
Abstract
Abstract
Breastfeeding is the biological norm for infant feeding but is also a social construct. As such, its rates and practices are determined by the same social determinants that shape health inequalities and inequities. In the past 30 years, several reports have drawn attention to the changing pattern of breastfeeding inequalities across countries and population groups. Breastfeeding rates tend to fall and rise following a similar pattern everywhere, although at different times and speed. The role of women within families and societies, the routines of maternity hospitals and other healthcare services, and the pressure exerted by the baby food industry are among the factors that influence the time and speed of changes in breastfeeding rates and practices across countries and population groups. Inequities (i.e., inequalities considered unfair and avoidable by reasonable action) can be redressed by interventions for the protection, promotion, and support of breastfeeding. Evidence-based and quality-implemented support and promotion activities, if applied without an equity lens, may increase inequities. Activities for the protection of breastfeeding (e.g., implementation and enforcement of the International Code of Marketing of Breastmilk Substitutes; legislations, regulations, and policies to remove obstacles and barriers to good-quality breastfeeding support and to protect women and mothers in the workforce; elimination of obstacles and barriers to breastfeeding anywhere, anyhow, and anytime mothers want) apply to all women and are less dependent on take up by the target population. If well designed and enforced, protective interventions contribute to reducing inequalities and inequities and to delivering promotion and support activities more effectively.
The availability of good medical care tends to vary inversely with the need for it in the population served. 1
Introduction
In a society, social norms on nutrition are determined by various factors, such as the level of economic development and the daily living conditions, the political and physical environment in which people live, the types of employment and work, the production and marketing of goods and foods, the structure of families and communities and the relationships among their members, the education and health systems, the way knowledge and information are disseminated, and so on. In a word, social norms are determined by social determinants—more precisely, by determinants that are in a state of constant change. That's why social norms constantly change.
The determinants of social norms also determine the way a society is stratified into social classes. These are the so-called determinants of social inequalities. 2 If infant feeding, as a social construct and norm, is subject to the same social determinants, inequalities in breastfeeding are to be expected in all societies and are in fact seen in all societies. In this article, I will present and discuss examples of inequalities in breastfeeding from an international perspective. I will then try to identify, among these inequalities, those that may be considered as unfair and unjust and as unnecessary and avoidable inequities. Finally, I will advocate for effective interventions and actions that, using an equity lens, may lead to better and, at the same time, less discriminatory breastfeeding rates and practices.
Inequalities
The first article I read that drew my attention to inequalities in breastfeeding rates was a critical review of the then available information on the prevalence and duration of breastfeeding, published by the World Health Organization (WHO) in 1982. 3 It was a review of several hundred national and local survey reports from more than 50 countries from which the authors tried to quantify trends. Despite differences in definitions and methods, the review revealed large inequalities among regions, countries, and population groups. Breastfeeding rates and duration were higher in rural and poor urban groups in sub-Saharan Africa and in Middle and Western-South Asia, but were already falling among the urban elite in some countries. In Eastern-South and East Asia rural prevalence was high, but duration was lower in some rural and urban groups, with an evident decline among the urban elite. In Latin America prevalence was high, but duration longer than 1 year was rare. Prevalence and duration were falling until about 1970 in Europe and North America, but recent increases were reported from some countries, especially in Northern Europe. Overall, the available data allowed identification of three phases (Fig. 1): An initial one with high prevalence and duration of breastfeeding across all population groups (Stage 1); a transformation phase with prevalence and duration falling first among the urban elite, then among the urban and rural poor (Stages 2–5); and a third phase of resurgence, in a sort of inverse pattern (Stages 6–8).
