
Abstract

Dear Editor:
I
Using a cross-sectional design we recruited neonates born at Royal Prince Alfred Hospital, Sydney, Australia, between September and October 2010. Eligible subjects were well, term, singleton neonates (37–42 weeks of gestation) within the first 48 hours of birth. Exclusions included neonates with major congenital abnormalities, multiple births, preterm neonates, and admissions to the neonatal intensive care unit for greater than 48 hours as illness or invasive monitoring prevented access. The breastfeeding data were extracted from the maternal medical record. We developed an objective composite measurement to identify neonates who had poor breastfeeding up to 3 days postpartum. Breastfeeding was coded according to a scale ranging from 1 to 6, where 1 was “breast offered but does not attach” to 6 defined as “long feed with good nutritive sucking.” A score by midwives of less than 4 conservatively estimated problems with breastfeeding. The timing of all breastfeeds was recorded by the in-charge midwife in the medical record. The first successful feed was calculated as the difference in time between the first feed that included a code scale of 5 and above and the time of delivery. Unsuccessful breastfeeding was defined as having at least two of the following three criteria: (1) frequency (fewer than three breastfeeds in the first 24 hours and fewer than six in the next 24 hours); (2) poor breastfeeding (or bottle feeding) codes (code of <4 occurring three or more times); and (3) expressed breastmilk or additional formula (more than twice). Rate ratios were estimated comparing poor breastfeeding versus “normal” for each timing category. We choose ≤1 hour initiation of breastfeeding as the reference group based on current literature and breastfeeding practice. 1 The other timing categories included 1–2 hours, 2–4 hours, and >4 hours. Prior to the study, Royal Prince Alfred Hospital was assessed for Baby Friendly Health Initiative status and was accredited following the study.
Five hundred eighty-one neonates were enrolled, with 75% recruitment. Of the 581 neonates, 97% initiated breastfeeding; 82% were exclusively breastfed, and 16% were predominately breastfed at discharge. As per our definition, 21% were defined as unsuccessfully breastfeeding after birth. The timing of the first breastfeed was assessed using ≤1 hour as the referent group and associated breastfeeding difficulty based on the three criteria. Initiating breastfeeding after 1–2 hours, compared with within 1 hour, had a rate ratio for poor feeding of 2.39 (95% confidence interval 1.54, 3.70; p<0.001). Similarly, initiation of breastfeeding after 2–4 hours had a rate ratio of 3.75 (95% confidence interval 2.38, 5.92; p<0.001) and >4 hours of 5.59 (95% confidence interval 3.27, 9.72; p<0.001). Figure 1 shows the rate ratios by timing of first feed and demonstrates the increasing rate of poor feeding with increasing delay to the first feed. To determine associated factors with breastfeeding difficulties, we conducted logistic regression including potential confounding factors such as delivery type, maternal ethnicity, age, body mass index, education, parity, and smoking status; any maternal illness including diabetes, gestational diabetes, gestational hypertension, pre-eclampsia, and eclampsia; and infant neonatal intensive care unit admission (<48 hours), body fat percentage as a measure of undernutrition using air displacement plethysomography, 3 gestational age, and sex. After an adjusted analysis including all the potential confounders regardless of significance, we found the predictors of breastfeeding difficulties included primiparity (p<0.001), emergency cesarean delivery (p=0.04), and elective cesarean delivery (p=0.02). When stratified by delivery type and parity the risk remained (Fig. 1). In contrast, neonatal undernutrition as measured by air displacement plethysomography was not a significant predictor.
