
Abstract

The attendees for the meeting were similarly diverse. A mixture of clinicians, researchers, and students, including basic scientists, neonatologists, pediatricians, midwives, nurses, lactation consultants, and dietitians, attended the main conference and the modular sessions on the pre-conference day, September 27.
The Conference program featured nine primary scientific topics that ranged from infant nutrition, premature infants, the gut microbiome, the milk microbiome, milk production, and other important human milk and lactation topics. There were 40 invited speakers, 130 submitted abstracts, and 14 abstracts selected for podium presentations. The invited and submitted abstracts are posted online (www.isrhml.org/meetings-conferences/).
A feature of each ISRHML meeting is the awarding of the prestigious Macy-Gyorgy award, given to a researcher whose lifetime research and scholarship has had a major impact in the field. The 2012 Awardee was Dr. Katherine Dewey, who presented the lecture “Research on human lactation and infant nutrition: The value of challenging conventional wisdom.” Another prestigious recognition, the Erlich-Koldovsky Award for an emerging human milk scholar, was received by Dr. Lars Bode. Travel awards were received by Olivia Ballard, Georgia Billing, Sarah Comstock, Eric Nonnecke, Mara Riley, Julie Ross, Li Tang, and Catrin Wurtz.
The superb scientific program was augmented by productive networking and sharing among participants, as well as the beautiful Adriatic Sea location, nice weather, and a plethora of social and sightseeing activities. Evaluations from the conference were overwhelmingly positive.
1. Manipulation of the Intestinal Microbiome in the Newborn Infant
References
2. Health Outcomes of Human Milk for Premature Infants
Human milk (HM) feedings from the infant's own mother (e.g., excluding donor milk) have been associated with a reduction in the risk of developing severe and potentially handicapping morbidities during and after the neonatal intensive care unit (NICU) hospitalization in premature infants. 1 These morbidities, which include late-onset sepsis (LOS), necrotizing enterocolitis (NEC), chronic lung disease (CLD), and retinopathy of prematurity (ROP), are costly to treat in the NICU 2 and increase the risk for long-term health problems in affected infants. 3 Increasingly, this body of evidence suggests a dose–response relationship between the amount of HM received by the infant and the magnitude of risk reduction. 1 Other lines of evidence suggest that there may be critical exposure periods during which the premature infant is especially susceptible to the pro-inflammatory effects of bovine-based formulas, which potentially trigger inflammation-based morbidities such as NEC.4–7 Thus, the protective effect of HM feedings in previous research may result from infants having received a threshold dose (mL/kg/day) or having avoided formulas (100% HM feedings) during critical exposure periods. It is important to understand the specific relationship between dose and exposure period of HM feedings and health outcomes during and after the NICU hospitalization in premature infants because this information has important research, clinical, and health policy implications.
This presentation will report dose and exposure period of HM feedings and health outcomes for an ongoing prospective cohort of very low birth weight (VLBW) (<1,500 g) infants enrolled in a National Institutes of Health-funded study from 2008 to 2012. Exclusion criteria were as follows: birth weight >1,500 g, birth gestational age >35 weeks, initiation of enteral feedings after day of life 14, major congenital anomalies or chromosomal disorders, and maternal conditions that would preclude HM provision or use for infant (e.g., maternal cocaine use). For multiple births, one infant from the multiple set was randomly selected for inclusion in the study. Although preliminary findings reveal that 98% of enrolled infants received some HM, the maternal decision to provide HM was not an inclusion criterion. Slightly over 95% of eligible VLBW infants have been enrolled in the study, and the cohort is diverse with respect to the inclusion of infants born to African American (40% of cohort) and low-income (Supplemental Security Income, Women Infant and Children eligible, 60% of cohort) mothers.
Prospectively collected data included infant daily weight, occurrence of morbidities (NEC, CLD, ROP, and LOS, using standardized medical definitions), maternal and neonatal clinical factors, daily intake (mL) of HM and formula, and timing of HM fortifier supplementation. Dose of HM feedings was calculated in two ways in order to examine whether the impact of HM on a specific morbidity was associated with infants having received a critical threshold amount (e.g., mL/kg/day) of HM and/or the avoidance of bovine-based formula (percentage of total enteral feedings as HM). Exposure periods for which the dose of HM was examined were postnatal Days 1–14, 15–30, 31–45, 46–60, and >60 and the entire NICU hospitalization.
The presentation of results will include the relationship between dose and exposure periods of HM feedings during the NICU hospitalization and the risk of select morbidities and infant growth. These findings will be discussed within the context of previous research in this area with recommendations for further research, clinical practice, and health policy priorities.
References
3. The Economic Burden of Necrotizing Enterocolitis
References
4. The Role of Oligosaccharides in the Protection from NEC: Data from an Original Study
Necrotizing enterocolitis (NEC) is one of the most frequent and fatal intestinal disorders in preterm infants. Between 5% and 10% of very low birth weight infants (<1,500 g birth weight) develop NEC. More than 25% of them die from the disorder, and the survivors are often faced with long-term neurological complications. NEC etiology and pathogenesis remain poorly understood, and biomarkers to identify at-risk infants do not exist. Breastfed infants are at six- to 10-fold lower risk for NEC than formula-fed infants, but the protective components in human milk have not been identified. One of the major differences between formula and human milk lies in the quantity and complexity of oligosaccharides. One liter of mature human milk contains between 5 and 15 g of unconjugated complex glycans, called human milk oligosaccharides (HMOs). In contrast, the oligosaccharide concentration in formula is several orders of magnitude lower, and the structures are less complex. HMOs are prebiotics and antimicrobials that alter the infant's intestinal microbiota composition. In addition, in vitro studies suggest that HMOs may modulate the infant's immune system and reduce mucosal neutrophil infiltration and activation. Since bacterial colonization and excessive mucosal neutrophil activity are key features in NEC pathogenesis, we hypothesized that HMOs contribute to the lower NEC risk in breastfed infants. Studies to test this hypothesis in human infants are currently not feasible owing to the limited availability of isolated and purified HMOs. Instead, we took an alternative approach, isolated several grams of HMOs from pooled human milk, and determined whether they reduce NEC in an established model of the disorder in neonatal rats.
Our studies confirmed that formula without HMOs reduces survival rates and causes NEC in neonatal rats. Adding pooled HMOs to the very same formula significantly improved survival and reduced NEC risk. Compared with formula alone, pooled HMOs significantly improved 96-hour survival from 73.1% to 95.0% and reduced pathology scores from 1.98±1.11 to 0.44±0.30 (—p<0.001). Galactooligosaccharides, which are currently added to commercial infant formula to mimic the prebiotic effects of HMOs but are structurally very different from the naturally occurring HMOs, had no effect, suggesting that the beneficial effects of HMOs are structure-specific and independent of their prebiotic properties.
Subsequently, we used two-dimensional chromatography to answer the question of which of the more than 100 different HMOs were responsible for the observed beneficial effects. In the first dimension, we used anion exchange chromatography to separate the pooled HMOs by charge. Neutral HMOs, containing some of the most abundant HMOs like 2'-fucosyllactose or lacto-N-tetraose, lowered pathology scores to 1.18±0.50 (—p<0.05). While the −1, −3, and −4 charged HMO fractions had no effect, the −2 charged fraction lowered pathology scores to 0.44±0.42 (—p<0.001). These results showed that not all HMOs are protective and that the most significant effects depend on the presence of two sialic acids. In the second dimension, we used gel exclusion chromatography to further separate the oligosaccharides in the −2 charged HMO fraction by size. Testing the subfractions in the neonatal rat model revealed one distinct HMO that reduced pathology scores to 0.64±0.41 (—p<0.001). While matrix-assisted laser desorption ionization–time of flight mass spectrometry provided first insights into the overall composition of the protective HMO, we used high-performance liquid chromatography-fluoresecence detection after sequential exoglycosidase digestion as well as gas chromatography–mass spectrometry analysis of partially methylated alditol acetates (PMAA) derivatives to determine the exact positions and linkages of the different monosaccharide residue. This combined approach unambiguously identified HMO 2 as disiayllacto-N-tetraose (DSLNT) with the isomeric configuration NeuAcα2-3Galβ1-3[NeuAcα2-6]GlcNAcβ1-3Galβ1-4Glc. Linkage-specific neuraminidase treatment confirmed that both sialic acids are required for DSLNT to protect neonatal rats from NEC, indicating high structure specificity.
We report that a single HMO, DSLNT, improves survival and reduces NEC in neonatal rats. The underlying mechanisms, however, remain to be elucidated. The high structure specificity suggests that specific receptors are involved, which could be expressed by either the host or certain intestinal microorganisms.
