
Abstract
Abstract
Background:
Fecal calprotectin (fCP) is a biomarker of gastrointestinal tract (GIT) inflammation that is currently being used investigationally among very low birth weight (VLBW) infants.
Materials and Methods:
Stool was collected weekly from 20 breastmilk-fed VLBW infants for up to 8 weeks after birth during the establishment and fortification of feeds, and fCP concentrations were measured.
Results:
Mean fCP levels increased significantly in stools collected immediately following bovine-based nutrient fortification of feeds (p = 0.005).
Conclusions:
Addition of bovine fortifier to breastmilk feeds appeared to be associated with an acute increase in GIT inflammation.
Introduction
C
Among infants, the clinical use of fCP remains investigational. High fCP concentrations have been observed in healthy term4,5 and preterm5–9 infants in the first weeks of life, including in meconium. 10 Reports suggest fCP is elevated in acute gastrointestinal events among very low birth weight (VLBW) infants such as necrotizing enterocolitis (NEC).6,7,11,12 Thus fCP has been proposed as a potential biomarker to aid in the early diagnosis of NEC.13,14 The pathogenesis of NEC is multifactorial, but the association between NEC in VLBW infants and cow's milk formula feeds is well established. 15 When VLBW infants are fed breastmilk, this milk is typically enriched with a multicomponent fortifier including bovine-based protein in order to meet the nutritional needs of such infants. There is emerging evidence to suggest a relationship between bovine-based nutrient fortifier and increased oxidative stress 16 as well as NEC among VLBW infants.17,18 Although the pathophysiology underlying NEC and formula feeds is not entirely elucidated, the ultimate pathway to injury is the initiation of an inflammatory cascade potentially resulting in devastating local and systemic effects. 19
The objective of this study was to assess the effect of bovine-based nutrient fortification of breastmilk feeds on GIT inflammation in VLBW infants by measuring fCP levels during the course of establishing feeds as well as before and after addition of fortifier.
Materials and Methods
VLBW infants admitted to the tertiary neonatal intensive care unit at Mount Sinai Hospital, Toronto, ON, Canada, between January and December 2012 were recruited. Eligible infants were birth weight of <1,500 g, <96 hours of age at enrollment, and expected to initiate feeds in the first 7 days of life. Infants were excluded if they had a major congenital or chromosomal anomaly or had severe asphyxia at birth. The study received Research Ethics Board approval, and written consent was obtained from parents.
Feeds were introduced and advanced by a standardized protocol based on birth weight that included sequential increases of 15–20 mL/kg/day of feed. Fortification commenced at 120–160 mL/kg/day of enteral feeds using powdered Similac® (Abbott Laboratories, Chicago, IL) human milk fortifier, followed by oral vitamin D and iron supplementation after fortification. Stool samples were collected weekly from the infants' diapers for up to 8 weeks and stored at −80°C until analysis. The fCP levels were measured using a commercially available calprotectin enzyme-linked immunosorbent assay (Calprest®; Eurospital Spa, Trieste, Italy).
Infants were included in the subsequent analyses if they received exclusive breastmilk feeds during the study period and had a complete stool collection series (six or more samples). Descriptive statistics were calculated for all variables of interest. A two-sided paired t test was used to compare first pre- and postfortification fCP values. A repeated-measure regression analysis was performed to compare fCP by postnatal day of life and week of life, including an adjustment for gestational age. All analyses were carried out using SAS version 9.1 software (SAS Institute, Cary, NC).
Results
Of 83 infants enrolled, 30 were exclusively breastmilk-fed, and 20 of these had six or more weeks of stool collected. The remaining 10 infants had incomplete stool collections, mainly due to transfer to a community hospital, and were not included. No deaths occurred among the infants.
The mean gestational age (± standard deviation) of the 20 included infants was 26.4 ± 1.7 weeks with a mean birth weight of 874 ± 181 g (Table 1). Ten infants were male, and nine were delivered via cesarean section. Three infants were born to mothers with chorioamnionitis, defined as a maternal temperature of >38°C at delivery, purulent liquor, or culture-positive placental swab. One infant whose mother had chorioamnionitis developed early-onset Escherichia coli sepsis with meningitis. None of the infants developed NEC or late-onset sepsis. Stool volume was inadequate for analysis in 10 meconium samples and three samples prefortification.
Data are mean ± standard deviation values unless indicated otherwise.
NEC, necrotizing enterocolitis.
The fCP concentrations are displayed by week of life in Figure 1. There was no association between fCP concentration and day of life (p = 0.54) or week of life (p = 0.57), even after adjustment for gestational age (p > 0.05).

Median, first and third quartile, and mean fecal calprotectin concentration by week of life among very low birth weight infants (n = 10–20 infants per week).