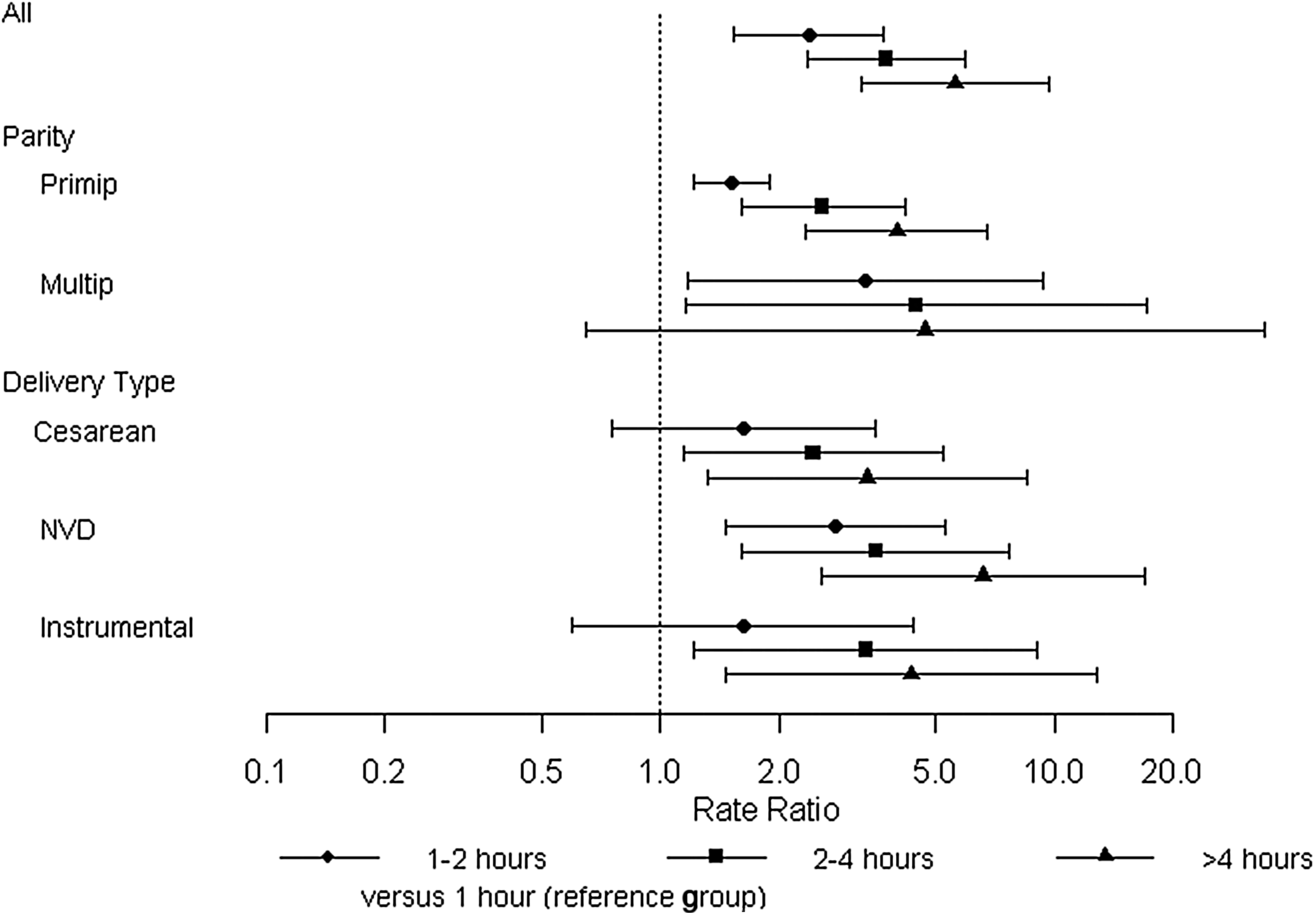
Rate ratios by timing of first feed for all women and stratified by parity and delivery demonstrating the increasing rate of poor feeding with increased interval to the first feed. Multip, multiparous; NVD, normal vaginal delivery; Primip, primiparous.
Our study is limited by the short investigation period, which may have missed breastfeeding difficulties that occurred after hospital discharge. Furthermore, the study was cross-sectional in design and did not allow for longer follow-up of breastfeeding duration and/or quality post-discharge. In addition, our study may be limited by neonatal conditions that prevent earlier hospital discharge; however, it is unlikely that these would impact our findings as adjustment for neonatal intensive care unit admission of <48 hours did not confound our results.
Our findings are compelling; for each hour that elapses before breastfeeding is initiated, there is a marked increased risk of breastfeeding difficulties following birth. In particular, our analysis highlights the need to focus on establishing appropriate breastfeeding within the first hour to prevent early feeding problems, especially for women who are first-time mothers and have had a cesarean birth. The management of first-time mothers and cesarean deliveries differs by and within countries. In particular, at a hospital level there is a growing demand for early discharge post-cesarean section 1–2 days following birth. Cesarean deliveries do not necessarily prevent early initiation of breastfeeding; rather, it is the processes around it. Thus, these results highlight that systems need adjusting to support breastfeeding immediately following cesarean section deliveries.
A recent systematic review and meta-analysis has shown that although skin-to-skin contact and early breastfeeding are associated with better breastfeeding outcomes at 1–4 months, the reason behind this is unclear, with inadequate evidence surrounding the exact timing of initiation, dose of skin-to skin contact, and technique. 4 We believe that our findings highlight that early successful breastfeeding, particularly initiation within the first hour, may explain why overall breastfeeding duration is improved. It is important that undernutrition is not a limiting factor to success. This study needs further investigation, and our future work will include long-term follow-up particularly focusing on the developing world.