Due to the limited amount of available HMOs, the neonatal rat NEC model was the most feasible approach to test our hypothesis that HMOs protect from NEC and to identify individual protective HMOs. The rat model itself, however, has its limitations, and whether our results translate to human infants needs to be confirmed. If additional studies confirm the benefits of DSLNT for human infants, it might be a valuable supplement to prevent NEC in infants who do not receive human milk.
The inter- and intrapersonal variations in the DSLNT concentration of human milk may provide one explanation for why some breastfed infants still develop NEC. Some mother's milk may simply not contain sufficient amounts of DSLNT to protect the infant from NEC. If this is true, the concentration of DSLNT in the mother's milk may become a noninvasive biomarker to identify breastfed infants at risk to develop NEC.
References
5. Experimental NEC and Its Relationship with Foetal and Early Neonatal Nutrition
Necrotizing enterocolitis (NEC) results from a combination of intestinal immaturity and inappropriate responses to enteral nutrition and microbial colonization. The relationship among these determinants is poorly understood, and this inhibits prevention of the disease. NEC is among the most serious diseases for preterm infants, but factors indicated to protect against NEC in preterm infants might be important for gut health and body growth in healthy infants also. For infants in general, adequate nutrition in the immediate postnatal period is believed to be important for later organ development and health. The preterm gut is particularly sensitive to enteral feeding. Enteral milk feeding helps the gut to adapt and grow but may also provoke gut inflammation via maldigestion, nutrient fermentation, decreased barrier function, and bacterial overgrowth. Tumor necrosis factor-α, Toll-like receptors, and heat-shock proteins are identified among the immunological components of the early mucosal dysfunction. It remains difficult, however, to distinguish between the early initiators of NEC and the later pathological consequences of NEC. To elucidate the diet- and microbiota-dependent mechanisms and to identify clinical interventions, animal models showing spontaneous NEC development after preterm birth are important. So far, the pig is the only animal that has been reported to spontaneously develop NEC-like symptoms in response to preterm delivery and enteral milk feeding. In this review, we summarize some results from preterm pigs on the nutritional, microbial, and immunological interactions during the early feeding-induced mucosal dysfunction and NEC progression. We show that introduction of suboptimal enteral formula diets, coupled with parenteral nutrition, predisposes to NEC, while increasing the amount of mother's milk from birth protects against NEC. However, it remains difficult to know the exact time, amount, and diet of enteral food introduction for preterm newborns. Our studies in pigs suggest that enteral food should be initiated within a few hours after preterm birth and that trophic feeding with minimal enteral nutrition (15–25 mL/kg/day) should be continued for 2–4 days before transition to higher volumes of enteral milk. In pigs (and probably in infants) natural milk, even from another species (bovine colostrum, human or bovine milk), consistently provides better NEC protection than processed infant formula products. On the other hand, enrichment of infant formula with lactose, oligosaccharides, and bioactive whey ingredients may improve intestinal responses when mother's milk is not available. Numerous other bioactive milk factors remain to be investigated, but it is unlikely that one component alone will mimic all the beneficial actions of mother's milk. Decreasing gestational age at birth induces greater structural, functional, and immunological responses following formula versus mother's milk, and these gut responses to the first milk are similar in normal and low birth weight preterm newborns. The transition from parenteral to enteral nutrition after birth plays a pivotal role to secure gut growth, digestive maturation, and an appropriate response to bacterial colonization in the sensitive gut of preterm neonates. Studies in preterm pigs may help to elucidate mechanisms and to identify the optimal time, amount, and diet of enteral milk to preterm infants. The fact that introduction of feeds and microbial colonization of the intestine are essential for NEC development raises the possibility that an underlying inability of the premature infant to tolerate bacterial products and feeds may be central in NEC pathogenesis. We show that there is a direct relationship between the severity of NEC lesions and the functional response of the intestine such as the magnitude of sugar malabsorption that is detectable before clinical symptoms are evident. Stimulation of intestinal tissues with bacterial ligands decrease sugar absorption, but preterm pigs are not more sensitive than term pigs. Studies in infants and rodents indicate a hyper-responsive state in the fetus followed by acquired immunological tolerance to endotoxin after birth. However, we show that a degree of prematurity similar to that in NEC-sensitive preterm infants does not increase the intestinal endotoxin responses in pigs, and we therefore suggest that key functional and immunological responses of the developing intestinal epithelium is not markedly affected by moderate reductions in gestational age at birth. These and other results demonstrate that interactions among nutrition, microbiota, and immunity are crucial in NEC development but may vary among species when they lead to similar tissue pathological end points.
6. From Kangaroo Mother Care to Breastfeeding for the Competent Preterm Infant
Breastfeeding can be introduced as soon as infants do not require ventilator/continuous positive airway pressure (CPAP) treatment, irrespective of current postmenstrual or postnatal age, from 28 weeks, without any program for oral stimulation or assessment of readiness for oral feeding. Delayed introduction deprives mothers of optimal opportunities for establishment of lactation/breastfeeding and “becoming a mother.”
Breastfeeding outcome was explored in 15 very preterm singletons, born at a median (range) of 29 (26–31) weeks (Nyqvist, 2008). Fourteen had received ventilator/CPAP treatment and additional oxygen. Unrestricted kangaroo mother care (KMC) was encouraged. Breastfeeding was initiated at 31 (29–33) weeks, cup feeding at 33 (31–36) weeks, semi-demand feeding (prescription of total daily volume, unregulated; not fixed hours; breastfeeding with occasional cup/tube feeding when required) at 34 (32–36) weeks, and early discharge at 36 (33–39) weeks. Breastfeeding at early discharge was done by 12 exclusively and two partially. exclusive breastfeeding was attained at a postmenstrual age of 35 (32–38) weeks. One exclusively breastfed infant with bronchopulmonary dysplasia came home with additional oxygen.
KMC was defined as early, prolonged, and continuous (24/7) skin-to-skin contact between a mother and her low birth weight (<2,500 g) infant, in the hospital and after early discharge, with (ideally) exclusive breastfeeding and adequate follow-up (Cattaneo et al., 1998a). However, KMC application differs considerably in timing of initiation and discontinuation, duration of sessions, and number of sessions per day (from 20 minutes/day to one/a few/24 hours/day).
Benefits of KMC include increased maternal milk volume (Hurst et al., 1997). Commonly, higher breastfeeding rates and longer duration are found at discharge. Despite variable extents of KMC, a systematic review by Carfoot et al. (2003) found longer duration in the KMC groups. A U.S. randomized controlled trial (RCT) found longer (5 vs. 2 months) exclusive and any breastfeeding in KMC dyads (Hake-Brooks and Anderson, 2008). In a Colombian RCT, both groups showed high exclusive (46% vs. 45%) and partial (52% vs. 47%) rates, but the rate receiving only formula was higher in the traditional care group (Charpak et al., 1997); a higher rate of KMC infants were breastfed until 3 months (Charpak et al., 2001). Higher rates of exclusive breastfeeding were also found in India (Suman et al., 2008) and in Ethiopia, Indonesia, and Mexico (Cattaneo et al., 1998b); the latter also noted better weight gain, earlier discharge, and mothers' preference for KMC. In another Indian RCT of preterm/small for gestational age infants, Rao et al. (2008) found better weight gain/day, more increase in length and head circumference, and lower incidence of hypoglycemia in the KMC group. Swedish very preterm infants who were breastfed at 1, 2, 5, and 6 months had spent more time with KMC/day (Flacking et al., 2011). In Zimbabwe, the survival rate in infants with continuous KMC with a body weight of <1,500 g improved from 10% to 50% and in infants weighing 1,500–1,999 g from 70% to 90% (Bergman and Jurisoo, 1994). A nasogastric tube was used while infants sucked at the breast, followed by cup+breast. The authors stated “Strict guidelines for weaning from the tube are not possible, must be done ‘by feel’ in collaboration with the mother, over a period of 1–2 weeks.”
In Colombia, the kangaroo feeding policy aims at exclusive/almost exclusive breastmilk feeding, from the mother's breast when possible, otherwise by tube/cup. At inadequate weight gain (<25 g/day) supplementation is given with high-calorie formula, when available. The goal is to approach the intrauterine growth rate during the third trimester (15–20 g/day) until 40 weeks. Ruiz et al. (2002) suggested a prediction model for early identification of infants needing supplementation. Feeding every 90 minutes during daytime and every 2 h during nights is recommended.
Problems have also been reported. In Brazil, mothers who left the hospital with exclusive breastfeeding abandoned exclusive breastfeeding at home because of perception of insufficient milk (Groleau and Cabral, 2009). A survey found that staff perceived support of breastfeeding KMC mothers as extra workload, “perhaps the most important barrier to KMC perceived by professionals” (Charpak and Ruiz-Pélaez, 2006).