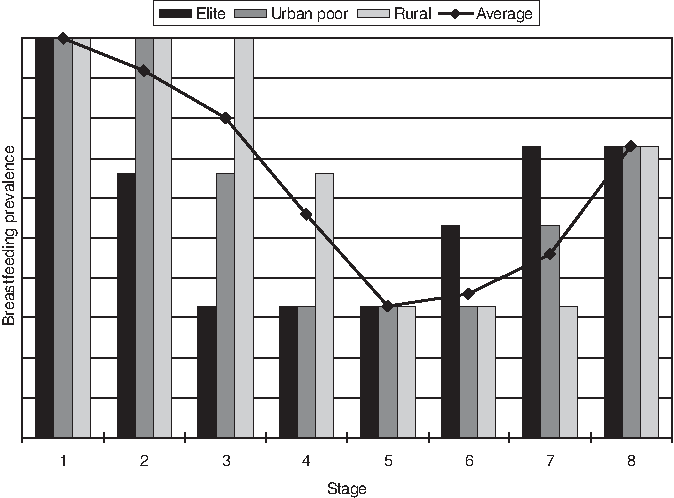
Prevalence and duration of breastfeeding across population groups: Phases and changes up to the early 1980s. Reprinted with permission from World Health Statistics Quarterly. 3
Many sub-Saharan African countries, including the one in which I was working at the time, Mozambique, were in Stage 1. Kenya, where I had worked some years earlier, however, had already moved to Stage 2, and indeed one could clearly see plenty of bottle feeding among the urban elite in Nairobi. Some South American countries—Chile, for example
4
—had already moved, decades earlier, to Stage 5, and there was no sign of resurgence yet. Scandinavian countries had already started to move up to Stages 6–8. I remember that when I read the WHO review my immediate thought was: How can Mozambique avoid moving away from Stage 1? Or, if it does move, how can the transition to Stage 8 and final complete resurgence be accelerated? To answer these questions, an explanation for the pattern of Figure 1 was needed. Were the urban and rural poor just imitating the urban elite? And if so, why? And what was the prime mover for the urban elite? The answer I gave at that time, as a young doctor interested in global public health, was that socioeconomic forces were pushing for the change:
• First, the role of women within the family and the society was changing, with greater opportunities for work not always compatible with child care and breastfeeding. • At the same time, modern maternity hospital care, based on the Fordist model of mass production, was spreading; in this model, formula feeding, controlled by health workers, was fitting better than breastfeeding, controlled by mothers and babies. • Finally, manufacturers of infant formulas were hungry for profit and eager to penetrate new markets using aggressive advertising through mass media and promotion through health services.
From 1982 onwards I kept looking at breastfeeding reports with an equity lens, only to find that inequalities, when sought, were found everywhere, irrespective of the equity stratifiers used. For example, in my own country, Italy, the rates of initiation, exclusivity, and duration of breastfeeding are lower in the south and among less educated mothers. 5 The same north to south gradient, and probably the same gradient by maternal education, can be observed across Europe, although with an upward trend.6,7 In the United States, there are wide variations in initiation and duration of breastfeeding among states. Western and northwestern states show the highest rates, with adjusted odds of not being breastfed 2.5–5.15 times greater in southern states and about three times greater in some New England states compared with Oregon. 8 Sociodemographic factors (e.g., family structure, poverty level) and maternal characteristics (e.g., language spoken, health and mental status) and behaviors (e.g., smoking, exercise) account for only 25–30% of these state variations. The absence of legislation for the promotion and support of breastfeeding probably accounts for part of the remaining variation, as infants living in states without such legislation show higher odds of not being breastfed after birth and for at least 6 months compared with those living in states with legislation. Other factors (e.g., hospital and community health practices, availability of lactation consultants and/or peer support, access to lactation rooms, and mandatory breastfeeding breaks in workplaces) may account for residual variation among states.
Moving to developing countries, in Africa, Asia, and Latin America only 47–57% of infants younger than 2 months are exclusively breastfed; for infants 2–5 months of age this percentage falls to 25–31%. 9 Figure 2 shows that in most developing countries less than 50% of infants younger than 6 months were exclusively breastfed between 2005 and 2009. The data are compiled by UNICEF using as sources Multiple Indicators Cluster Surveys, Demographic and Health Surveys, and other national surveys. 10 Although progress is reported by many countries in all regions, disparities among countries are evident.
