
Abstract
Abstract
Background:
Maternal smoking during pregnancy is associated with a variety of risks on fetal health, whereas breastfeeding may protect infants from infections in the early postpartum period. Little has been reported regarding their associations with children's general health later in childhood.
Subjects and Methods:
Parent-rated children's general health status was investigated among 14,836 children and adolescents 3–17 years old who participated in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) in 2003–2006. Data on breastfeeding and maternal smoking during pregnancy were collected by parent-administered questionnaires. SPSS complex samples logistic regression was used to estimate odds ratios (ORs) and 95% confidence intervals (95% CIs).
Results:
Exclusive breastfeeding and non-exposure to maternal smoking during pregnancy were associated with better health status overall among all children in the KiGGS (both p<0.001). After adjusting for potential confounding factors including other prior and current exposures, exclusive breastfeeding over 6 months remained significant overall among all children (OR 1.21, 95% CI 1.05–1.38) and in the age groups 7–10 years (OR 1.27, 95% CI 1.01–1.60) and 11–17 years (OR 1.23, 95% CI 1.01–1.50), while non-exposure to maternal smoking during pregnancy remained significant in the age group 11–17 years only (OR 1.49, 95% CI 1.06–2.10).
Conclusions:
Exclusive breastfeeding and non-exposure to maternal smoking during pregnancy may be associated with better children's general health status later in childhood, particularly when children reach adolescence. Further studies are required to elucidate these possible and biologically plausible associations. Health professionals should take opportunities to promote breastfeeding and cessation of smoking among (expectant) mothers for a healthy future of their children.
Introduction
The World Health Organization recommends that infants be breastfed exclusively for the first 6 months of life. 1 Following this recommendation, the German National Breastfeeding Committee issued guidelines in 2004, recommending that complementary feeding should be initiated no earlier than 5 full months but no later than 7 months of age. 8 In addition, health professionals continue to warn pregnant women of the dangers of smoking. In spite of this, rates of exclusive breastfeeding over 6 months are rather low in developed countries,9,10 including Germany, 11 and a substantial portion of women (range, 11–36%) still smoke during pregnancy.12,13 Reasons for this are various; one of them may be that young (expectant) mothers do not adequately recognize the long-term effects of breastfeeding14–16 and maternal smoking during pregnancy5,6,17 on their children's general health later in life.
Children's general health status is an important health indicator that has been widely investigated in national health surveys and found to be associated with a broad spectrum of factors.18–22 Our own previous studies found that it is closely associated with medication use and predicted pain in children.23,24 So far, little has been reported regarding its possible associations with children's prior exposures to risk or protective factors. In the present study, we investigated the association of breastfeeding and exposure to maternal smoking during pregnancy with children's general health later in childhood in a large community sample of German children.
Subjects and Methods
Data source and study population
The German Health Interview and Examination Survey for Children and Adolescents (KiGGS) was conducted by the Robert Koch Institute (Berlin, Germany) between May 2003 and May 2006. The design, sampling strategy, and study protocol have been described in detail elsewhere. 25 In brief, study subjects were enrolled by a two-stage sampling procedure. In the first stage, a sample of 167 municipalities was drawn that were representative of municipality sizes and structures in Germany. Stratified by sex and age, random samples of children and adolescents between the ages of 0 and 17 years were then drawn from local population registries in proportion to the age and sex structure of Germany's child population. The final sample included 17,641 children and adolescents (8,985 boys, 8,656 girls); the response rate was 66.6%. 25 Considering that young babies under 2 years may still be breastfed, we excluded these children (n=2,805), resulting in 14,836 children 3–17 years old left in the present study (Table 1).
Percentages and mean±SE values presented here were weighted according to the German national child population.
The sum in each category may not be equal to the total because of missing data.
The p values were calculated by Rao–Scott χ2 tests for categorical variables or analysis of variance for continuous variables.
Children who (1) had immigrated themselves or (2) had at least one parent who was not born in Germany or was of non-German nationality.
Defined as having any of the following conditions: (1) difficulty breathing or an adaptation problem; (2) infection; (3) neonatal jaundice; (4) low birth weight (<2,500 g), premature (<34 gestational weeks); or (5) other problems leading to hospital observation.
