
Abstract
Abstract
Objectives:
Breastfeeding is accepted as the healthiest practice for human immunodeficiency virus (HIV)-infected infants, but decisions about infant feeding are made before the child's HIV status is known. We examined the feasibility of counseling to support breastfeeding for newly diagnosed HIV-infected infants, including relactation for those who had never initiated or who had stopped breastfeeding before the infant's HIV status was known.
Materials and Methods
Results:
Mother–infant pairs (19 of the original 30) were followed up for 24 weeks. Ten of 19 women (53%) reported some breastfeeding at enrollment, two had stopped, and seven had never breastfed. At 24 weeks post-enrollment, 11 of 19 (58%) were providing breastmilk for all milk feeds. All women produced milk and provided some breastfeeds during the initial weeks of the study, but eight reported difficulty overcoming infant latching problems and stopped all breastfeeding. Attitudes toward breastfeeding were positive at the outset but became more negative in those who did not establish or sustain breastfeeding. Three of the seven who had never breastfed before enrollment into the study were fully breastfeeding at 24 weeks post-enrollment.
Conclusions:
Support for breastfeeding and relactation is possible among mothers of newly diagnosed HIV-infected infants but requires motivation from mothers and clinicians. Lactation counseling at the time of infant diagnosis is challenging as other issues predominate at this time. Improvements in antenatal infant feeding counseling are essential.
Introduction
T
For women either who never initiated breastfeeding or who stopped breastfeeding before learning their infant's HIV status, relactation would be a way of giving the vulnerable HIV-infected infant the well-established benefits of optimal nutrition and immunological support provided by human milk. Relactation is defined as the initiation of lactation at a time unrelated to postpartum milk production.4–9 Relactation has been reported in nonbiological mothers of adopted children in many cultures and settings around the world.10–13 One of the earliest reports is from South Africa noting the practice of older women taking up breastfeeding of their grandchildren. 14 Support for relactation has also been incorporated into nutrition rehabilitation programs for young children who have been weaned15–17 and has been part of programs to support women with lactation difficulties or early weaning.18–21 Relactation has been supported in the context of transitioning preterm infants to independent feeding.22–24 Counseling programs to assist women achieve relactation have been developed by lactation experts. 6
In this study, we investigated the feasibility of supporting breastfeeding, including relactation, for HIV-infected mothers of HIV-infected infants diagnosed at a young age. At the time the study was conducted, initiation of breastfeeding among HIV-infected women was thought to be uncommon at our clinical site.
Materials and Methods
Study population
A pilot study was conducted to examine the feasibility of supporting breastfeeding, including relactation, among HIV-infected women and their HIV-infected infants. Mothers of newly diagnosed HIV-infected infants under 14 weeks of age identified as part of early infant diagnosis services at the Perinatal HIV Research Unit at Chris Hani Baragwanath Hospital in Soweto, South Africa, were approached about possible enrollment into the study. The early infant diagnosis program offered routine testing of all infants born to HIV-infected women at 6 weeks of age as follow-up of prevention of mother-to-child HIV transmission (PMTCT) services. Inclusion criteria were infant age <14 weeks, willingness to participate in a study that supported breastfeeding, and planning to remain in the area for the next 6 months. Exclusion criteria were maternal body mass index (BMI) of<18.5 kg/m2, CD4 count of <50 cells, or being too weak to attempt to breastfeed and infant weight of <1.5 kg. No exclusions based on current infant feeding practices were made to avoid inadvertent incentives for providing incorrect information about feeding practices. We approached 116 women having newly diagnosed HIV-infected infants within the age range before reaching the target sample size of 30 mother–infant pairs who were enrolled between September 2008 and May 2010. The study was approved by the Human Research Ethics Committee of the University of the Witwatersrand, and all women provided written informed consent for their participation.
Study design
All mothers were offered lactation counseling. Support for breastfeeding initiation or for re-establishing breastfeeding was provided to those who had not established any breastfeeding or who had stopped prior to enrollment. Data on feeding practices were collected at enrollment, and then mother–infant pairs were followed up for 24 weeks with intensive counseling, evaluation of feeding practices and attitudes, and assessments of maternal and infant morbidity and infant growth. All infants were started on antiretroviral therapy as well as mothers who met local standard of care for initiating therapy.
