
Abstract
Abstract
Background:
The Baby-Friendly Hospital Initiative aims at protecting, promoting, and supporting breastfeeding. Cesarean section is known to represent an obstacle to breastfeeding. In this observational study we compared Baby-Friendly and non–Baby-Friendly hospitals (BFHs and non-BFHs, respectively) in terms of cesarean section rate.
Materials and Methods:
Italian BFHs were compared with non-BFHs located in the same regions. Data used for analysis were type of hospital, annual deliveries, annual cesarean section deliveries, region of location, and BFH status. The primary outcome was a cesarean section rate below a threshold specific for the identified regions; because of skewed distribution, the median rate was chosen. Descriptive and comparative univariate and multivariate analyses were carried out.
Results:
In 2009, in Italy, there were 20 BFHs located in eight regions. Compared with the 207 non-BFHs with more than 200 annual deliveries located in the same regions, BFHs had a cesarean section rate below the median of the eight regions (30.4%; interquartile range 14.6%), even after adjustment for confounders (adjusted odds ratio, 12.71; 95% confidence interval, 1.84, 87.72). In addition, being a public hospital, performing a higher number of deliveries, and being located in specific regions also predicted a cesarean section rate below the median. Overall, the regions with at least one BFH showed a lower cesarean section rate, compared with regions without BFHs.
Discussion:
In Italy there are few BFHs, but regions with at least one BFH show a cesarean section rate below the national median. Several factors impact on the cesarean section rate, causing huge variation among regions. Nevertheless, within the same region, BFHs have a lower cesarean section rate compared with non-BFHs.
Introduction
However, when the BFHI was launched, the attainment of an adequate rate of cesarean section was not listed among the hospital policies to be promoted, which were mainly focused on neonatal care. In 2009 the BFHI package was revised and updated, and a more holistic approach, addressing “Mother-Friendly Care,” was adopted. 10 Novelties introduced include (1) support to mothers who are not breastfeeding, (2) human immunodeficiency virus and infant feeding, and (3) more guidance for monitoring and reassessment. Containment of invasive procedures such as rupture of the membranes, episiotomies, acceleration or induction of labor, instrumental delivery, and cesarean section was also introduced among the activities to be pursued. The rate of cesarean section was listed among the indicators to be measured in Baby-Friendly hospitals (BFHs), but a defined threshold has not been established; countries define it according to local condition and priorities. The Ministry of Health of Brazil, for example, since 2004, has added 10 more criteria to the Ten Steps for the Baby-Friendly designation; a cesarean section rate below a threshold identified for each federal administrative area is one of these.11,12
Italy is the country with the highest cesarean section rate (38.4% in 2009) 13 in the industrialized world, 14 with impressive differences among regions (regional means range from 23.7% to 62.0%) and a north–south gradient, with southern regions presenting higher rates of cesarean section. 13 Several factors, often interlinked and not always clearly understood, contribute to this situation: the cesarean section rate is higher in private hospitals (58.3%) than in public ones (35.0%), 15 private health care is more widespread in southern than in northern regions (private beds for acute care are 21% of the total in the south and 12% in the north), 16 and the physician/nurse ratio for a given population follows the same gradient (0.48 in the south, 0.35 in the north). 16 In addition, maternity wards attending less than 500 deliveries per year are more often located in southern region, whereas those attending more than 1,000 deliveries per year are more frequent in the north. 15 Sociocultural differences are also relevant: employment of women is lower in the south than in the north (32.1% vs. 57.5% in women 15–64 years old), 17 whereas early school leaving (i.e., population 18–24 years old with at most lower secondary education and not in education or training) is more frequent in the south than in the north (31.4% vs. 15.8%, respectively). 18
The objective of this study is to assess the association, if any, between Baby-Friendly designation and cesarean section rate in Italian hospitals.
Materials and Methods
The study was conducted at the end of 2010. Context data were gathered from the national database of hospital admissions (Italian acronym SDO), a register based on central collection, analysis, and reporting of quarterly data provided by each region. All Italian BFHs were identified, and their main characteristics were compared with those of non-BFHs located in the same regions. Original data collected for BFHs and non-BFHs were as follows: annual number of deliveries, annual number of cesarean section deliveries, administrative status of the hospital, BFH designation, and region of location (all data referred to 2009). Regional contact persons (listed in Acknowledgments), contacted by e-mail, provided these information for all hospitals within their region. Hospitals were categorized based on annual deliveries (less than 500, 500–999, 1,000–1,499, 1,500 and over) and on administrative status (public, private, university hospital).