The willingness of parents in Western societies to practice continuous KMC has been questioned. However, Swedish mothers and fathers preferred KMC 24/7 during their infants' hospital stay, taking turns (Blomqvist and Nyqvist, 2011; Blomqvist et al., 2011). Investigation of breastfeeding patterns is included in a Swedish prospective study of parents' use of KMC (to be published) in two neonatal intensive care units (NICUs). Parents in one NICU had opportunities to practice continuous KMC; the other NICU offered limited opportunities. The 104 infants were born at a mean (range) gestational age of 32 (28–33) weeks, with birth weights of 1,835 (740–2,920) g. Mothers completed 24-hour breastfeeding diaries at infants' corrected ages of 2, 4, 6, and 12 months. These reveal wide variations in frequency of sessions (mostly much higher than what is usual in hospital feeding guidelines), duration of sessions and total sucking time, intervals between sessions, and frequency of extremely short sucking sessions—probably natural sucking patterns (Table).
Sucking activity that only lasted a few seconds.
The mother actively woke up the baby for breastfeeding.
Day, 6 a.m. to before 10 p.m.; night, 10 p.m. to before 6 a.m.
The Uppsala NICU guidelines, based on parent–infant non-separation, include tube feeding infants in kangaroo position while sucking the breast. Parents commence tube feeding from the day of birth or soon thereafter. Cup feeding is introduced from 29 weeks and used in the mother's absence and when the infant is awake after nursing. Semi-demand feeding commences at signs of some milk intake at the breast.
7. Current Concepts in Vitamin D Requirements for Mother and Her Breastfeeding Infant
Almost four centuries ago, in 1620, the observation was made that children living in industrialized urban areas in Europe where there was limited access to sunlight were at higher risk of developing childhood rickets than those living in the countryside. It would be another 300 years before it was discovered that within skin, sunlight exposure led to the synthesis of a preprohormone vitamin D—Vitamin D was first “discovered” in the early 20th century as a substance that could be ingested from foods (and hence its designation as a vitamin) or could be made in the skin from the precursor 7-dehydrocholesterol to vitamin D following exposure of a specific wavelength of sunlight (ultraviolet B, 290–320 nm).
With improved techniques in the laboratory and a subsequent explosion of data in the 1980s, it was noted that breastfed infants were at higher risk of developing vitamin D deficiency than those who were formula-fed. Further investigation revealed that breastmilk itself was the culprit, and that compared with standard formula that contained 400 IU of vitamin D/L, human milk contained on average 70 IU of vitamin D/L. Yet, closer examination of the data revealed a selection bias in that the women tested were typically from higher latitudes with limited sunlight exposure. A study by Cancella et al. (1986) showed a direct association between breastmilk vitamin D content and maternal vitamin D status. Thus, those women who had marginal vitamin D status would have a diminished amount of vitamin in their breastmilk; conversely, those women replete in vitamin D would have enhanced transfer of vitamin D in their milk thus providing ample vitamin D substrate for their recipient breastfeeding infants.
It was not until the 21st century that maternal supplementation with higher doses of vitamin D up to 6,400 IU/day to enhance transfer into breastmilk and to the recipient breastfeeding infant was tested for its safety and effectiveness. In a National Institute of Child Health and Human Development 6-year grant, we tested the hypothesis that 6,400 IU of vitamin D/day would be the amount necessary to make the mother replete (similar to vitamin D status attained in living in a sun-rich environment with 5–9 hours of exposure per day), such that her milk would provide at least 400 IU of vitamin D/L and thus that her recipient infant would also be replete. Specifically, we tested this hypothesis in a randomized controlled two-center trial involving more than 300 mother–infant pairs. Women were randomized to receive 400 IU (control), 2,400 IU, or 6,400 IU of vitamin D/day. Infants of mothers in the control group received 400 IU of vitamin D/day, while those infants of mothers in the 2,400 or 6,400 IU groups received 0 IU (placebo). The 2,400 IU group was stopped after 3 years of enrollment, as there were a disproportionate number of infants with deficiency at 4 months of age compared with those in the 400 IU or 6,400 IU groups. Upon completion of the study, preliminary analysis suggests that the 6,400 IU group was superior to attaining maternal sufficiency when compared with the 400 IU group. In addition, those infants whose mothers received 6,400 IU/day only with placebo given to the infants did not differ from the infants supplemented with 400 IU of vitamin D/day. Thus, when lactating women achieved 25(OH)D levels of at least 60 ng/mL or greater, there was sufficient transfer of vitamin D into the milk without safety issues such that the recipient breastfeeding infant was replete.
The concept that human milk is deficient in vitamin D is obsolete based on these data. Whether a woman chooses to use sunlight or vitamin D supplementation to attain vitamin D sufficiency during lactation remains maternal preference. Strategies then to improve maternal vitamin D status will benefit not only the mother but also her breastfeeding infant.
8. Human Milk Lipids: Current Knowledge and Future Perspectives
Breastfeeding is considered the ideal mode of feeding healthy infants. 1 Exploration of the biology of human milk and lactation is desirable in order to better understand the physiology of breastfed infants. 2 Moreover, insights into the physiology of breastfeeding may provide some guidance for the nutrition of those infants who are not fully breastfed and receive infant formula, complementary foods, or enteral or parenteral nutritional support, 3 and it may provide guidance on the desirable nutrition of infants who are not fully breastfed and receive infant formula, complementary foods, or enteral or parenteral nutrition support. The compositional and biological effects of human milk lipids have received considerable interest regarding their modulating effects on growth, metabolism and functions. Dietary fat is the major source of energy for growing infants. In addition, dietary lipids provide the essential lipid soluble vitamins (A, D, E, and K) as well as ω-6 and ω-3 polyunsaturated fatty acids (PUFAs). Dietary lipids also modulate the taste and mouth feel of foods as well as the gastrointestinal physiology and motility. Following absorption, lipids modulate the metabolism of lipoproteins, eicosanoids, docosanoids, and other signaling molecules, and they markedly affect the functions of the cardiovascular, immune, and nervous systems as well as end points such as cardiovascular diseases, allergy, and cognitive development. The high rate of absorption and digestion of human milk lipids is due to their composition, the unique structural positioning of palmitic acid in the sn-2 position, and the enzymatic activity of human milk lipase (bile salt-stimulated lipase [BSSL]), which help secure an adequate dietary energy supply and improved uptake of cations such as calcium. Recent randomized clinical trials using BSSL in preterm infants fed pasteurized human milk or preterm formula demonstrated a marked benefit on growth rates. Human milk lipid content varies among women and throughout lactation. 4 During the first 6 months of lactation monounsaturated fats contributed the majority of human milk fat (42–47%), followed by saturated (38–43%) and polyunsaturated fats (13–17%). Palmitic acid was the major contributor of saturated fat (25%). 5 Recent data show marked effects of maternal variation in the genotype of fatty acid desaturases (FADS1 and FADS2) on the PUFA content of human milk, 6 which may have a major impact on child development.7,8 Accumulating evidence supports the conclusion that maternal long-chain (LC)-PUFA intake may benefit infant development. In children with an FADS genotype associated with lower LC-PUFA synthesis, breastfeeding providing LC-PUFA achieved a more marked benefit for the child's IQ at school age than in those who had a higher ability for PUFA conversion. 9 Women who do not regularly consume fish are advised to take a supplement providing an average intake of at least 200 mg of docosahexaenoic acid /day.10,11 In conclusion, the composition of human milk lipids is complex and shows large inter- and intra-individual variation among lactating mothers as well as changes within feedings, during the day, and over the course of lactation and with genetic variation. This variation appears related to child outcome.
References
9. Body Composition of Human Milk-Fed Newborn Infants: Plethysmographic Finding
Nutrition in early life may exert programming effects on disease risk later in life through the modulation of growth pattern and body composition. Accurate and noninvasive measurement of infants' body composition represents a useful tool in assessing the quality of weight gain in addition to the quantity of growth.
With regard to the physiological postnatal weight loss, research has focused the attention in understanding the nature of the body composition modifications that occur during the initial days of life in order to provide a baseline and crucial information on the additional risk posed to at risk infants (i.e., preterm or intrauterine growth restricted) that lack energy stores at birth. Roggero et al. 1 have recently investigated the composition of losses that accompanies normal postnatal weight loss in 202 (cross-sectional sample) and 28 (longitudinal sample) full-term, breastfed newborns by means of an air plethysmography (ADP) system. Mean percentage of fat mass significantly decreased from birth (10.46±3.25%) to Day 3 (8.56±3.47%) (—p<0.031) in the cross-sectional sample and from birth (9.29±3.03%) to Day 4 (8.13±3.76) (—p<0.001) in the longitudinal sample. Fat free mass also decreased significantly (—p<0.001) during the first 4 days of life both in the cross-sectional (–261.71 g) and in the longitudinal (–152.18 g) samples. These results indicate that the postnatal weight loss in healthy, full-term, breastfed newborns is due to a reduction in both the quantity of fat mass and fat free mass. However, the percentage reduction in fat mass was greater than that in fat free mass.