Data collection and definition of variables
As described elsewhere in detail, 25 standard, age-specific (3–6, 7–10, 11–13, and 14–17 years) questionnaires completed by parents (over 80% of questionnaires were completed by children's mothers), and a parallel questionnaire completed by adolescents (11–13 and 14–17 years), were used to collect data on sociodemographic characteristics, family economic background, and children's health-related behaviors. All data presented in this study were derived from parental questionnaires unless specified otherwise.
Children's general health status was rated by children's parents for the question “How do you rate the health status of your child at large?” with answer choices of “excellent/very good,” “good,” “fair,” “bad,” and “very bad.” 26 Data on breastfeeding were collected based on two questions. First, we asked, “Had your child ever been breastfed?”; if this was answered with “Yes,” then we asked, “How long had your child been breastfed exclusively, that means no extra bottle feeding or complementary feeding?” Answer choices for this question were “never breastfed exclusively,” “breastfed exclusively up to XX months” (number of months should be given), or “do not know.” 27 Information on maternal smoking and alcohol consumption during pregnancy was collected by the question “Did the mother of the child smoke (or drink alcohol) during the pregnancy?”; the answer choices were “yes, regularly,” “yes, occasionally,” and “never.” 28 Primary analyses found that only a very small portion of children had “very bad” (0.07%) or “bad” (0.25%) health status, and only 0.14% of children's mothers drank alcohol “regularly” during pregnancy, so we merged them into their respective nearest categories.
We included several control variables of prior and current exposures in the analysis that are likely to be associated with children's general health outcome. A medical problem in the first 4 weeks after birth was defined as having any of the following conditions as reported by the parents: (1) difficulty breathing or an adaptation problem; (2) infection; (3) neonatal jaundice; (4) low birth weight (<2,500 g), premature (<34 gestational weeks); and (5) other problems leading to hospital observation. 28 Children's body weight and height at birth were obtained from the mothers'/children's healthcare booklets. 28 Parental socioeconomic status was defined as lower, intermediate, or upper according to the total scores of a composite social status index integrating the parents' levels of education, household incomes, and professions. 29 Children were referred to as immigrants if they had immigrated themselves, they had at least one parent who was not born in Germany or was of non-German nationality, or both parents had immigrated or were of non-German nationality. 30 Children's current body mass index was computed from children's body weight and height measured by health professionals during the medical interview. Relative body weight was classified as normal weight, overweight, or underweight according to the criteria of Kromeyer-Hauschild et al. 31 Information on physical activity was collected among all children 3–17 years, which was provided by parents of 3–10-year-old children in the parental questionnaires and by 11–17-year-old adolescents in the child questionnaires. 32 Exposure to passive smoking at home was defined by the question “Is there any smoking at home in the presence of your child?”; the frequency of this was categorized as “daily,” “sometimes,” or “never.”
Statistical analysis
A weighting factor was used to adjust for deviations of demographic characteristics between the survey population and official population statistics (as of December 31, 2004). 33 Descriptive statistics were used to examine characteristics of the study population and children's health status. Group differences were tested by using Rao–Scott χ2 tests for categorical variables and using analysis of variance for continuous variables. We compared children's general health status among children overall and in each specific age group (3–6, 7–10, and 11–17 years, which roughly corresponds to preschool children, primary-school children, and middle-school children in Germany, respectively) stratified by breastfeeding and maternal smoking during pregnancy. As children's general health status showed a highly skewed distribution, we therefore dichotomized health status categories and fitted logistic regression models with an “excellent” versus “non-excellent” health status as the dependent variable. In order to determine the independent effects of breastfeeding and maternal smoking during pregnancy from other factors on children's general health status, we fitted four models for each age group. First we entered breastfeeding or maternal smoking during pregnancy in Model 0 to obtain crude odds ratios (ORs) and 95% confidence intervals (95% CIs); then we added other variables of prior and current exposures, including demographics, first separately and then in combination, to Models 1–3 to obtain respective adjusted ORs. In total, 1,683 (12.6%) of study participants had missing observations in some variables, with a range of 0.4% for immigrant background, 1.4% for children's health status, and 4.6% for breastfeeding. Missing values were excluded in multivariable regression modeling given the large sample size. All statistical analyses were performed using SPSS (Chicago, IL) statistical software (release 18.0). The SPSS complex samples procedure was applied throughout analyses to account for the clustered sample design and keep statistical inferences as conservative as possible. A p value of<0.05 was considered as statistically significant.