Study context
At the time the study was done, most HIV-infected women who made use of the services at the study site chose to feed their infants formula. Free infant formula was provided as part of the PMTCT program. Antenatal infant feeding counseling was designed to follow WHO guidelines in place at the time that emphasized individualized informed choice and supporting formula feeding to avoid HIV transmission if social and economic characteristics of an individual woman made formula feeding affordable, feasible, acceptable, sustainable, and safe. Adult antiretroviral therapy was available in the public sector but was generally restricted to persons with CD4 counts of <200 cells. PMTCT programs attempted to ensure that pregnant women meeting treatment criteria initiate antiretroviral therapy. For pregnant women not meeting treatment eligibility criteria, PMTCT guidelines supported zidovudine started at 28 weeks of gestation, and single-dose nevirapine was given at the onset of labor. Toward the end of 2009, guidelines shifted to WHO-recommended Option A, which included, for the first time, extended use of nevirapine prophylaxis to the infant during the breastfeeding period and greater support of breastfeeding for HIV-infected women. Antiretroviral therapy was recommended for all HIV-infected infants regardless of clinical or immunological criteria and for women with CD4 counts of ≤350 cells or advanced clinical disease.
Study intervention
A clinic-based counseling program was developed to provide lactation support for HIV-infected mothers of HIV-infected infants, including support around breastfeeding initiation for those who had not attempted to establish any breastfeeding or who had stopped prior to enrollment. A training program was developed for the study team, which included a physician, nurse–midwife, and counselor. The training program was developed by two experienced local lactation consultants and consisted of a 2-day workshop, in-service counseling training over a period of 4 weeks, and individual mentoring for the study team over the course of the study. The 2-day workshop included information about the physiology of lactation and other aspects of lactation support following standard curricula recommended by La Leche League International, the International Board of Lactation Consultants, and the WHO. Specific input on HIV-related issues was also provided by the HIV researchers on the team.
Intensive individual support and counseling were provided to the mothers enrolled in the study by the study physician, nurse, and counselor. Information was provided about the possibility of re-establishing breastfeeding and the physiological mechanisms involved. The benefits of breastfeeding were discussed as well as the practical steps to achieve full lactation. The team attempted to correct misinformation about breastfeeding and HIV as well as to provide reassurance and support around strengthening breastfeeding. Lactation-inducing drugs were not encouraged. The frequency of the counseling was weekly in the first 4 weeks, every 2 weeks in the next 8 weeks, and then every 4 weeks for 24 weeks after enrollment.
Data collection
At enrollment, data on socioeconomic parameters were collected, and breastfeeding history was examined. Questions were asked about whether the child had ever been breastfed, when any breastmilk exposures had ended, and the frequency of breastmilk and other feedings. Over the course of the 24 weeks of follow-up, feeding practices and attitudes were closely monitored. Each mother was supplied with a feeding diary to record amount of formula milk and/or breastmilk given to her infant. The mother was asked to fill in the diary each time she fed her infant, as well as recording the presence of urine or stools after each diaper change. During the study visit, these diaries were reviewed, and specific questions were asked about feeding frequencies, experiences, and attitudes. At each visit, women were asked whether they felt more positive, less positive, or the same about relactation to ascertain their attitudes toward infant feeding. Open-ended questions were asked about what had been satisfying and challenging about relactation and supportiveness of partners and family. At each visit, mothers and infants were weighed, and infants' lengths were recorded. Weight-for-age Z-score adjusted for sex was calculated by using WHO growth standards. 25 Episodes of illness in either mother or infant were recorded. Blood samples were drawn from infants at enrollment and at 3 months and 6 months post-enrollment and from mothers at enrollment and 6 months to measure CD4 count and plasma viral load. Breastmilk was pumped for exactly 5 minutes, and the amount of milk produced was measured at each visit. Observation of infant positioning and attachment during breastfeeding was done on every visit. Mothers were considered to have established full lactation if infants were given 100% of total milk intake by breastfeeding at 24 weeks.
Statistical methods
Student's t test and nonparametric Wilcoxon tests were used for continuous variables, and Pearson's chi-squared statistics and Fisher's exact test were used for categorical variables. Generalized estimating equation models were used to compare groups when covariates were measured at repeat follow-up visits. Growth was plotted over time using a moving average. Statistical analysis was conducted using SAS software (SAS Institute, Cary, NC).
