in the presence of both minor risk factors extra support should be provided to all women with a LATCH score of 9 or below.
In the moderate-risk group (presence of one minor risk factor) the LATCH score acquires significance in the prediction of non-exclusive breastfeeding at discharge because a value of the LATCH score equal to or below the reported cutoff (6 when the minor risk factor is phototherapy, 4 when the minor risk factor is primiparity) puts these dyads in a condition of higher risk.
In the low-risk group (no risk factor) women do not require special attention. Obviously, maternity staff should provide appropriate basic support to all women.
The purpose of identifying risk groups is not that of giving less breastfeeding support to some women; on the contrary, we believe that our findings help identify mothers and infants at higher risk of breastfeeding failure who need more support during hospitalization.
We are aware that the present study has some limitations. We did not explore to what extent the LATCH score can predict breastfeeding success after discharge (i.e., on the mid/long-term basis) as we decided to focus our attention and resources on hospital organization and practices. Furthermore, we are aware that an inter-rater reliability study for the LATCH tool is needed, and our research group is about to complete a research project on this aspect.
The fact that non-exclusive breastfeeding at discharge was assessed later for the groups more at risk according to Table 2 (more at-risk groups having longer mean hospital stay) should be considered positively for our results because breastfeeding in the first days after birth tends to increase because of the increase in the prevalence of women with lactogenesis stage II.
Our institution has a long-lasting tradition in breastfeeding promotion and support. Nevertheless, it was never designated as Baby Friendly and never even entered the BFHI accreditation process. Currently, no health professional has the International Board Certified Lactation Consultant qualification. In the light of these facts, we believe our results may also be applicable to hospitals with different degrees of breastfeeding support. In fact, we simply tested a method that can help identify more vulnerable dyads in need of special breastfeeding support.
Conclusions
The present study shows that the LATCH score is a useful tool to identify mother–infant pairs who might benefit from special skilled support in specific subgroups. According to our experience, the LATCH score represents a simple, effective tool for health professionals to assess breastfeeding in maternity wards, in particular, for recording data, transferring information to colleagues, and monitoring breastfeeding more objectively.
Further research is needed to study if specific subgroups of mothers targeted for extra support improve their outcomes and if the LATCH score used in the first days of life—before hospital discharge—can also predict the duration of breastfeeding after discharge. Moreover, more evidence on the reliability of the LATCH tool should be gathered.
Footnotes
Acknowledgments
The authors wish to thank the mothers who participated in the study and all the nurses of the maternity ward who factually contributed to the survey. We would also like to thank Barbara Franzelli for her generous help in the collection of medical records. This work has been made possible by a research grant from the Institute for Maternal and Child Health “Burlo Garofolo,” Trieste, Italy.
Disclosure Statement
No competing financial interests exist.