The clinical value of the body composition assessment is further enhanced by the availability of reference data that allow an accurate estimation of the energy and nutrient requirements and the evaluation of the normal growth and nutritional status of pediatric populations.
The World Health Organization recommends breastfeeding as the optimal nutrition for infants. Exclusively breastfed infants have been reported to have a growth trajectory different from that of formula-fed infants. In addition, type of infant feeding seems to influence body composition development. Hence, body composition reference data (age and sex specific) developed using a “prescriptive” approach, that is, how children “should grow” if exclusively breastfed for the first 6 months of life, are needed.
Data on longitudinal changes of fat and fat-free mass from birth up to the sixth month of life in exclusively breastfed infants assessed by an ADP system have been recently reported.2,3 Roggero et al. 2 evaluated the body composition changes in a cohort of 59 Italian singleton, healthy, full-term infants. Fields et al. 3 conducted a multicenter cohort study and reported the data related to the changes in fat mass and fat free mass in 160 singleton, healthy, full-term infants, recruited at birth from three U.S. medical centers. All infants in both studies were exclusively breastfed for 6 months, according to the World Health Organization's definition. Percentage of fat mass increased significantly (—p<0.001) over the first 4 months of age, in both genders. Italian newborns showed a percentage of fat mass lower than that of U.S. newborns at birth (8.69±3.09% vs. 13.19±2.27% for females and 8.94±2.78% vs. 10.66±2.84% for males). At 1 and 2 months of age percentage of fat mass was still lower in Italian females compared with U.S. females (16.12±5.22% vs. 19.38±3.96% and 22.42±3.97% vs. 24.03±3.67%, respectively). However, Italian females reached values of fat mass similar to those of U.S. females from the third month of life (25.95±3.72% vs. 26.56±4.21%). Italian males, in contrast, showed a percentage of fat mass slightly higher than that exhibited by U.S. males at 2 months (24.69±3.99% vs. 22.70±4.29%), at 3 months (27.25±4.16% vs. 24.65±4.21%), and at 4 months of life (28.28±4.47% vs. 25.29±4.29%).
These findings could be partially explained by the fact that the genetic background may play an important role in affecting the growth process. In addition, the differences in body composition between the Italian and the U.S. centers may be also due to the fact that both maternal prepregnancy body mass index and gestational weight gain affect fetal growth. Indeed, Italian mothers showed lower maternal prepregnancy body mass index and gestational weight gain compared with U.S. mothers (21.8±3.35 vs. 25.5±5.8 kg/m2 and 12.7±3.78 vs. 14.8±4.9 kg, respectively).
The plethysmographic findings from these studies indicate the occurrence of a rapid accretion of fat mass during the first 2 months of life followed by a gradual rate thereafter and represent a first step in establishing normative body composition values for both boys and girls in early life.
The ADP system is currently becoming one of the most utilized technique for assessing body composition as it allows noninvasive and repeated measurements, providing further insight in the dynamic and rapid changes in fat mass and fat-free mass that characterize the first crucial months of life.
References
10. Ultrasound Imaging: A Technique for Tracking Premature Infant Body Composition
Reference
11. Short and Long Term Consequences of Feeding Very Low Birth Weight Infants Born to HCMV-Seropositive Mothers
Human milk is a substance of unique composition for enteral feeding, ideal for growth and development of infants, in particular, for preterm infants. Breastmilk reduces the risk of necrotizing enterocolitis, nosocomial infections, retinopathy of prematurity, and the time of total parenteral nutrition and leads to a better neurodevelopmental outcome in preterms. 1 However, there is a relevant risk for postnatal transmission of human cytomegalovirus (HCMV) up to 40% if fresh untreated breastmilk is fed 2 and around 10–15% if thawed frozen breastmilk is given to very low birth weight infants of HCMV-seropositive mothers. 3 In most cases, these postnatally acquired HCMV infections are asymptomatic. As a short-term consequence symptomatic HCMV disease occurs in 0–35% (median, 3.7%) with thrombocytopenia, sepsis-like syndrome, neutropenia, hepatosplenomegaly, elevated liver enzymes, pneumonia, 4 and an extended hospital stay. 3 In some cases, HCMV transmission via fresh breastmilk can lead to severe morbidity and mortality in preterm infants. 5
Concerning the long-term consequences due to postnatal acquired HCMV infections of preterm infants, Vollmer et al. 6 found no negative effect on neurodevelopment and hearing in 2–4.5-year-old children after early postnatal HCMV infection. The same cohort was additionally examined at school age. 7 In this study the overall performance in assessments of cognitive and motor function was in the normal range. However, poorer outcome was observed in the 20 early postnatal HCMV-infected infants compared with the 21 HCMV-negative controls.
The questions arise of how HCMV transmission via human milk could be prevented, how each method of prevention affects the quality of breastmilk, and what that finally means to the preterm infants.
Heating, as either Holder pasteurization (heating at 62.5°C for 30 minutes) or high-temperature short-term pasteurization (heating at 62–72°C for 5 seconds), eliminates the viral load but also affects relevant bioactive factors and nutrients of human milk. Freezing of breastmilk at −20°C preserves the nutritional, immunological, and endocrinological quality of human milk and reduces HCMV infectivity in vitro, but it does not eliminate HCMV viral load reliably. These conflicting data lead to inconclusive current international recommendations concerning the enteral feeding of very low birth weight infants of HCMV-seropositive mothers. The American Academy of Pediatrics states that fresh mother's own milk is preferable for routinely feeding all preterm infants. 1 Contrary to this, the French Society for the Safety of Nutrition proposes not to feed fresh milk to preterm infants <32 weeks in gestational age or <1,500 g in birth weight born to HCMV-seropositive mothers. They recommend that the milk should either be lyophilized (freeze-dried) or pasteurized. 8 The Commission on Nutrition of the Austrian Society for Children and Adolescent Medicine supports either freeze-thawing or pasteurization of breastmilk, 9 and the guidelines of the Swedish National Board of Health and Welfare recommend the freezing of milk from HCMV-seropositive mothers for preterm babies <32 weeks of gestation. 10
As a result it is not surprising that preterm babies <32 weeks in gestational age or <1,500 g in birth weight born to HCMV-seropositive mothers are fed with different regimens in Germany, Austria, and Switzerland including untreated, freeze-thawed, or long- and short-term pasteurized breastmilk. Additionally, 28% of German neonatologists feed these patients with formula milk to avoid HCMV transmission, 11 which is, to my knowledge, not recommended by any guideline. All these different feeding regimens have their own short- and long-term consequences to very low birth weight infants born to HCMV-seropositive mothers.
Further investigations are urgently needed to establish a method that prevents HCMV transmission via breastmilk reliably, is feasible in clinical daily life, and preserves the unique qualities of mother's milk for preterm infants.
References
12. Does Breastfeeding Reduce the Risk for Immune-Mediated Diseases?
There are specific difficulties when comparing outcomes in breastfed infants with those of formula-fed infants. It is unethical and not feasible to randomize healthy term infants to their mode of feeding. In most cases this precludes the use of blinded, randomized controlled trials, which have the highest degree of scientific evidence. Moreover, breastfeeding is not clearly defined and varies in exclusivity and duration, and the nutrient intake is not known. For formula-fed infants outcomes vary with type of formula. These factors and the fact that confounding factors are not evenly distributed between breastfed and formula-fed infants make it difficult to compare studies and to make systematic reviews and meta-analyses of pooled data. Bearing these precautions in mind, breastfeeding compared with formula feeding is considered to confer both short- and long-term health benefits on recipient infants. Among the long-term benefits is a possible reduced risk of developing immune-mediated diseases (e.g., allergic [atopic] diseases, celiac disease, type 1 diabetes [TID], and inflammatory bowel disease [IBD]).
Whether or not breastfeeding reduces the risk of allergy has been a hot topic for decades. Animal experiments as well as several meta-analyses published before 2007 found probable evidence that exclusive breastfeeding protects against asthma, wheezing, and atopic dermatitis. More recent meta-analyses on the relationship between exclusive breastfeeding and atopic disease have not supported these conclusions, and there are even studies suggesting that breastfeeding might increase the risk. Disregarding this, exclusive breastfeeding for 4–6 months of age is recommended irrespective of the relative risk of the infant to develop atopic disease.