Results
Characteristics of the study population
The main characteristics of the study population are described in Table 1. Overall, about 23% of subjects had never been breastfed or had been breastfed exclusively over 6 months, while 8% were fed with breastmilk combined with formula milk concurrently. About 18% of children's mothers had smoked regularly or occasionally, and 14% had drunk alcohol occasionally during pregnancy.
Children's general health status by sociodemographics, prior breastfeeding, and exposure to pre- and postnatal health-related characteristics
According to parents' perceptions, only 7.2% of children had “fair” health status, while the vast majority of children had “good” (56.2%) or “excellent” (36.6%) health status. Except for the variable “region of residence” and sex (p=0.071), all other variables were found to be statistically significant in the bivariate analyses (Table 1). For example, significantly fewer adolescents in the age group 11–17 years had “excellent” health status than younger children in the age groups 7–10 and 3–6 years (32.5% vs. 40.3% vs. 41.3%, respectively; p<0.001).
Breastfeeding and age-specific children's general health
Children who had been breastfed exclusively over 6 months had significantly better health status later in life than children who had other feeding patterns. A significant difference for duration of breastfeeding was consistently found among children overall and in the age groups 3–6, 7–10, and 11–17 years (Fig. 1). Stratified by sex, the same was true for both boys and for girls of all age groups except for 3–6-year-old boys (p=0.145) (data not shown).
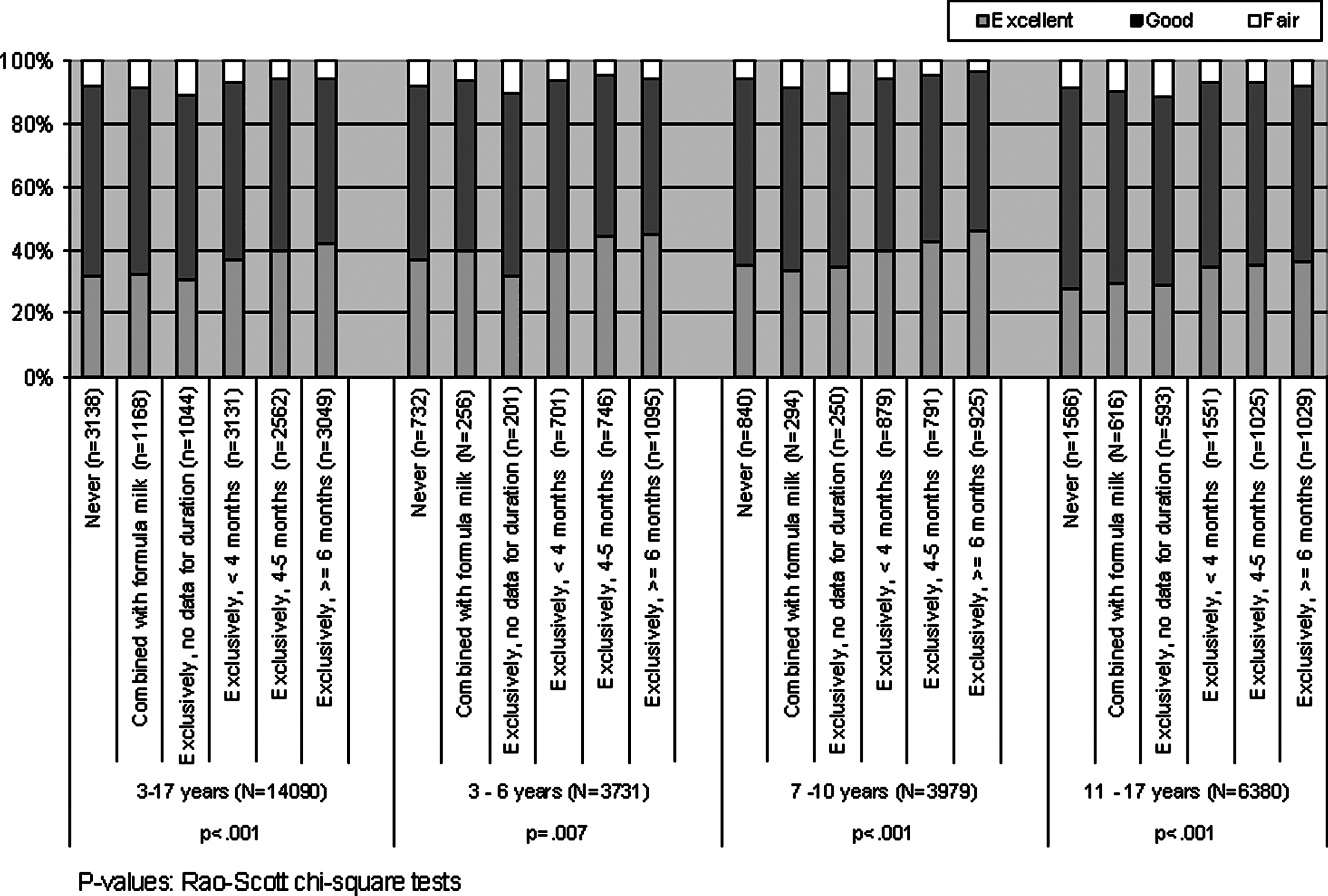
Breastfeeding pattern and age-specific children's general health status in the German Health Interview and Examination Survey for Children and Adolescents, 2003–2006. The p values were calculated by Rao–Scott χ2 tests.