Results
Cohort description
Of 116 women approached, 17 did not meet eligibility criteria (nine infants were >14 weeks, one infant was a twin, one infant was found to be polymerase chain reaction negative, one mother died, three mothers had CD4 counts of <50, one infant had a birth weight of <1.5 kg, and one infant had been abandoned by his biological mother), and 69 declined to enroll; 30 (25.9%) were enrolled into the study. The most commonly cited reasons for declining to participate was the need to return to work or to school (n=22), not wanting to breastfeed (n=14), being afraid of re-infecting their infants (n=10), or planning to relocate (n=9). Others were not interested in participating (n=7) or reported that fathers refused maternal breastfeeding (n=3), that they had taken breastmilk suppressants (n=2), that they were living separately from the infant (n=1), or disclosure concerns (n=1). The study team identified maternal psychological distress around the time of infant diagnosis and the high burden of visits required for initiation of infant antiretroviral therapy as further barriers to enrollment. Of the 30 women enrolled, one woman did not meet eligibility criteria (CD4 count <50) and was retrospectively withdrawn. One infant died, and five women were lost to follow-up. Four women withdrew from the study because infants were hospitalized (n=2) or mothers were relocating to other places (n=2). Follow-up to 24 weeks was completed for 19 of 29 mother–infant pairs. Clinical and socioeconomic factors as well as initial feeding practices were not significantly different between those who were followed up (n=19) compared with those who did not complete the study (n=10) (Table 1).
BMI, body mass index; Q, quartile; SD, standard deviation.
Establishment of full lactation
Among the 19 mother–infant pairs followed to study end, infants were on average 63 days of age (range, 37–92 days) when enrolled. At enrollment, 10 of the 19 (52.6%) women reported currently breastfeeding, seven (36.8%) reported never having breastfed the child, one (5.3%) had breastfed for less than 1 week, and one (5.3%) reported having stopped before enrollment. Six of the 10 women who were breastfeeding at enrollment were exclusively breastfeeding at this time.
At 24 weeks post-enrollment, 11 (58%) women were fully breastfeeding their infants (i.e., giving 100% of the milk feeds by breastmilk). None of the 11 was exclusively breastfeeding at this time, but all of the infants were older than 24 weeks of age at the time (average age at the end of the study, 34 weeks; range, 29–39 weeks). All women could produce milk during the initial weeks of the study. The eight women who did not establish full lactation by 24 weeks post-enrollment were able to produce breastmilk during the initial weeks of the study, reported some breastfeeding during this time, but reported difficulty overcoming infant latching problems, which they attributed to insufficient milk production.
Those who achieved full lactation by the end of the study did not differ in baseline clinical and sociodemographic factors from those not breastfeeding at study end (Table 1). Of the 10 women reporting some breastfeeding at enrollment, eight were fully breastfeeding at 24 weeks. Of seven women who reported never having breastfed, three were able to achieve full lactation by the end of the study: two by the week 1 visit and one by the week 3 study visit. The two women who had stopped breastfeeding before enrollment, although able to produce breastmilk and re-establishing some breastfeeding, did not sustain breastfeeding to 24 weeks post-enrollment.
All 11 women who were fully breastfeeding 24 weeks after enrollment and seven of eight women who did not establish or persist with lactation were producing milk at the time of enrollment. Women who were fully breastfeeding at the end of the study produced significantly higher volumes of breastmilk over the course of follow-up than those who were not as measured during 5 minutes of pumping (24.7±17.3 mL versus 3.3±5.7 mL; p<0.0001). Those who did not establish lactation initially produced milk, and almost half were able to give 100% of the total milk intake by breastfeeding by the week 4 clinic visit, but this declined thereafter.
As recommended by the counseling to stimulate milk production, mothers who did not establish or maintain lactation expressed breastmilk more frequently than mothers who established lactation (45.2% of study visits versus 8.2%; p=0.036). The three women who had never breastfed before the study but who successfully established relactation produced a higher volume of breastmilk at the first clinic visit than those who did not establish breastfeeding through 24 weeks.
Several factors associated with breastfeeding practice significantly differed among women who established lactation and those who did not (Table 2). When the infant's positioning and attachment to the breast/nipple were evaluated at each study visit, infants who were not fully breastfed at the end of the study were breastfed in a manner defined as correct and effective by the study team's observations for only 68.3% (28/41) of study visits versus 97.9% (95/97) among those who successfully established lactation (p=0.07). Also, although for 91.8% of study visits women who established lactation put the infant to the breast even when the infant did not need to feed, those who did not establish lactation did so only for 34.3% of study visits (p=0.0001). The average reported suckling time differed between the two groups (8.2 minutes among women who established lactation versus 13.8 minutes among who did not; p=0.25). Among the three women who had never breastfed their infants before enrollment but who relactated, the mean reported suckling time of the infants was 17.2 (±6.6) minutes, and the mothers put infants to the breast even when they did not need to feed for 27 of 28 study visits (96.4%).
p value was calculated from generalized estimating equation models taking into account multiple measurements on the same child.