A descriptive analysis of reported frequencies, with means, SDs, and median and interquartile range (IQR), was conducted. The outcome of interest of this comparative analysis was a cesarean section rate below a given threshold, chosen as proxy of better obstetric care. To determine the most appropriate threshold, the rates of the selected hospitals were plotted; because of important differences among regions, only data from regions with at least one BFH were included in this comparative analysis. As the distribution was skewed to the right, with several outliers showing extremely high rates (over 80%), the median was chosen as a more appropriate threshold (Fig. 1).
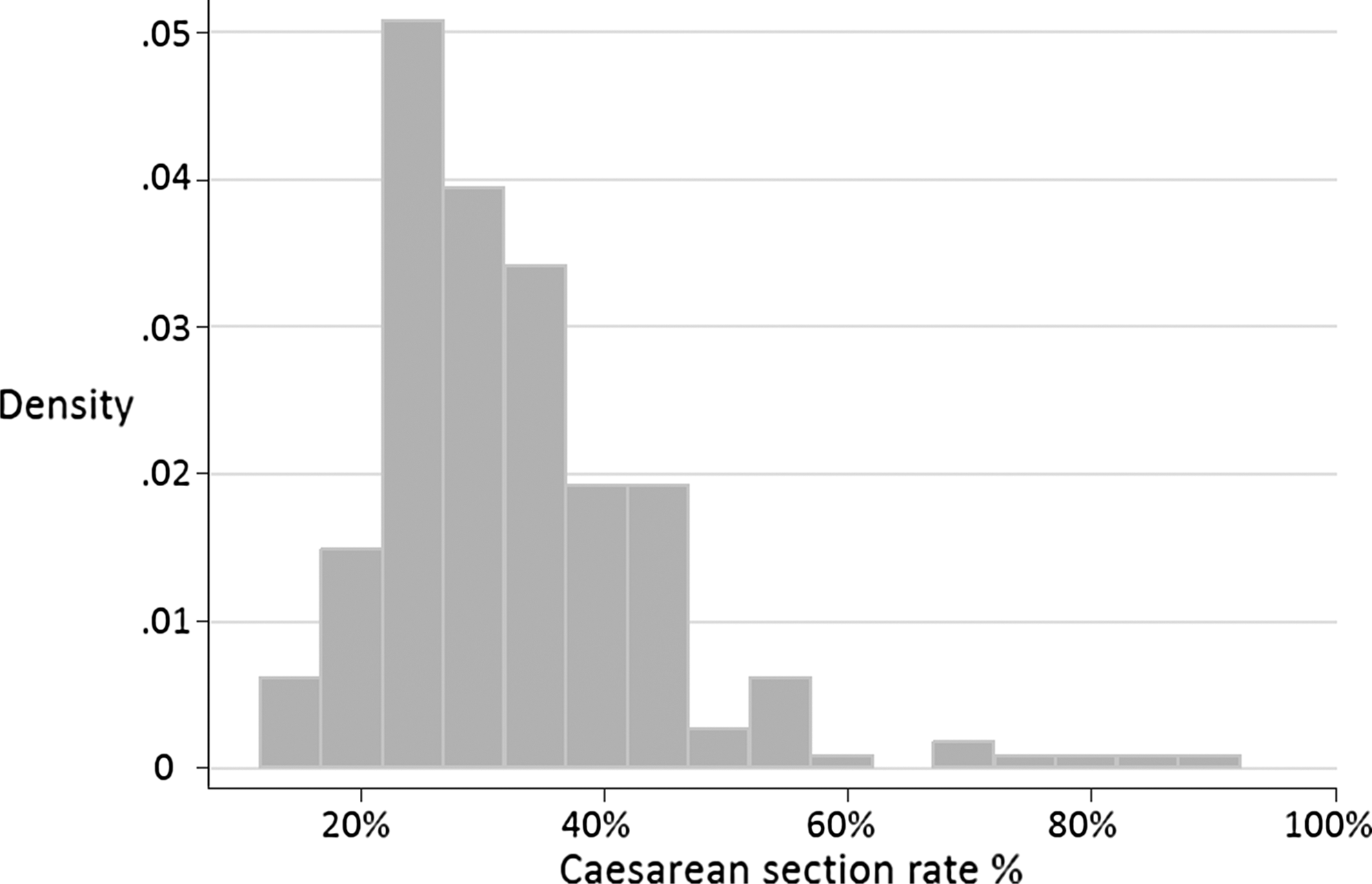
Distribution of the cesarean section rate in the overall sample of 245 maternity units in eight regions in Italy in 2009 having at least one Baby-Friendly Hospital. Source of data: regional key informants (given in Acknowledgments).