The largest study on breastfeeding and celiac disease (i.e., the case referent multicenter study resulting from the Swedish “epidemic” of celiac disease in children below 2 years of age, which lasted from the mid-1980s for a little more than a decade) strongly suggested that breastfeeding reduces the risk to develop celiac disease. The conclusion was that introducing gluten-containing complementary foods into the infant's diet in small, gradually increasing amounts while the infant is still breastfed reduces the risk. To find out if the mode of introduction really affects the occurrence of the disease, or merely its clinical expression, a large two-phased cross-sectional screening study was recently carried out to which more than 13,000 12 year olds from two birth cohorts were invited: children born during the epidemic (1993) typically introduced to gluten in relatively large amounts from 6 months of age, often after being weaned, and children born after the epidemic (1997), who were introduced gradually to gluten from 4 months of age, often while still being breastfed. The total prevalence of celiac disease was 29/1,000 and 22/1,000 in the 1993 and 1997 cohorts, respectively (prevalence ratio, 0.75; 95% confidence interval [CI], 0.60–0.93; p=0.01). This suggests that introducing gluten-containing complementary foods from 4 months of age while the infant is still breastfed reduces the risk to contract celiac disease until 12 years of age. While a meta-analysis also concluded that breastfeeding compared with formula feeding reduces the risk, all studies have not confirmed this. Other studies have concluded that age at introduction might be more important (i.e., that there is an immunological window, possibly between 4 and 6 months, during which the chance to develop tolerance to new food antigens is particularly high). However, from an immunological point of view such a distinct window is not obvious in the human. Recently, there has been a paradigm shift from later is better to earlier is better in terms of introducing strong food antigens. Ongoing studies will confirm if this is true and, if so, reveal if this is due to an immunological window, or that earlier introduction results in more infants being introduced to such allergens while still being breastfed, or both.
Two meta-analyses suggest that breastfeeding for at least 3 months reduce the risk of childhood T1D compared with breastfeeding of shorter duration. Some, but not all, later studies have been supportive, including a case-sibling study suggesting that infants with T1D had been breastfed for a shorter duration than their siblings. However, data on duration of breastfeeding were collected retrospectively. It still remains an open question if it is early exposure to cow's milk protein (in formula) that causes the risk or if breastfeeding indeed is protective. Large ongoing studies will most likely give the final answer.
With respect to IBD, data are conflicting. A recent systematic review in which seven studies were included found that breastmilk exposure had a protective effect against childhood onset of IBD (odds ratio [OR], 0.69; 95% CI, 0.51–0.94; p=0.02). There was no significant effect for ulcerative colitis or Crohn's disease when analyzed separately. However, also for IBD the effect remains controversial.
In a community-based health survey including more than 18,000 individuals, 136 women being incidence cases of rheumatoid arthritis (RA) were identified. When compared with four matched female controls for each case, a longer history of breastfeeding was associated with lower risk for RA for women who had breastfed for longer than 13 months (OR 0.46; 95% CI 0.24, 0.91) and for those who had breastfed for 1–12 months (OR 0.74; 95% CI 0.45, 1.20) compared with those who had never breastfed also when adjusted for smoking and level of education. Whether being breastfed reduces the risk of developing RA is still controversial.
In conclusion, there are numerous reasons why breastfeeding, conferring the many immune-modulating and antimicrobial factors in breastmilk on the infant, together with its effect on gut microbiota composition should affect the immature immune system of the breastfed infant and, consequently, the risk to contract immune-mediated diseases. Therefore, it may seem surprising that the evidence based on clinical studies, including systematic reviews and meta-analyses, is relatively weak and for most of the diseases still controversial. This may reflect the difficulty in conducting proper studies on the outcomes of breastfeeding but could also reflect that the size effects are generally small and in many cases of relatively minor importance for the individual infant while the effect on the population level still may be significant.
13. Can We Define Lactational Mastitis?
Lactational mastitis is a common and problematic complication of breastfeeding. It makes mothers feel very ill and may lead to premature weaning. The wide range of incidences reported in the scientific literature (2.6% and 33%) suggests that there is some dissension about the definition of the disease. In 2010, a concept analysis 1 of the usage of the term “lactational mastitis” in contemporary scientific literature confirmed the problem of defining the ailment.
Although the symptoms are generally agreed upon, we still have no clear consensus about the cause of these symptoms. Theories include permeation of the breastmilk into breast tissue, caused either by simple fullness of the ducts or by blocked ducts, an active immune response, and the effect of cytokines leaking through, what should be, tight cell junctions.
Recent clinical and bacteriological research has revealed that healthy breastfeeding women have an abundance of bacteria in their breastmilk, including both potential pathogens and probiotics.2–4 Moreover, potential pathogens have been found in similar concentrations in the milk of breastfeeding women both with and without symptoms of mastitis. 4
These findings suggest a normal bacterial flora in the breastmilk of lactating women, which might seem obvious but is something that has only recently been clearly expressed in the literature.
If milk containing a diversity of bacteria is pressed out into the connective tissue of the breast, the subsequent immune response will give rise to all the symptoms of mastitis that we are familiar with: sudden onset, pyrexia (at times extreme), breast tension, erythema, and pain. Although interesting, one more theory of the etiology of symptoms does nothing to help us decide on an operational definition for mastitis.
References
14. Appropriate Treatment for Infectious Mastitis During Lactation
Breastmilk is a source of bacteria (<103 colony-forming units [CFU]/mL of milk) to the infant gut. Staphylococci, streptococci, and lactic acid bacteria are among the predominant cultivable bacteria. Therefore, this fluid plays a key role in the acquisition of the infant gut microbiota. However, there are a variety of factors that may lead to the development of an infectious mastitis, the main medical cause for early weaning. This process of mammary bacterial dysbiosis is characterized by a high increase in the concentration of the etiological agent(s) (>104 CFU/mL of milk) and the disappearance of other bacteria that are usually present in human milk. Such microbial alteration is the main responsible for the inflammatory state and the obstruction of the mammary ducts.
The main etiological agents of mastitis belong to the genera Staphylococcus (Staphylococcus aureus, Stapylococcus epidermidis), Streptococcus (Streptococcus mitis, Streptococcus salivarius, etc.), and, at a lower extent, Corynebacterium. S. aureus is the main etiological agent of acute mastitis, a process easily diagnosed and generally characterized by an intense local inflammation accompanied by systemic flu-like symptoms and that, eventually, may lead to breast abscess. These are the prototypical cases of “mastitis,” but, actually, they represent a small percentage of infectious mastitis. A higher number of cases can be classified as subacute mastitis, a process characterized by a pricking or needle-like pain or a burning breast pain. They are usually due to overgrowth of coagulase-negative staphylococci or viridans streptococci in the mammary ducts and are widely underrated owing to the absence of breast redness and systemic symptoms. Independently of the species, mastitis-causing strains generally share some properties, such as ability to form dense biofilms, resistance to methicillin and other clinically relevant antibiotics, and mechanisms to evade the action of the immune system. On the other hand, despite the existence of unjustified beliefs, the incidence of yeasts as an agent of infectious mastitis (or even sore nipples) is extremely low.
Milk cultures and antibiograms would facilitate a rational treatment of the different types of mastitis, but microbiological analyses of human milk are not performed routinely. In this context, the clinician should be able to associate each type of mastitis with its characteristic symptoms and the most adequate therapeutic approach.
A β-lactam antibiotic (cloxacillin or amoxicillin with or without clavulanic acid) used to be the first choice to treat acute mastitis. Generally, the best option in the absence of a milk culture is amoxicillin/clavulanic acid (1,000/62.5 mg) in a depot presentation. Cloxacillin has been widely used for this purpose, but its efficacy has decreased notably owing to the rise of resistant strains. Approximately 50% of the abscess-causing S. aureus strains are resistant to methicillin. Many times, the clinician tends to prescribe low antibiotic concentrations because of the potential transfer of residues to milk; however, the concentration in milk is not directly proportional to the dose, and, often, low concentrations foment the selection of antibiotic-resistant bacterial cells. In this context, the easily accessible information provided by high-quality databases on the compatibility between breastfeeding with pharmaceutical drugs (http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACT and www.e-lactancia.org) may be very useful to the clinician. The treatment of acute mastitis with a β-lactam antibiotic may lead to three situations: (a) the treatment is successful; (b) the treatment is unsuccessful; and (c), more frequently, the treatment is successful against S. aureus, but it induces a selective growth of coagulase-negative staphylococci, leading to a subacute mastitis.