Table 2 lists crude and adjusted ORs and 95% CI of children having perceived “excellent” health status in relation to breastfeeding. Children who had been breastfed over 6 months were more likely to have “excellent” health status in all age groups. ORs in each age group changed little after adjusting for prior exposure variables (Model 1) but changed considerably after adjusting for demographics and current exposure variables (Model 2). After adjusting for all confounding factors (Model 3), ORs remained significant in the regression models for children overall 3–17 years old and in the age groups 7–10 and 11–17 years (Table 2).
Odds ratios (ORs) and 95% confidence intervals (95% CIs) were derived from the logistic regression models with an “excellent” versus “non-excellent” perceived health status as the dependent variable. Model 0 included breastfeeding only, Model 1 included Model 0+prior exposures including medical problem after birth, maternal smoking and alcohol drinking during pregnancy, and body weight and height at birth, Model 2 included Model 0+demographics and current exposures including sex, age, urbanization, migration background, parental social status, body mass index, sports activities, and exposure to passive smoking at home, and Model 3 included Model 1+Model 2. Entries given in bold indicate a significant difference.
Maternal smoking during pregnancy and age-specific children's general health
Children whose mother never smoked during pregnancy had better health status than children whose mother smoked regularly or occasionally among children overall and in the age groups 3–6 and 11–17 years (Fig. 2). Stratified by sex, a significant difference was found for girls of the age groups 3–6 (p=0.006), 7–10 (p=0.052), and 11–17 (p=0.003) years but only in boys of the age group 3–6 years (p=0.047) (data not shown).
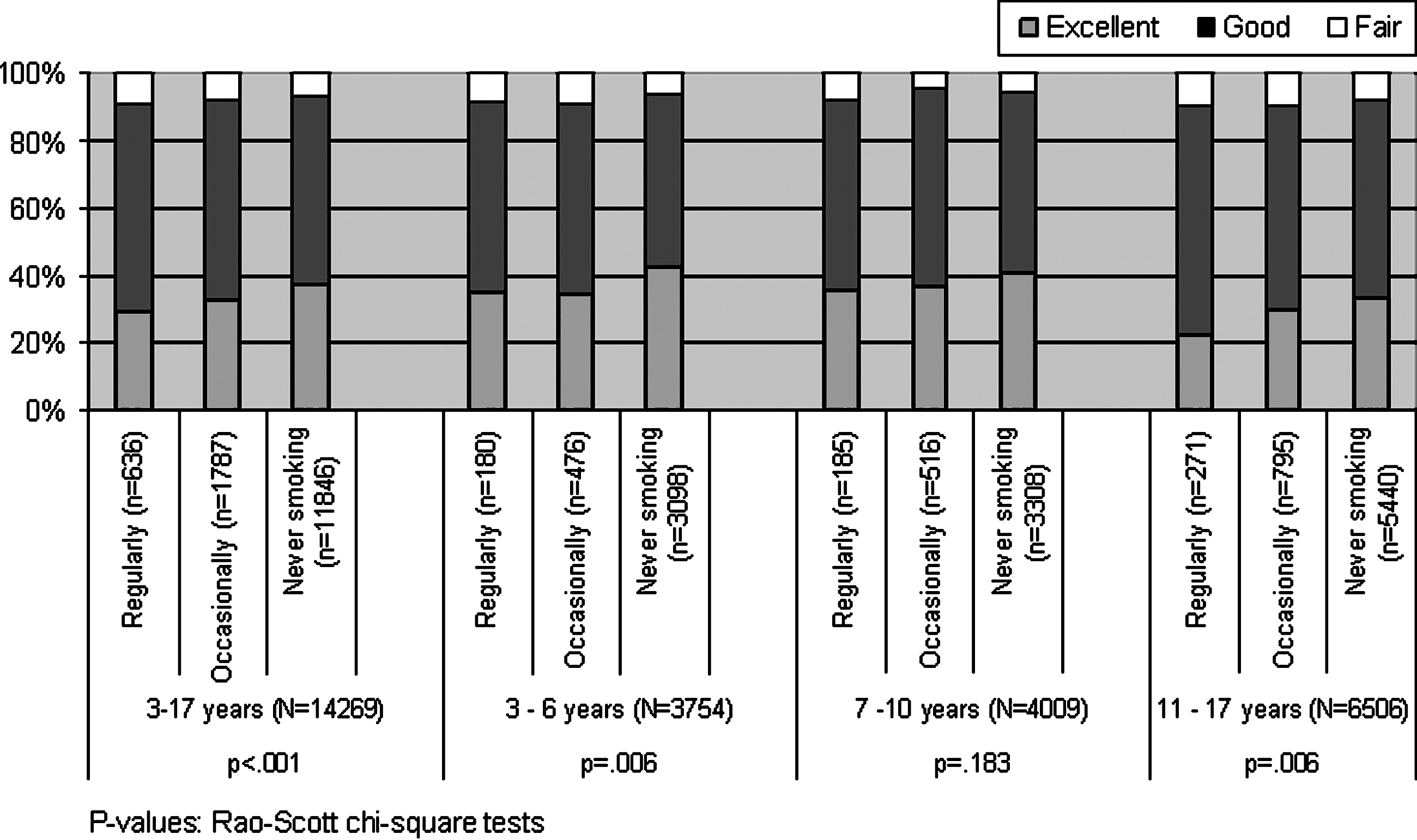
Maternal smoking during pregnancy and age-specific children's general health status in the German Health Interview and Examination Survey for Children and Adolescents, 2003–2006. The p values were calculated by Rao–Scott χ2 tests.