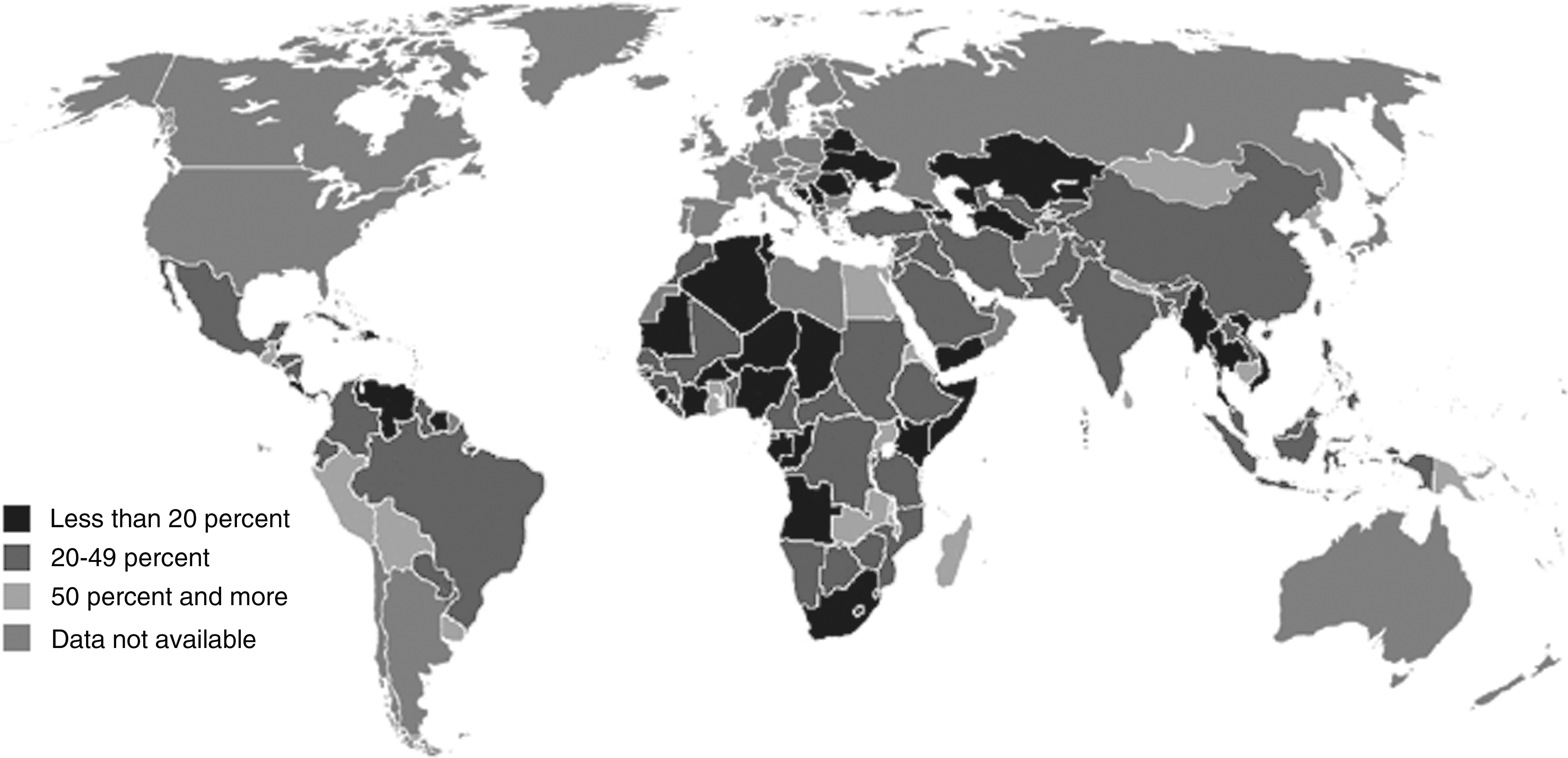
Percentage of infants under the age of 6 months who are exclusively breastfed, 2005–2009. 10
Disparities are present also within countries, irrespective of the equity stratifiers used. In Bangladesh, for example, where the rate of initiation of breastfeeding is 98%, with little geographical variation, the percentage of infants who receive colostrum is 96.6% when the mother has completed secondary or higher education but goes down to 87.3% when the mother has no formal education. The latter group of mothers is also more likely (65.2% vs. 56.4%) to give newborn babies all sorts of prelacteal feeds: Sugar or glucose water, milk, honey, plain water, or infant formula. 11 In Nicaragua, in 2001, the median duration of breastfeeding among mothers with higher, secondary, primary (4–6 years), primary (1–3 years), and no education was 9.4, 14.7, 17.3, 19.4, and 20.2 months, respectively. 12 In Mozambique, in 2003, 24.6% of infants less than 6 months of age living in urban areas were exclusively breastfed, compared with 32.1% of those living in rural areas. 13 Wealth is a common equity stratifier. Figure 3 shows the rates of exclusive breastfeeding and bottle feeding in infants 0–3 months of age by wealth quintile in different regions of the world; the data come from Demographic and Health Surveys carried out in 50 countries between 1990 and 2005. 14 The variation across regions is clear, as well as the fact that the rates of exclusive breastfeeding are higher in families with lower income, whereas those of bottle feeding are lower in the same families and higher in the upper wealth quintiles. In industrialized countries the opposite is usually observed (i.e., rates of breastfeeding are higher and rates of bottle feeding are lower in families from richer wealth quintiles).