Generally, the agents responsible for subacute mastitis are more resistant to antibiotics than S. aureus, but, fortunately, they are more sensitive to probiotics, which are defined as living microorganisms that exert beneficial effects to the host. Recently, two clinical trials have shown that specific Lactobacillus strains isolated from breastmilk represent an efficient alternative to antibiotics for the treatment of infectious mastitis, lacking the secondary effects associated to antibiotherapy (candidiasis, diarrhea, etc.). More specifically, some Lactobacillus salivarius strains lead to a full recovery in more than 90% of the cases. Hopefully, such strains will be commercialized soon. Meanwhile, there are some probiotic products available in the pharmacy, although, unfortunately, their efficacy is notably lower (<30%) since the properties of the strains that they contain is different because their target (pediatric infectious gastroenteritis) is also different.
If the clinician prefers an antibiotic to treat a subacute mastitis, then it would be preferable to avoid the use of β-lactams due to the widespread resistance of coagulase-negative staphylococci to such drugs. The alternative would be other risk antibiotics that traditionally have not been had in account during breastfeeding, such as ciprofloxacin. Several years ago, there was a controversy since it was announced that quinolones may have negative effects on the growth of cartilage in ducks. Subsequent studies revealed not only that such a group of antibiotics (and, in particular, ciprofloxacin) has no adverse effect on human cartilage development, but also that it is one of the safest antibiotics for neonates and infants, and one of the best options if prolonged antibiotherapy (e.g., cystic fibrosis) is required.
Anyway, the percentage of mastitis cases that are completely solved by antibiotherapy is low, even when an antibiogram is available. This fact is due to three basic reasons: (1) the continuous increase in the number of resistant strains among the community; (2) the formation of dense biofilms that are highly refractory to antibiotics; and (3) the coexistence of staphylococcal/streptococcal strains with different susceptibility to the same antibiotic.
It must be highlighted that the treatment of any type of infectious lactational mastitis cannot rely exclusively on an anti-infectious therapy (either an antibiotic or a probiotic) but must be accompanied or complemented by an anti-inflammatory therapy. In these cases, the antimicrobial therapy often fails since it is unable to reduce the inflammatory response rapidly. The anti-inflammatory therapy choice should be a non-steroidal drug. Paracetamol and ibuprofen should be alternated if fever is present, but it would be preferable to use ibuprofen exclusively if there is no fever. Steroidal drugs must be avoided since, although they may provide a temporary relief, they favor the undetected progression of the infection.
15. Breastfeeding After Breast Cancer
Breast cancer is the most frequent malignant tumor that occurs in women during reproductive age. Around 6% of breast cancer patients are less than 40 years of age at diagnosis, with a yearly incidence of 2,420 new cases in Italy.
Due to the advances in the in the field of adjuvant treatments, 5-year survival of breast cancer in young women is around 86%, with an estimated prevalence of 25,000 women, according to the Italian Association of Tumor Registries. 1 Therefore, patients' enquiry into the possibility of subsequent pregnancies and breastfeeding is increasingly encountered.
Current evidence suggestd that breast cancer survivors who have a pregnancy after treatment completion are not at increased risk of death. A recent meta-analysis on 14 studies that enrolled 1,244 cases and 18,145 controls has shown that the pooled relative risk (PRR) of death was 0.59 (95% confidence interval [CI] 0.50–0.70). When controls free of disease at least as long as the time to pregnancy were chosen, the PRR was 0.85 (95% CI 0.53–1.35). 2 Thus pregnancy after breast cancer is safe and should not be discouraged.
Breastfeeding in patients with previous breast cancer is still considered cumbersome and unfeasible. The breast treated with conservative surgery and subsequent radiation is less responsive to hormonal stimulation, with reduced glandular hyperplasia and hypertrophy. Milk production is usually decreased, and surgery may affect duct integrity.
Nonetheless, previous surgery and radiation or the absence of one breast are not contraindications for exclusive breastfeeding. Each breast has the capability to self-regulate milk production according to the baby's suckling habits, and many evidence (including breastfeeding of twins) supports the notion that one breast is enough for successful breastfeeding. Specific education programs should focus on adequate baby positioning, correct latching, and reinforcement of the advantages of on-demand breastfeeding. Data from our group demonstrate the feasibility of breastfeeding after breast cancer but also highlight some problems. Twenty patients who had 21 births after breast cancer were interviewed. 3 Breast conservative surgery was performed in 15/20 patients. Median age at delivery was 36 years, with a median time from diagnosis to pregnancy of 4 years. Ten of the 20 patients attempted breastfeeding. Four women interrupted lactation within 1 month: two for reduced milk production after formula supplementation and two for mastitis. The other six women breastfed for a median duration of 11 months (range, 7–17 months); all of them had had a breast-conserving surgery. Qualified lactation counseling was offered to five of the 20 women. All five women enjoyed a successful breastfeeding with a median duration of 12 months (range, 9–17 months). Reasons for not attempting breastfeeding were patient's choice in one case and medical counseling against breastfeeding in the other nine women. The main reported reasons were uncertainty regarding maternal safety and a priori unfeasibility expressed either by the obstetrician or by the medical oncologist. Other reasons included hepatitis C virus infection, maternal multiple sclerosis, twin pregnancy, and postpartum bleeding. Out of 15 women who underwent breast-conserving surgery and radiotherapy, 14 (93%) reported hypoplasia of the irradiated breast during pregnancy. Of these, eight of the 15 did not attempt breastfeeding, five attempted lactation from the unaffected breast only, and two attempted from both breasts. The main reasons for not attempting breastfeeding from the previously affected breast were difficulty in latching in two of five women, reduced milk production in two of five women, and breast pain in one woman. The two women who tried to breastfeed from both breasts succeeded in bilateral breastfeeding for only 2 weeks. Milk production from the previously treated breasts was significantly reduced in both women. These data confirm that breastfeeding is feasible also after breast cancer but underscore the importance of correct patients' support and the need of caregivers' educations. In our series, nine of 10 women who opted for bottle feeding did so because inadequate counseling by their doctors, who minimized the benefits of breastfeeding for both the newborn and the mother.
It is noteworthy that breastfeeding after breast cancer could exert a favorable impact on breast cancer prognosis. Data in the general population report a 4.3% less breast cancer incidence for each year of breastfeeding. In the high risk BRCA1 mutated population, breast cancer occurrence is reduced by 32% after 1 year of breastfeeding and by 49% after 2 or more years of breastfeeding beyond the first. 4 Possible explanations of reduced breast cancer incidence after breastfeeding include reduction in the number of potentially oncogenic breast stem cells, terminal maturation of the breast lobules, and epigenetic silencing of deleterious genes.
In patients with previously diagnosed breast cancer, data on the prognostic impact of breastfeeding are scarce. In the previously mentioned series, 3 no differences were observed in disease-free survival, with one local recurrence within the group who breastfed and one in the group who did not. In an unplanned analysis of 94 patients who had a pregnancy after breast cancer, 27 women breastfed their babies, and 25 did not. Overall survival was in favor of the group that breastfed, but no sound conclusion could be drawn from this work, owing to the limited number of patients involved. 5
In conclusion, breastfeeding in women with previously diagnosed breast cancer is feasible and safe. No reasons whatsoever should hamper the possibility for women who have had breast cancer and for their babies to enjoy the benefits of breastfeeding and being breastfed.
References
16. The Use of Antidepressants in Pregnant and Breastfeeding Women
The perinatal period is often associated with a number of neurologic complications, including depression, bipolar syndrome, and schizophrenia. Current estimates are that at least 10% and perhaps 15% of pregnant or breastfeeding mothers will suffer from depression alone. Previously, most mothers simply avoided drug therapy for this syndrome because of our limited knowledge about the teratogenicity of these products or their transfer into human milk. Then the risks of untreated depression became evident, along with an excessively high rate of severe relapse. Thus in the last decade we have re-evaluated the relative risks associated with the use of these drugs during pregnancy and breastfeeding.
At present we do not think that antidepressants as a family are highly teratogenic following exposure in utero. Thus far, selective serotonin reuptake inhibitors (SSRIs) are not considered teratogenic. It is well known that infants exposed to SSRIs during pregnancy often exhibit withdrawal symptoms or, more commonly termed, “discontinuation syndrome” following birth. This is simply a withdrawal syndrome, not dissimilar to that seen in adults who are rapidly withdrawn from these drugs. Discontinuation syndrome is characterized by poor adaptation, jitteriness, irritability, and poor gaze control after gestational exposure to SSRIs. While some symptoms observed in neonates could be due to the immaturity of the newborns' central nervous system, they could be due to characteristics of the medications themselves. SSRIs readily transfer via the placenta into the fetus, and plasma levels in the fetus are often comparable to maternal levels. The prevalence of discontinuation syndrome ranges as high as 30% in various studies and is highest in those infants exposed to the shorter half-life SSRIs (paroxetine, sertraline). Other more serious symptoms include mild respiratory distress (transient tachypnea of the neonate), occasionally hypotonia, and rarely pulmonary hypertension. These effects were especially likely when paroxetine was combined with clonazepam as clonazepam appeared to change metabolism of paroxetine. In most all cases, these symptoms rapidly dissipate with no long-term complications reported.