Point estimate (odds ratio [OR]) and 95% confidence intervals (95% CIs) of the association between the main exposure (being a BFH) and the outcome of interest (cesarean section rate below the median) were calculated using univariate analysis. The same analysis was conducted for all the other variables; Pearson's χ2 test or Pearson's χ2 test for trend was used as appropriate.
Because the sample included some hospitals with a small number of annual deliveries, a sensitivity analysis was carried out to estimate the effect of excluding these hospitals from the final model. Four scenarios were considered: excluding hospitals with less than 100 annual deliveries, less than 200, less than 300, and less than 350, with 368 being the annual deliveries of the smallest BFH. As the estimates were stable across the four scenarios, the model including the largest number of observations and the smallest number of outliers was chosen; only hospitals with more than 200 annual deliveries were included in the final model.
Multivariate analysis was then conducted by logistic regression including the variables associated with the outcome of interest (p<0.10) in the univariate analysis; the likelihood-ratio test and Pearson's χ2 test for goodness of fit were used. One BFH was excluded from the multivariate model as no other hospitals were present in the same region (Valle d'Aosta) for comparison. Valle d'Aosta is a peculiar region, as it is small and surrounded by mountains, with tiny villages located in the valleys. In this region there is only one hospital with a maternity ward. There are no comparable regions in Italy; for this reason data regarding this hospital were included only in the descriptive and univariate analysis.
Statistical analyses were carried out using STATA software version 11 (StataCorp LLC, College Station, TX).
Results
In 2009, according to the SDO database, there were 665 maternity wards in the 20 administrative regions of Italy. 13 The total number of deliveries was over 590,000, and the overall mean rate of cesarean section was 38.4%, with large differences among regions (from 23.7% in Friuli-Venezia Giulia to 62.0% in Campania) (Table 1).
Data are from 2009 from the SDO database. 13
Regions are listed based on geographical location, from north to south.
Region with at least one Baby-Friendly Hospital (BFH).
Only eight regions (Friuli-Venezia Giulia, Lazio, Lombardia, Marche, Toscana, Trentino-Alto Adige, Valle d'Aosta, and Veneto) had a BFH in 2009. According to data gathered for this research from regional key informants, those eight regions had 245 hospitals with a maternity ward: 18 of these 245 hospitals, all non-BFHs, reported fewer than 200 annual deliveries and thus were excluded from the analysis (four had less than 10, seven between 10 and 100, and seven between 100 and 200 deliveries in 2009). The characteristics of the remaining 227 hospitals, by region, are reported in Table 2 (note that the sources of data for Table 1 and Table 2 differ). The number of deliveries ranged from 206 to 6,521 (mean, 1,177; SD, 864), and the cesarean section rate was between 11.6% and 87.1% (mean, 32.6%; SD, 11.8%; median, 30.4%; IQR, 14.6%, with some outliers) in the included hospitals. The majority of the BFHs (18 of 20) were public, two were private, and none was a university hospital. Among the 207 non-BFHs, 153 (73.9%) were public, 32 (15.5%) were private, and 22 (10.6%) were university hospitals. The distribution of annual deliveries in BFHs and non-BFHs is reported in Table 3.
Data are from 2009 from regional key informants (given in Acknowledgments). Considering the different sources, data in Table 2 can differ slightly from data in Table 1.
As Valle d'Aosta has only one maternity ward, the absolute rate of cesarean section, mean, and median coincide.
BFH, Baby-Friendly Hospital; IQR, interquartile range; NA, not applicable.
Source of data is regional key informants (given in Acknowledgments).
BFH, Baby-Friendly Hospital.
Seventeen of 20 BFHs (85%) had a cesarean section rate below the median, whereas only 96 of 207 (46.4%) of non-BFHs had a cesarean section rate below it; the median cesarean section rate was 30.9% (IQR, 14.3%) and 24.9% (IQR, 5.9%) in non-BFHs and BFHs, respectively (Fig. 2). In the univariate analysis, being a BFH was significantly associated with a cesarean section rate below the median (OR, 6.55; 95% CI, 1.86, 23.04). Other independent variables associated with a cesarean section rate below the median were type of hospital (with public hospitals as the reference, for private hospitals, OR, 0.44 and 95% CI, 0.20, 0.94; for university hospitals, OR, 0.30 and 95% CI, 0.11, 0.80), region (p<0.001), and annual deliveries, with the OR significantly increasing with higher number of deliveries (test for trend significant, p=0.004) (Table 4). Multivariate analysis, aimed at correcting for case mix based on number of annual deliveries and type of hospitals, confirmed the association: hospitals with a cesarean section rate below the median were more often BFHs and public and had 1,000 or more annual deliveries. The model also contained the region where the hospital was located because this variable was significantly associated with the outcome of interest (Table 4).