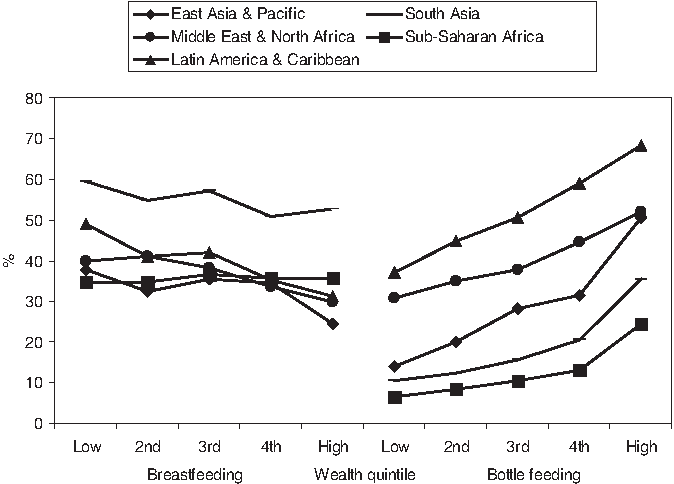
Prevalence of exclusive breastfeeding and bottle feeding in infants 0–3 months of age by wealth quintile. Drawn from data published in Gwatkin et al. 14
Inequities
In countries at all levels of income, health and illness follow a social gradient: the lower the socioeconomic position, the worse the health. It does not have to be this way and it is not right that it should be like this. Where systematic differences in health are judged to be avoidable by reasonable action they are, quite simply, unfair. It is this that we label health inequity. Putting right these inequities—the huge and remediable differences in health between and within countries—is a matter of social justice. Reducing health inequities is, for the Commission on Social Determinants of Health, an ethical imperative. Social injustice is killing people on a grand scale. 2
Which, among the differences, or inequalities, discussed in the previous section, do we judge as avoidable by reasonable action, or unfair? One may argue that living in a rural as opposed to an urban area, or in Oregon as opposed to a southern state, is not unfair; certainly it is not avoidable by reasonable action. Or that giving women more opportunities to increase their income by integrating them into the workforce is just and fair, in spite of its potentially negative effect on the exclusivity and duration of breastfeeding. Better education for women, as well as a more equitable distribution of wealth, can certainly be achieved by specific policies implemented by motivated local and national governments, as shown, for example, by the differences between the south and north of Italy, 15 or between Italy and Denmark in terms of equality score. 16 Whether such a reasonable action can be easily implemented is a matter of debate; also, one cannot expect rapid changes in these fields. It is certainly unfair that some mothers live in states or countries with no policies or legislation for the promotion and support of breastfeeding, because the development, implementation and enforcement of policies, laws, and regulations can be considered reasonable actions.
Finally, the WHO Commission on Social Determinants of Health includes health systems and services among the social determinants of health, as they can create, amplify, or mitigate health inequities—for example, through financing mechanism or discriminatory practices. 2 In our case, even if a mother is poor or less educated, lives in a rural area or in a state without a favorable legislation, works far from home, or belongs to a minority group, the lack of, or inadequate access to, effective support for the initiation, exclusivity, and duration of breastfeeding represents an inequity. As health professionals, we may feel unable to tackle the inequities associated with some social determinants of health such as legislation, education, or the distribution of wealth. As citizens, however, we should consider the redress of these factors as an ethical imperative. Moreover, as health professionals we are directly involved in the distribution of health care in our state, country, or community. If we do not act to remove all obstacles to universal access to good quality support for proper initiation, exclusivity, and duration of breastfeeding, we are failing to fulfil our professional obligations and are responsible for inequities.
Action
Several systematic reviews provide health professionals with inventories of interventions shown to be effective in improving the rates of breastfeeding. These reviews span from interventions at primary care level17,18 or in neonatal units 19 to interventions to promote the initiation of breastfeeding and/or its duration,20–22 based on professional and/or peer support.23,24 There are reviews about what mothers perceive and experience as effective support25,26 and on the effectiveness of mass media campaigns. 27 There are several Cochrane Reviews, on methods of milk expression, 28 on cup versus other ways of feeding, 29 on avoidance of bottles in preterm infants, 30 on the use of pacifiers, 31 and on support for breastfeeding mothers. 32 There are also overviews of reviews. 33 There is certainly no dearth of evidence-based literature.
All these interventions are usually grouped into three categories: protection, promotion, and support of breastfeeding. How can we give priority to interventions more likely to reduce inequities? I will discuss the three categories in inverse order.