In breastfeeding mothers, the use of antidepressants has been extensively studied.
The SSRIs are presently the mainstay of depressive therapy, primarily because they are incredibly effective and have minimal toxicity in overdose. All SSRIs transfer to varying degrees into human milk. It is interesting that we have more published data on the transfer of SSRIs into human milk than any other drug class. Fluoxetine is the most studied drug, with more than 90 mother–infant pairs published. Fluoxetine levels in milk range as high as 14.6% of the maternal dose. Levels with most antidepressants tend to fall overtime postpartum, and levels after the first month are generally lower in most studies. Because of its long half-life active metabolite, clinically relevant plasma levels in infants have been reported. Owing to a higher relative infant dose, fluoxetine is perhaps less preferred unless lower doses are used during pregnancy and early postpartum. However, in reality, the incidence of untoward effects is probably remote, and mothers who cannot tolerate other SSRIs should be maintained on fluoxetine while breastfeeding. Clinical studies of breastfeeding patients taking sertraline, fluvoxamine, and paroxetine clearly indicate that the transfer of these medications into human milk is low and that uptake by the infant is even lower. Several studies of sertraline suggest limited gastric uptake in the infant for unknown reasons. Thus far, few untoward effects in the newborn have been reported following the use of these three agents in breastfeeding mothers, with exception of withdrawal. Sertraline appears to be the overwhelming favorite as more than 50 infants have been evaluated in numerous studies, and milk and infant plasma levels are quite low to undetectable.
In addition, it is now considered current practice to maintain pregnant and breastfeeding mothers suffering from depression, bipolar, and other mental disorders on their medications, as the relapse rate during pregnancy and breastfeeding is extraordinarily high, and the complications of mental disorders in parenting a child are enormous. Thus we generally suggest the clinician avoid changing types of SSRIs and, instead, leave the mother on the medication that has proven effective in the past.
Lastly, following many studies, long-term neurobehavioral outcome in the infant exposed to antidepressants appears good. No study to date has shown major or long-term complications with neurobehavioral development in infants exposed prenatally or postnatally to the antidepressant family of medications.
References
17. Antipsychotic Agents, Anxiolytics, Hypnotics and Sedatives During Breastfeeding
• Antipsychotics. In all, 58 articles regarded 11 of the 22 (50%) antipsychotics. Pharmacokinetic studies involved a total of 146 mother–infant pairs. The most studied drug was sulpiride (65 mother–infant pairs), followed by lithium (n=30), olanzapine (n=14), haloperidol (n=11), zuclopenthixol (n=7), and chlorpromazine (n=6). Adverse effects were reported in 11 of 162 (7%) monitored newborns: delayed psychomotor development, drowsiness and lethargy with chlorpromazine (4 of 20 newborns monitored), delayed psychomotor development with haloperidol (3 of 13), sedation and agranulocytosis with clozapine (2 of 4), and central nervous system depression symptoms (hypotonia, lethargy, hypothermia, inversion of electrocardiogram wave) and toxicity in concomitance with respiratory infections (2 of 32) with lithium.
• Anxiolytics. In all, 24 articles (26%) regarded 8 of the 15 (53%) anxiolytics. Pharmacokinetic studies involved a total of 58 mother–infant pairs. The most studied drug was pinazepam (13 mother–infant pairs), followed by clobazam (n=12), alprazolam (n=8), and diazepam (n=8). Adverse effects were reported in 5 of 29 (17%) monitored newborns: withdrawal syndrome after cessation of breastfeeding (irritability, high-pitched crying, agitation, or sleep disturbances), and sedation, nausea, or reduced suckling with alprazolam (3 of 7 newborns monitored), and sedation with diazepam (2 of 14).
• Hypnotics and sedatives. In all, 12 articles (13%) regarded 8 of the 13 (62%) hypnotics and sedatives. Pharmacokinetic studies involved a total of 61 mother–infant pairs. The most studied drug was zopiclone (15 mother–infant pairs), followed by nitrazepam (n=14) and temazepam (n=10). Sedation and poor feeding were reported in only 1 of 6 newborns monitored for zolpidem use (4% of all hypnotics and sedatives).
No pharmacokinetic or safety data were found for 44% of the psychotropic drugs considered. For 16 of the 27 drugs (59%) with documentation, the available data do not permit an evaluation of the drug's safety profile during breastfeeding, and for an additional five drugs (sulpiride, lithium, clozapine, clobazam, and diazepam) the high exposure dose (relative infant dosage >10% of maternal dosage) or observed adverse effects make their use unsafe.
Despite this, if an antipsychotic, anxiolytic, hypnotic, or sedative agent is needed during breastfeeding, the drug with the most favorable pharmacokinetic profile (half-life, milk/plasma ratio [M/P], relative infant dosage) and no reported infant adverse effects should be used: olanzapine and chlorpromazine as antipsychotics, short-acting benzodiapezines, such as oxazepam or pinazepam, as anxiolytics, and lormetazepam as a hypnotic and sedative drug. However, these drugs must be used with caution by breastfeeding mothers, taking into account that neonates metabolize drugs more slowly than adults and that these drugs are usually used for long-term periods and may therefore accumulate in breastfed infants and produce adverse effects. Moreover, the minimum dosage required for symptom relief should be used, and the infant should be monitored regularly.
References
18. Evidence-Based Breastfeeding Promotion: A Global Scaling Up Model
Reference
19. A Milk Oligosaccharide, 2'-Fucosyllactose, May Ameliorate Necrotizing Enterocolitis in Preterm Pigs
Necrotizing enterocolitis (NEC), a severe intestinal disease occurring in 5–10% of hospitalized preterm infants, is associated with exaggerated tissue responses to the gut microbiota. Mother's milk decreases the risk of NEC, potentially owing to bioactive compounds that modulate gut colonization and tissue responses. Human milk oligosaccharides (HMOs) are largely indigestible to infants but are found at concentrations up to 12 g/L in human breastmilk, while only trace amounts are present in cow's milk. Important biological functions other than nutritional have been documented for several HMOs such as prebiotic, anti-inflammatory, or antimicrobial actions. 2'-Fucosyllactose (2'-FL), which accounts for 75% of HMOs, has been shown to have prebiotic effects on bifidobacteria, while it potentially inhibits epithelial adhesion of pathogens owing to structural homology with intestinal bacterial receptors. We hypothesized that a 2'-FL-supplemented infant formula would modify the gut microbiota, decrease epithelial adhesion of pathogens, and thereby reduce the risk of NEC. To test the hypothesis, we used a sensitive model with cesarean-delivered preterm pigs that at a high proportion spontaneously develop NEC after 5 days of formula feeding.
Twenty-one newborn preterm pigs were fitted with umbilical catheters and orogastric tubes. Parenteral nutrition and minimal boluses of formula (3 mL/kg/3 hours) was given for 48 hours followed by full enteral feeding (15 mL/kg/3 hours) with control formula (n=11) or 2'-FL-fortified formula (5 g/L) (n=10). To standardize initial gut colonization, maternal fecal bacteria (2.5×104 colony-forming units) were given as an oral inoculum with the first minimal formula bolus. On Day 5, all pigs were euthanized for tissue collection and NEC evaluation.
Five 2'-FL pigs (50%) and nine controls (82%) developed NEC (—p=0.18) with a tendency to increased intestinal NEC lesions in controls compared with 2'-FL pigs (small intestine, 1.8±0.3 vs. 1.4±0.2, p=0.36; colon, 2.7±0.6 vs. 1.5±0.5, p=0.14). A 40% reduction of anaerobic bacteria was observed in cecum contents of 2'-FL pigs compared with controls (1.6×1010±9.8×109 vs. 2.7×1010±2.6×1010 colony-forming units/mL), but the decrease was not significant (—p=0.24). Bacterial density along the intestinal mucosa, as detected by fluorescence in situ hybridization of general bacteria, was similar between groups (—p=0.68). Similarly, there were no significant effects of the 2'-FL on intestinal structure and function, as assessed by intestinal wet weight, proportion of mucosa, villus height, in vivo lactose uptake capacity, and brush border enzyme (sucrase, maltase, lactase, and peptidases) activities.
Adding 5 g/L 2'-FL to infant formula tended to decrease the incidence and severity of NEC in preterm pigs. Since bacterial colonization and intestinal structural and functional parameters were not significantly affected, further investigations are needed to test if the given dose of 2'-FL potentially modified tissue responses to colonizing bacteria and enteral feeding. It should further be investigated if other doses of 2'-FL may more efficiently alter bacterial colonization or mucosal responses to diets and bacteria and thereby increase NEC resistance in preterm neonates.