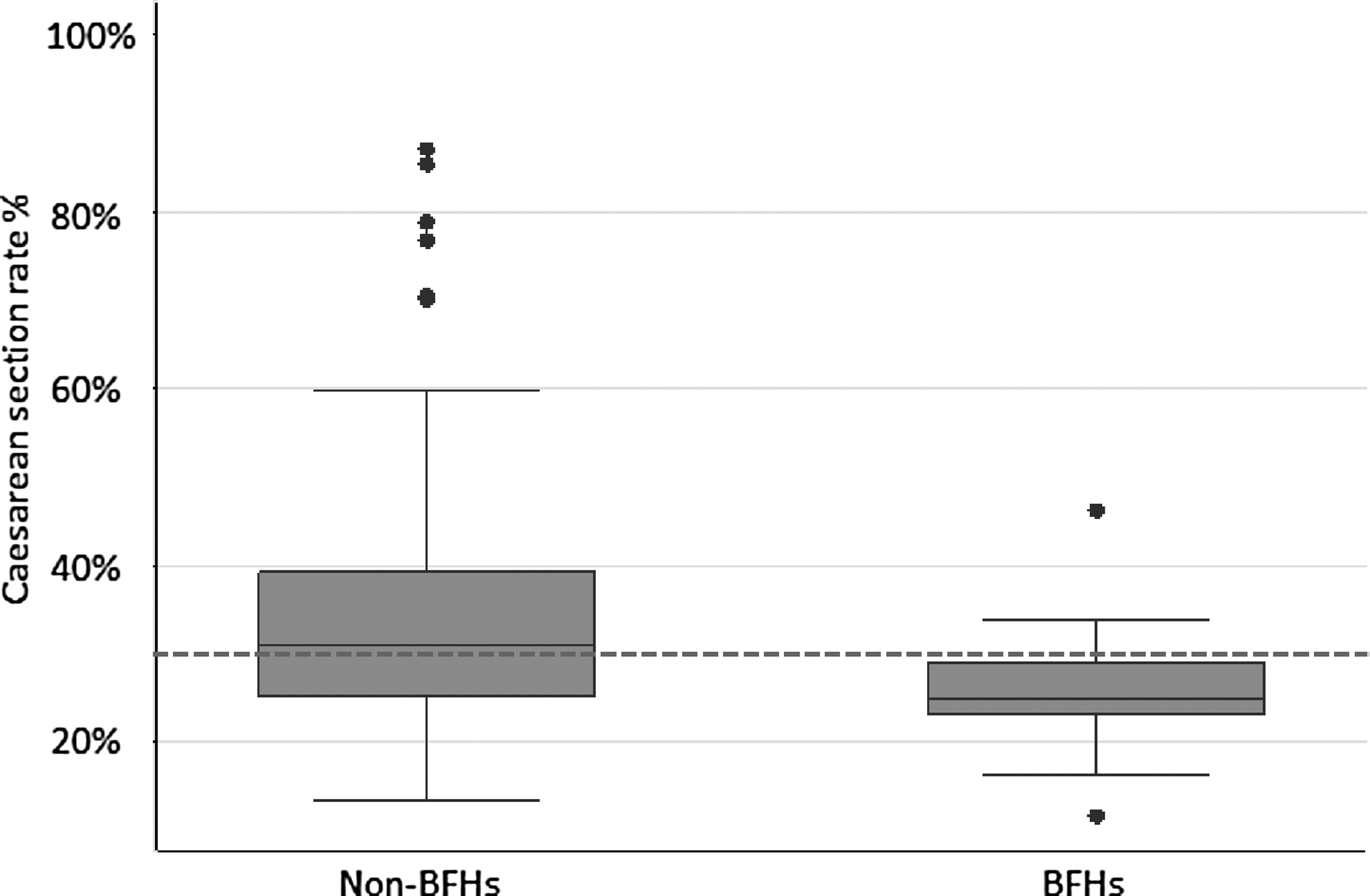
Distribution of the cesarean section rate by Baby-Friendly Hospital (BFH) status. Each box represents the interquartile ranges (25th, 75th percentiles) of the cesarean section rate in the considered group of hospitals, whereas the continuous line crossing the box represents the median (50th percentile), the ends of the whiskers represent the 5th and 95th percentiles, and the dots are the outliers (hospitals showing a cesarean section rate below the 5th or above the 95th percentile). The dotted horizontal line represents the median of the cesarean section rate in the whole sample (30.4%).