Limited to study visits when mothers reported giving >0% of total milk intake as breastfeeding.
NA, not applicable; SD, standard deviation.
Clinical outcomes
Maternal and infant clinical outcomes up to 24 weeks are shown in Table 3. There was no evidence of harm to mothers by establishing or continuing breastfeeding. The changes in maternal CD4 counts and plasma viral load between enrollment and 6 months were similar among women who were fully breastfeeding at study end versus those who were not. Change in maternal BMI also did not differ between the groups. There was a nonsignificant trend for women who established breastfeeding to have a slightly better CD4 and viral load profile at enrollment and to more likely to be of normal BMI, with an average overweight BMI in those women who did not establish breastfeeding. Occurrence of breast problems was rare. There were only two reports of breast problems: one report of mastitis and one of sore nipples. These symptoms resolved, and both occurred in the group of the mothers who established breastfeeding.
No mothers were on antiretroviral therapy at enrollment.
One mother in the not breastfeeding and two mothers in the breastfeeding groups were receiving antiretroviral therapy by the end of the study. All three had <50 copies/mL.
No infants were receiving antiretroviral therapy at enrollment, but all were receiving it by 3 months.
BMI, body mass index; HIV, human immunodeficiency virus; Q, quartile; SD, standard deviation.
The CD4 percentage and plasma viral load at enrollment and at 3 months and 6 month were not significantly different among the infants who were fully breastfed at 24 weeks and those who were not. There was a nonsignificant trend toward better growth in those who were breastfed, but these appeared to be present prior to the study (Fig. 1). Of the three children who were not receiving any breastmilk at enrollment but subsequently were fully breastfed, there was a net improvement in growth (i.e., higher weight-for-age Z-scores) in all three infants (Fig. 2). The reported number of sick visits was slightly fewer in infants who were fully breastfed at study end (34.4%, 33/96 study visits) compared with those who were not (42.9%, 33/77 study visits), but the difference was not statistically significant (p=0.25). The most common reasons for sick visits of infants included body rash, cough, diarrhea, gastroenteritis, lower and upper respiratory tract infection, and nasal congestion.
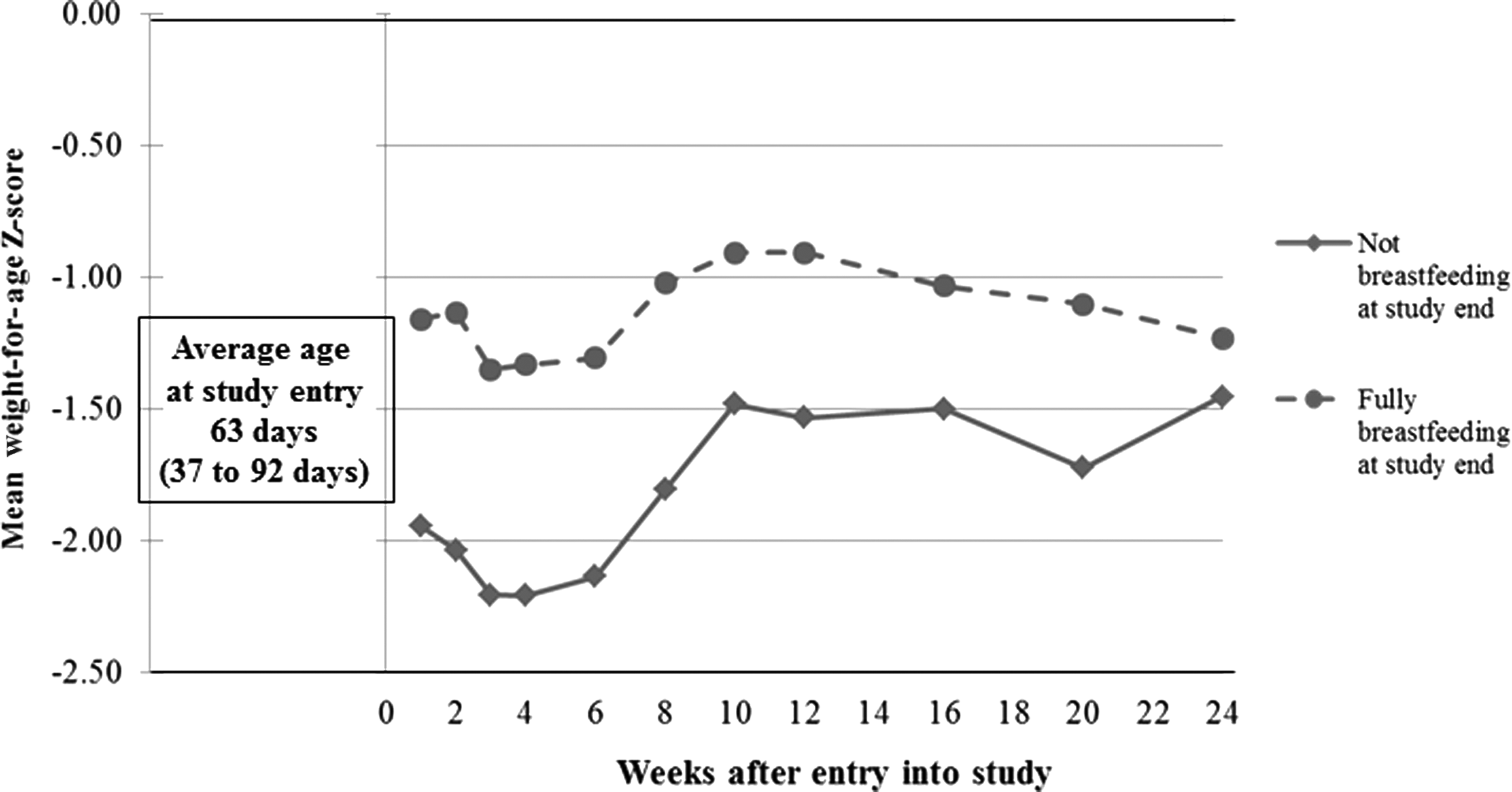
Mean infant weight-for-age Z-score (moving average) at each study visit stratified by whether or not breastfeeding was fully established by study end.

Actual weight-for-age Z-scores by infant age for the three infants who had never been breastfed before enrollment but who were fully breastfed at the end of the study. Each infant's weight-for-age Z-scores are represented by a different symbol.