Children who had not been exposed to maternal smoking during pregnancy were more likely to have “excellent” health status later in life overall for children 3–17 years old and in the age group 11–17 years (Table 3). After adjusting for all confounding factors (Model 3), ORs remained significant in the age group 11–17 years only (Table 3).
Odds ratios (OR) and 95% confidence intervals (95% CIs) were derived from the logistic regression models with an “excellent” versus “non-excellent” perceived health status as the dependent variable. Model 0 included maternal smoking during pregnancy only, Model 1 included Model 0+prior exposures including medical problem after birth, breastfeeding, maternal alcohol drinking during pregnancy, and body weight and height at birth, Model 2 included Model 0+demographics and current exposures including sex, age, urbanization, migration background, parental social status, body mass index, sports activities and exposure to passive smoking at home, and Model 3 included Model 1+Model 2. Entries given in bold indicate a significant difference.
In addition, children whose mother had never drank alcohol during pregnancy were more likely to have “excellent” health status in the age group 3–6 years only (Model 3, adjusted OR 1.27, 95% CI 1.01–1.59) but not in other older age groups 7–10 and 11–17 years (data not shown). Separate analyses found no interactions between breastfeeding and maternal smoking during pregnancy, either overall or in age-specific subgroups (data not shown).
For adolescents 11–17 years old, we also collected data on pubertal stage (self-assessed Tanner stage of pubic hair growth), cigarette smoking, and alcohol drinking in the children's questionnaires. With including these variables in the regression models, breastfeeding and maternal smoking during pregnancy remained statistically significant (data not shown).