The model contains the independent categorical variable “region.” This variable is associated with the outcome of interest both in the univariate analysis and in the multivariate analysis (p<0.001). The model includes 226 observations as the record describing the only hospital in Valle d'Aosta region has been excluded in the multivariate analysis. By Pearson's χ2 goodness-of-fit test, p=0.4693.
BFH, Baby-Friendly Hospital; CI, confidence interval; OR, odds ratio.
Discussion and Conclusions
This study analyzed the association between being a BFH and having a cesarean section rate below a threshold defined as the median of the eight regions included in the analysis. Based on 2009 data, being a BFH is associated with a cesarean section rate below this threshold. The association is significant, although with wide confidence intervals because of the small number of BFHs. Moreover, having a higher annual number of deliveries, being a public hospital, and the region in which the hospital is located are also associated with the outcome of interest.
In 2009, the year of observation, the overall mean cesarean section in Italy (20 regions, each with its own administrative and organizational structure also with respect of health services and hospitals administration) was 38.4%. 13 The mean cesarean section rate was as high as 45% when considering only the 12 regions without BFHs. Among these, some southern regions had a higher proportion of deliveries occurring in private hospitals 15 : these regions showed a higher rate of cesarean section (Table 1). Recent analysis shows that the Italian federal organization of health services has generated a high variability in quality of hospital care among regions with respect to labor and delivery care: the regions having a larger number of hospitals attending less than 500 annual deliveries are the regions with the highest rate of cesarean section13,19 and having more private hospitals. These are also the regions without BFHs. The regions with BFHs show a better attitude to appropriate obstetric care as measured by cesarean section rate. As Italy shows an impressive variability among regions with respect to cesarean section rate, intraregional comparison are also needed: within the same region BFHs perform better than non-BFHs in term of cesarean section rate, even after correcting for confounders.
A limitation of our study is that only a small set of variables was included in the analysis; thus we cannot exclude the effect of other known or unknown confounding factors on the association described. As the cesarean section rate varies considerably among Italian regions, with a clear gradient north–south, in that the southern regions are the ones showing higher cesarean section rates, we can speculate that factors other than being a BFH influence the cesarean section rate: on average, health care in the south is more frequently private, 16 more costly, 16 and less efficient, 20 but the real determinants of this situation are still unclear and, in any case, difficult to disentangle and to tackle. Despite this limitation, and to the best of our knowledge, this is the first study assessing the association between BFH status and cesarean section rate. Our study suggests that, in Italy, BFHs have more appropriate obstetric care than non-BFHs, at least as measured by containment of the cesarean section rate. Needless to say, BFHs report also much higher rates of breastfeeding. However, as the implementation of activities needed to start a BFHI designation process is recent and still not widespread (the first BFH was designated in 2001, and at the beginning of 2010 only 20 of 598 Italian maternity wards 21 had a BFHI certification), our conclusions should be considered with caution. It is possible that the situation will change and that the overall rate of cesarean section in BFHs will go up as the number of BFHs increases. This risk is especially relevant if newly designed BFHs will only focus their attention toward the implementation of the Ten Steps for Successful Breastfeeding without promoting also “Mother-Friendly Care.” A clear policy of including a low cesarean section rate, based on national or regional criteria, in conjunction with other appropriate obstetric interventions, should be a prerequisite to become a BFH, similarly to what has happened in Brazil since 2004,11,12 thus enhancing the virtuous process of combining “Baby-” and “Mother-Friendly Care.”
Footnotes
Acknowledgments
We are grateful to the following individuals for providing data about the hospitals within their region: Luisella Giglio, Direzione Centrale Salute Integrazione Sociosanitaria e Politiche Sociali, Friuli-Venezia Giulia; Domenico Di Lallo, Agenzia di Sanità Pubblica, Lazio; Carlo Zocchetti, Governo dei Servizi Sanitari Territoriali e Politiche di Appropriatezza e Controllo, Lombardia; Patrizia Carletti, Agenzia Regionale Sanitaria, Marche; Monica Da Frè, Osservatorio di Epidemiologia dei Servizi Sociali Integrati Agenzia Regionale di Sanità, Toscana; Fabrizia Tenaglia, Unità di Ostetricia e Ginecologia Ospedale S. Chiara Trento, Trentino-Alto Adige; Lucia Pellissier, Unità di Ostetricia e Ginecologia Ospedale Beauregard, Valle d'Aosta; and Costantino Gallo, Unità Ricerca e Innovazione Agenzia Regionale Socio Sanitaria, Veneto.
Disclosure Statement
No competing financial interests exist.