Attitudes
At the time of enrollment, attitudes toward breastfeeding were universally positive, and mothers were confident and willing to breastfeed. During the study, mothers who established lactation remained positive and were satisfied with breastfeeding because (1) breastfeeding facilitated mother–infant bonding, (2) infants grew well and stayed healthy, (3) breastmilk was easily accessible and did not require preparation, and (4) the mother saved money. For similar reasons, most of the time family members supported breastfeeding except when mothers were sick or babies were not latching. Attitudes became more negative in those who did not establish breastfeeding. Women reported that they were discouraged in that even though they tried and were willing to breastfeed infants, infants refused to suckle, and there was not enough milk produced to feed the infants.
Discussion
Our study demonstrated that support for breastfeeding, including support for relactation, following infant HIV diagnosis could result in substantial improvement in breastfeeding practices, with about 60% providing all milk feeds via the breast by 24 weeks after enrollment. But, achievement of this outcome was challenging and required intensive one-on-one counseling. It was also difficult to enroll participants into this study, with more than two-thirds of the seemingly eligible participants not wishing to enroll in the study. Only a minority of those not wishing to join the study explicitly stated that they did not wish to breastfeed. However, potential participants were told the objectives of the study, and the most frequently reason given for not joining the study was having to return to work. The barriers of employment to breastfeed are well recognized and have been a focus of several breastfeeding advocacy campaigns. 26 Thus it is possible that the challenges we faced enrolling participants were in part due to reluctance of HIV-infected women in this community at that time to consider breastfeeding.
Fear of “re-infecting” the infant was also a fairly common reason provided by mothers to avoid breastfeeding. The idea that HIV-infected mothers may think that breastmilk might infect or “poison” their infants has been reported from other contexts. 27 The concern likely arises from educational messages that emphasize the risks of postnatal HIV transmission at the expense of explaining benefits of breastfeeding. Although “superinfection” has been described in some contexts, its frequency in the breastfed infant is unknown. 28 Given the well-established benefits of breastfeeding for HIV-infected children who continue to be exposed to virus-containing breastmilk, the adverse clinical consequences of superinfection, should it occur, appear to be negligible.