Discussion
In a national community sample of children and adolescents in Germany, we found that exclusive breastfeeding over 6 months and non-exposure to maternal smoking during pregnancy were associated with better general health status when children reach adolescence.
Comparison with other studies
General health status is a comprehensive concept, reflecting the current situation of illness and well-being. In the long-term child growth period from one developmental stage to another, health status is influenced directly or indirectly by a wide spectrum of biological, environmental, and family socioeconomic factors as well as personal health behaviors, including sports activities, balanced nutrition, etc.18–22,34,35 In an effort to address this, we included a variety of well-known influential factors on health, including other prior and current exposures, in the logistic regression models. Nonetheless, even after accounting for those controllable factors, the association of prior breastfeeding and non-exposure to maternal smoking during pregnancy with “excellent” health status later for children 11–17 years old remained robust. This is most likely not a chance finding, but can be explained from two aspects.
First, our findings have a biological basis. Human breastmilk is the best source of nutrition for infants because of its many health-protective factors, such as antibodies derived from lactating mothers.3,36 Smoke contains thousands of toxic compounds such as nicotine and carbon monoxides. Breastfeeding is therefore believed to lower infants' risk of various infections in the early postpartum period,4,37 whereas exposure to maternal smoking during pregnancy is believed to increase the risk of low birth weight38,39 and abnormal development in infants.5,7 Such early events may likely play a critical role in the development of both later childhood and adult diseases. Second, the benefits of breastfeeding and adverse outcomes of exposure to maternal smoking during pregnancy have been well documented in previous studies. Breastfeeding has been found to reduce the risk of some chronic diseases in children later in life. Results of meta-analyses showed that breastfeeding has a protective effect against asthma, 40 atopic dermatitis, 41 obesity, 42 type 2 diabetes, 43 cancers, 44 high blood pressure later in life, 45 and protection against hospitalization for diarrhea and respiratory tract infection. 46 Furthermore, a shorter duration of breastfeeding may be a predictor of adverse mental health outcomes throughout the developmental trajectory of childhood and early adolescence. 47 Results of these studies suggest strongly that breastfeeding may have a long-term effect on health.14–16 In contrast, maternal smoking during pregnancy increased the risks of middle ear disease, 48 overweight, 49 type 2 diabetes during childhood, 50 and reduced children's motor competence, 51 also suggesting a long-term effect.5,6,17 Although in our study we checked health status in general, it logically follows that children with reduced risks of these diseases may have overall better health status.
However, even if breastfeeding and maternal smoking during pregnancy may influence health status, their effects were expected to be moderate. This may be one of the reasons why our results tend to show a borderline significance and to be detected in age groups with a large sample size. Family socioeconomic status, socioenvironmental factors, and parental and individual health behavior, including sports activities,20–22,34,35 play a more critical role in children's health status later in life. The strength of the associations of two exposure variables with health status was attenuated after these important confounders were added into the models. This can be seen as the crude ORs considerably changed after adjustment for various confounders of current exposures (Tables 2 and 3). As shown in our multivariable regression models, family social status and sports activities mostly contributed to the age-specific multivariable regression models (data not shown). The associations are most apparent in the age group of 11–17 years; however, results in the younger age groups are generally in the same direction. Reasons for this may be that among younger children there is a less pronounced difference in subjective health than among older ones. For adolescents 11–17 years old, puberty is an important developmental stage. Individual health behavior such as cigarette smoking and alcohol drinking has a substantial influence on health, too, which may likely contribute to the overall poorer health status in adolescents compared with younger children. Yet, separate reanalyses including these variables in the models found no significant changes compared with the results reported, suggesting the effects of breastfeeding and maternal smoking were rather robust.
In our study sample, only a small portion of mothers drank alcohol occasionally during pregnancy, and their children showed better health status than children whose mothers did not in the bivariate analysis (Table 1). This association, however, was not found in the multivariable analyses, suggesting occasional exposure to alcohol during pregnancy may have little influence on children's general health later in life. Nevertheless, we still oppose drinking alcohol by women during pregnancy given its reported other well-known adverse effects. 52 In fact, non-exposure to maternal alcohol drinking was found to be associated with “excellent” health status in the age group 3–6 years after adjusting for other factors.