20. Transcription of Mucin Genes in Lactocytes and the Mucin Content of Milk
21. RNA Sequencing of the Human Milk Fat Globule Transcriptome at Three Stages of lactation
22. Intergenerational Epigenetic Effects on Milk Production and Infant Condition in a Non-Human Primate Model
23. The Effects of Exercise and Calcium Intake During Early Lactation on Bone Mineral Density at One Year Postpartum
24. Documentation of the Fecal Microbiome of Breastfed and Formula-Fed Infants Using Culture-Independent Methods
Although it has long been assumed that the newborn infant's gastrointestinal (GI) tract is sterile at birth, researchers and clinicians know that an infant's complement of GI microbiota develops quickly during the first few months of life. Various factors including mode of feeding (breastfeeding vs. formula feeding) can affect which bacteria reside in the infant's GI tract. These bacterial community structures are thought to impact both immediate and long-term health such as risk for diarrhea and chronic conditions such as obesity and type 2 diabetes. Until recently, most examinations of fecal microbiota have utilized culture-dependent methodologies known to introduce bias into their interpretations. Thus, the main objective of this study was to characterize the fecal microbial ecology of breastfed and formula-fed infants during the first 2 months of life. Healthy pregnant women were recruited in their last trimester of pregnancy from the Moscow, ID–Pullman, WA area, and infant fecal samples were collected from 12 exclusively breastfed and two exclusively formula-fed infants at five time points during the first 2 months of life. When possible, meconium samples were also collected within 24 hours of birth. The bacterial profiles of the fecal samples were determined using Roche 454 sequencing of the DNA encoding for microbial 16S rRNA. Results indicate that infant feces harbor a wide range of microbial communities whose composition and diversity change over the first 2 months of life. Meconium samples were not sterile but instead contained a variety of microbial genera, including Comamonas, Leuconostoc, and Lactococcus with mean relative abundances of 35%, 7%, and 5%, respectively. Whereas Comamonas was present in amounts as high as 63% in meconium samples, it was rarely found in samples collected after Day 2 of life. In general, intersubject variability in bacterial community structure of the meconium samples was less than intersample variability within an infant over time. Mode of delivery (vaginal vs. cesarean) did not appear to influence the types of bacteria found in meconium samples. Feeding mode clearly influenced patterns of early change in the fecal microbiome. For instance, by Day 5 of life the mean relative abundance of Bacteroides was 97% and 12% for formula-fed and breastfed infants, respectively. Together, Bacteroides, Veillonella, Parabacteroides, Escherichia/Shigella, and Streptococcus represented 51% of the overall relative abundance in infant fecal samples collected between 2 days and 2 months of life. Analysis of the operational taxonomic units (OTUs) with 3% similarity across all samples revealed that the number of observed OTUs was low, ranging from 6 to 57 OTUs per sample. In conclusion, these preliminary data suggest that an infant's GI tract is not sterile at birth, the GI microbiome fluctuates during the first 2 months of life, and feeding mode influences this process. Further work is needed to determine the origins of an infant's GI microbiome and factors influencing its establishment.
25. Lactoferrin Modulates Lipopolysaccharide-Induced Perturbations in Gene Expression in Human Fetal Intestinal Epithelial Cells
Lactoferrin (Lf) functions in the orchestration of iron homeostasis, immune maturation, and proliferation of intestinal epithelial cells (IECs) in the breastfed infant. The exaggerated inflammatory response of enteropathogenic-derived infantile diarrheas is potentiated, in part, by exposure to lipopolysaccharide (LPS). Lf sequesters the lipid A moiety of LPS with high affinity and may dampen the effects of overt Toll-like receptor complex activation. In the present study, effects of Lf in the presence of LPS on the expression patterns of stress-response genes were examined using a fetal IEC model. FHs74 cells were treated for 24 hours with 400 μg/mL native (N)- and holo (H)- human (hLf), bovine (bLf), or commercially available bovine Lf (cbLf) with or without 1 μg/mL LPS. Cell viability was attenuated (>30%) by LPS challenge, an effect that was ameliorated by the addition of Lf(s). Using polymerase chain reaction (PCR) array profiling N-hLf treatment was determined to differentially modulate LPS-induced up-regulation of numerous intermediates and products of the nuclear factor-κB, mitogen-activated protein kinase, and Fas signaling pathways. Quantitative PCR was employed to validate PCR array findings that Lf(s) mediates perturbations of multiple pro-inflammatory cytokines due to LPS challenge, including interleukin-1, -6, and -8. Our findings suggest Lf may protect the neonatal intestinal epithelium against LPS by altering the expression of key regulatory genes associated with an LPS-derived inflammatory response.
26. Longitudinal Survey of Adherent Mucosal Microbiota in Hospitalized Preterm Infants
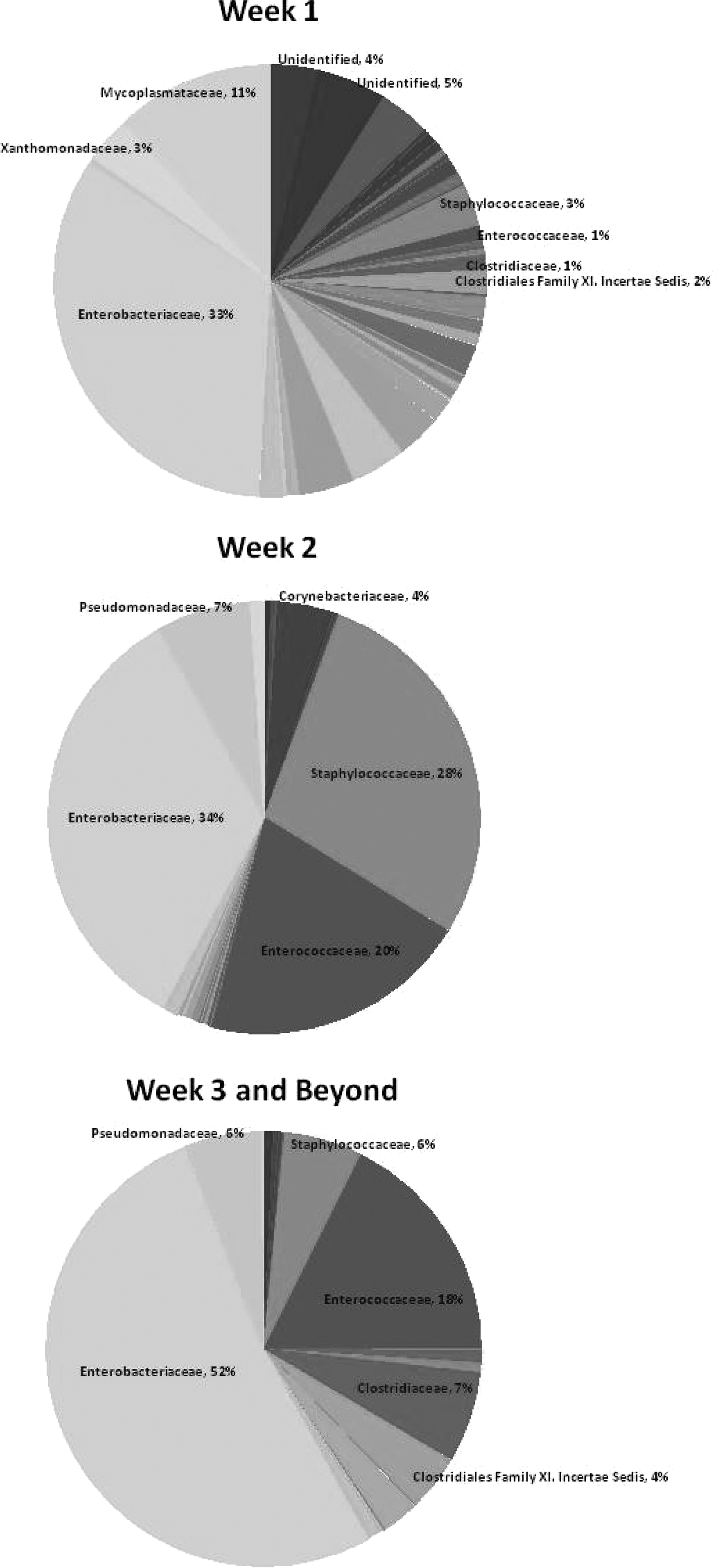
Bacterial families identified in the samples.
p=0.049 between Weeks 1 and 3–4.
27. The Effect of Different Collection and Processing Protocols on the Measurement of Vitamin D–Binding Protein in Human Breastmilk
Data are mean±SD (range) values.
Adjusted for subject and milk type.
Adjusted for subject and treatment type: p<0.0001.
DBP, vitamin D-binding protein.