We were surprised at the frequency of breastfeeding at enrollment in the cohort (10 of 19 were still breastfeeding at the time of enrollment) at a site where we anticipated that uptake of breastfeeding would be low. This may reflect the selection factors that resulted in the small subset choosing to participate in the study and may not be representative of women at the site at that time. However, exclusive breastfeeding at the time of enrollment was rare, and many women were breastfeeding intermittently or had stopped and started breastfeeding without a clear commitment to either breastfeeding or avoiding breastfeeding. This pattern was most likely exacerbated by concerns about HIV transmission in the era prior to antiretrovirals being used during the postnatal transmission to prevent transmission. 29 Women may also have felt more comfortable to disclose their actual feeding practices in the nonjudgmental, confidential context of our study.
Greater breastfeeding prior to enrollment predicted sustained establishment of breastfeeding by the end of the study. Our study confirms the reversible nature of infant feeding decisions that has been carefully described before. 30 However, three women who had never breastfed their infants were able to gradually move to full breastfeeding by 24 weeks post-enrollment and can thus be considered exemplars of relactation in the strictest sense. Our findings of reasonable success with uptake of relactation are consistent with the literature.21,23 For example, in a prospective study of 139 mothers with complete lactation failure encouraged to breastfeed infants 10–12 times per day, over 80% successfully established relactation. 16 Similarly, in another study where mothers were randomized to receive lactagogues or not, 92% of mothers without lactagogues were able to relactate by 50 days of follow-up. 19 Relactation has not to our knowledge been previously reported among mothers of HIV-infected infants.
It appeared that nonrestricted access of the infant to the breast, longer suckling time, and correct positioning and attachment during feeding were the factors that allowed full breastfeeding to be achieved. All women could produce milk during the course of the study, but those who did not establish breastfeeding were unable to overcome infant latching difficulties to establish a sustained practice. Latching problems are commonly reported in the clinical literature due to various reasons, and overcoming them requires support from family members and counselors. 6
Infants fully breastfed at the end of the study had higher weight-for-age Z-scores at this time. However, these infants also had better weights at the start of the study, possibly reflecting their better breastfeeding practices initially. However, in the three infants not breastfeeding at enrollment but who relactated, there was a trajectory of improving weight-for-age Z-scores over time (Fig. 2), supporting the notion that breastfeeding in these HIV-infected infants was able to have some benefits for growth. There was no suggestion of any detriment of breastfeeding for the health of the mother and child, and all trends were in the direction favoring breastfeeding.
The study has several limitations. First, because this was a pilot feasibility study, only a small number of mother–infant pairs were recruited. Thus conventional hypothesis testing is somewhat uninformative about associations other than those that are large. Second, by necessity we relied on self-reported feeding behaviors. Although these may have been inaccurately reported, the close relationship with the study team and the frequency of contact make it unlikely that these reports are completely fabricated. Finally, our study was done largely before the changes to the infant feeding guidelines that now provide more support for breastfeeding for HIV-infected women and thus cannot be generalized to the now hopefully improved practices.
Despite these limitations, our data suggest that counseling HIV-infected women at the time of their infant's HIV diagnosis is a feasible opportunity to intervene to support breastfeeding and relactation. Most women can be supported to achieve full breastfeeding regardless of their prior practices if there is sufficient counseling and they are motivated. The time immediately after infant diagnosis is a challenging time for infant feeding counseling as several other issues require maternal attention at this time, including confronting the significance of having transmitted HIV to the infant and concerns about the health of the infant, as well as multiple health service visits for assessments and initiation of antiretroviral therapy.
Now that the current WHO recommendations encourage breastfeeding with infant and/or maternal antiretrovirals during the period of breastfeeding, it is important to improve antenatal, perinatal, and early postnatal infant feeding counseling for HIV-infected women. Improved initial counseling would allow later counseling for mothers of HIV-infected infants to be more effective. More research on how to support breastfeeding for HIV-infected infants in this setting is urgently needed.
Footnotes
Acknowledgments
We would like to thank Brenda Campbell and Brenda Pierce for assistance with the training and conduct of this study.
Disclosure Statement
No competing financial interests exist.
The study was designed by G.G., L.K., and M.N. M.N. recruited and counseled the study participants. Analysis was done by H.-Y.K. and L.K. All authors contributed to the writing and interpretation of the data.