Implications on public health
Our results are favorable toward breastfeeding and unfavorable toward smoking and are of great public health importance, given the low rate of breastfeeding and the substantial proportion of women smoking during pregnancy. We assessed the general health status of all children, instead of specific conditions; results are relevant to all children. Because children's overall health, in adolescence in particular, is key to the development into adulthood and a significant concern of mothers, (expectant) mothers may take appropriate action with regard to these two modifiable health behaviors.
Strength and limitations
KiGGS is a well-organized national health survey investigating a large nationally representative community sample of children and adolescents. 25 We used the SPSS complex sample methods to estimate ORs and 95% CIs, and the weighted results could be generalized to the entire child population in Germany. However, there are some limitations to our study. First, breastfeeding behavior occurred years prior to the survey; although studies show that maternal recall for breastfeeding initiation and duration is valid and reliable, 53 we do not exclude the possibility of recall bias. In particular, recall bias could likely be larger for the age group 11–17 years than in the younger age groups. However, as some women may overestimate while some women may underestimate their breastfeeding duration, this would rather be a nondifferential misclassification, which would bias the results toward an underestimation of any true relationships. In addition, we used the categorical variable for breastfeeding; this would allow for some degree of recall error and would not influence the results substantially. For example, suppose a woman had a true breastfeeding duration of 7 months, no matter whether she reported the breastfeeding duration of 6.5 months, 10 months, or even 15 months because of recall error, she belonged to the group “breastfeeding ≥6 months.” Differences in breastfeeding practices may be less pronounced compared with 10 years ago as a result of education campaigns in recent years. In response to this concern, we checked the proportion of breastfeeding over 6 months among different age groups and found that it declined significantly along with age (31.7%, 24.7%, and 16.7% for age groups 3–6, 7–10, and 11–17 years, respectively [data not shown in Results]). As our results suggested that breastfeeding over 6 months may promote children's health, supposing that children 11–17 years old had the same higher proportions as children in younger age groups, their health status would be even better. As regard to maternal smoking during pregnancy, no significant difference was found among different age groups. Second, although we used the word “exclusively” in the questionnaire, the wording was somewhat modified and could largely be treated as “full breastfeeding.” 27 Based on the strict World Health Organization definition for exclusive breastfeeding, we do not exclude possibility of misclassification bias. Yet, given the large sample size, small misclassification bias, either due to a different definition for exclusive breastfeeding or due to recall errors, should have no substantial influence on our final findings. Third, subject to the cross-sectional study design, the links established in our study between prior breastfeeding and exposure to maternal smoking during pregnancy with children's health status later in life do not necessarily mean causality. Fourth, although we cover as many influence factors as possible in the regression models, other factors such as nutrition and maternal passive smoking during pregnancy that may have a substantial influence on children's health were not considered, potentially resulting in some degree of residual confounding. Nutrition habits, however, may change with time. We believe the influence of nutrition as well as parental health awareness or health behaviors may have been well captured by family socioeconomic status, 54 while maternal exposure to second-hand smoke during pregnancy may have been captured by the exposure to passive smoking at home. Finally, we cannot rule out that the two investigated exposures may merely be surrogate parameters for some other factors like parental health awareness or health behaviors considering that adjusted ORs changed considerably in the regression models.
Conclusions
In spite of the limitations of our study, our findings suggest that exclusive breastfeeding for >6 months may have a positive influence, whereas maternal smoking during pregnancy may have a negative influence, on children's health status later in life. This is particularly true when children reach adolescence. Further studies are required to elucidate these possible and biologically plausible associations. Like results of most other studies investigating associations of prior exposures in childhood with health outcomes later in life,55,56 our results should be interpreted with caution given the limitations of this study such as cross-sectional design and possible influences of recall bias. Nevertheless, breastfeeding and smoking are two modifiable health behaviors, and given the well-known benefits of breastfeeding and risks of smoking to which our study adds new evidence, health professionals should take all opportunities to promote exclusive breastfeeding over 6 months among new mothers and the cessation of smoking in expectant mothers for a healthier future of their children.
Footnotes
Acknowledgments
The German Health Interview and Examination Survey for Children and Adolescents (KiGGS) was funded by the German Federal Ministry of Health and the Ministry of Education and Research. We would like to thank Ms. Kim Truong from Stanford University very much for her language editing of this manuscript.
Disclosure Statement
No competing financial interests exist.