Support
All the so-called Baby-Friendly Initiatives (BFIs), in hospitals, communities, neonatal intensive care units, medical schools, pharmacies, and so on, include elements of support. Some support is needed during pregnancy, more at childbirth, and much more after discharge from the maternity unit and until breastfeeding is firmly established. Support is mostly provided by health professionals, increasingly by peer counselors with some training, and by lay people such as doulas, fathers, and members of mother-to-mother support groups. Breastfeeding support, if timely and of good quality, is highly effective, as shown by many of the systematic reviews cited above. To deprive women and mothers of effective breastfeeding support is irrational and, in my opinion, unethical. Yet many women and mothers are deprived. Some get support, but mistimed and/or of low quality (i.e., ineffective). Some get no support at all, either because they do not look for it or because they do not have access to providers of support. Obstacles to access may be of various types (e.g., cultural, economical, geographical), but mostly amenable to the way health systems and healthcare services are built and organized. This is tantamount to saying that whenever a woman is totally or partially deprived of timely and effective support, it is our fault. Needless to say, this deprivation is more likely to occur to women from disadvantaged groups. Breastfeeding support can help reduce inequities only if it is actively offered to disadvantaged women and communities more than to the general population. This rule is indeed true for all types of healthcare services. 34 Increasing the amount of support and improving its quality, without an equity lens, are likely to increase inequities, at least initially. 35
Promotion
All the interventions that include some form of individual, group, or mass information, education, communication, advocacy, and social marketing belong to this category. Promotion includes activities directed to the general population or to specific groups, including health professionals. The development and dissemination of policies, recommendations, guidelines, and all sorts of training and communication tools are part of the promotion of breastfeeding. All the BFIs include elements of promotion. Many interventions in this category have evidence of effectiveness, some do not; for example, the use of an information booklet alone, without some kind of support, has been shown to be ineffective as far as duration and prevalence of breastfeeding at 6 months are concerned. 36 All promotion activities entail one or more senders and one or more recipients. Assuming the senders use effective tools and carry out their job well, the effect of promotion will depend on recipients. If recipients do not get the message, or get it wrong or incomplete, the effect will be null or partial. As for support, the likelihood of not getting the right message, or of getting it wrong or incomplete, is higher among disadvantaged women and mothers. Like support, promotion may actually increase inequities, at least initially, if it is not applied with an equity lens. Better-off and more educated women and mothers will get the message and will apply it earlier compared with the worse-off and less educated ones.
Protection
Protective interventions include the implementation and enforcement of the International Code of Marketing of Breastmilk Substitutes and subsequent relevant World Health Assembly resolutions, as well as legislation, regulations, and policies to remove obstacles and barriers to good-quality breastfeeding support, to protect women and mothers in the workforce, and to eliminate obstacles and barriers to breastfeeding anywhere, anyhow, and anytime mothers want. Some components of these protective interventions have evidence of effectiveness; for example, the handing out of commercial hospital discharge packs, with or without infant formula, which is forbidden by the International Code, appears to reduce the number of women exclusively breastfeeding at all times. 37 For most protective interventions, however, we do not have and we shall never have full evidence of effectiveness as intended by modern evidence-based medicine, for the simple reasons that it is very difficult, if not impossible, to submit legislation, regulations, and policies to controlled, let alone randomized, trials. Yet we all know that these interventions are effective because there is some indirect evidence; for example, countries with good enforcement of the International Code fare better in terms of breastfeeding rates than countries with poor or no enforcement, 38 as do countries with longer maternity leave and better legislation to protect and support mothers in the workforce who breastfeed. 39 Another type of indirect evidence is how strongly the baby food industry resists to any form of control; its huge investments in marketing strategies that circumvent the International Code and national legislation is indirect evidence that the latter are effective. Contrary to support and promotion, protection of breastfeeding applies to all women and is less dependent on take up by the target population. If well designed and enforced, protective interventions contribute to reducing inequalities and inequities. 40 Also, evidence-based promotion and support are less effective if implemented without protection.
Conclusions
The evidence presented above points to the existence of extensive social inequities as far as breastfeeding rates and practices are concerned. Action to reduce these inequities and their root causes is imperative; to refrain from such action is unethical. The development and implementation of policies and strategies for the protection, promotion, and support of breastfeeding that make use of an equity lens are urgent matters. To make sure that no segment of the population is excluded or loses out, protective interventions should have the priority, followed by promotion and support interventions that target disadvantaged women and communities, putting the last first in all policies and strategies.41,42 These policies and strategies should include the following: Progressive taxation to secure adequate public funds that are allocated according to need and regardless of ability to pay; a reduction of the burden of payment for low income groups, which usually have the highest need for care; procedures for monitoring inequities within the healthcare system and reporting the results to health professionals and policy makers, but also to the public; explicit equity-oriented objectives and targets; and finally, policies aimed at tackling the underlying social determinants of poor breastfeeding rates and practices.
Footnotes
Disclosure Statement
No competing financial interests exist.