The differences in fCP levels pre- and postfortification were confirmed to be normally distributed using the Shapiro–Wilk test. There was a significant increase in mean fCP concentration in the first stool collected after (up to +6 days) fortification of feeds when compared with the last stool collected prior (up to −6 days) to fortification (317.8 ± 180.7 versus 145.2 ± 203.2 μg/g; p = 0.005) (Fig. 2). The number of infants born to mothers with active chorioamnionitis or with sepsis was too small for subgroup analysis.
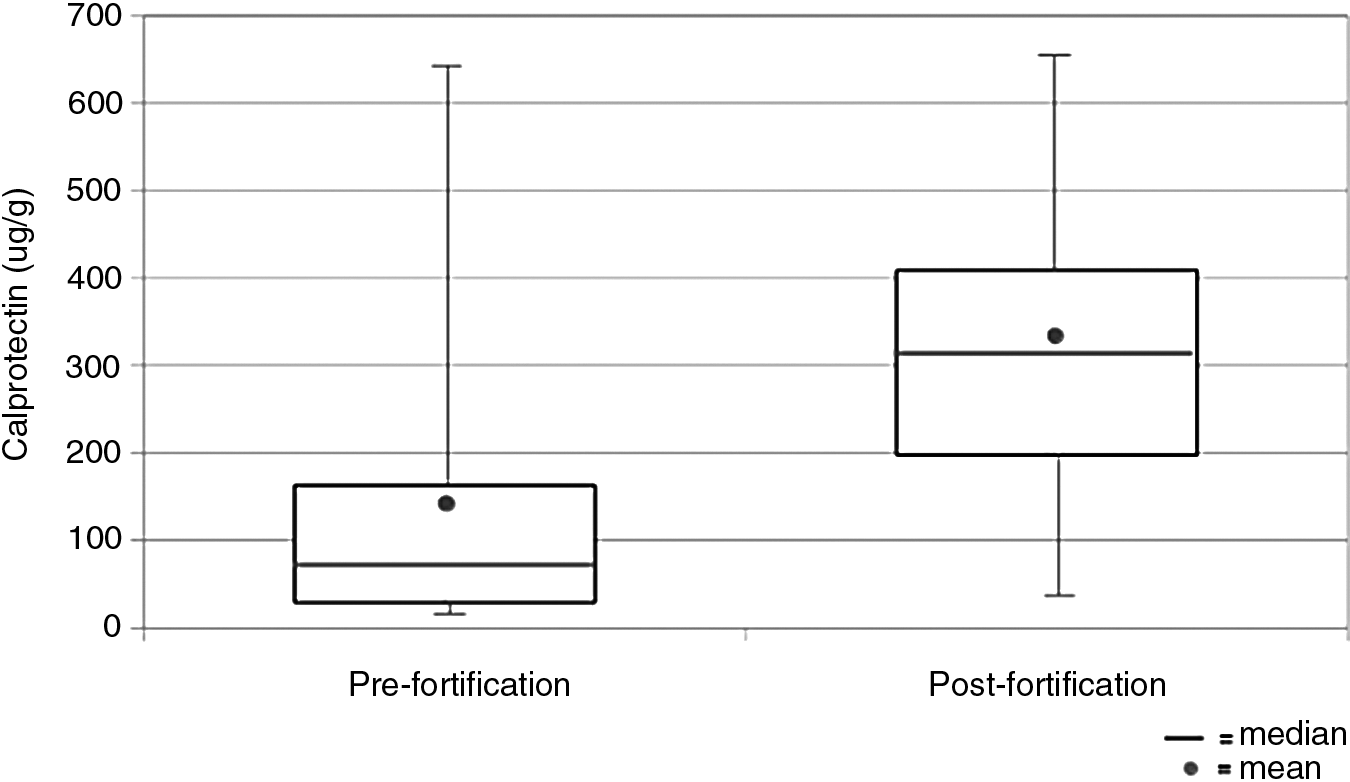
Median, first and third quartile, and mean fecal calprotectin concentrations among stools collected immediately prefortification (up to −6 days) (n = 17) and postfortification (up to +6 days) (n = 20) (p = 0.005).
Discussion
The main finding of our study was that mean fCP concentrations increased significantly in the first stool samples collected following nutrient fortification compared with those just prior to fortification, which may be indicative of increased GIT inflammation following fortification. It is interesting that the mean postfortification fCP level is above the threshold (180–210 μg/g) proposed by Zopelli et al. 14 to identify moderate NEC. Although none of the infants in our study developed NEC, we hypothesize the elevated fCP level postfortification suggests an acute inflammatory response among these infants following fortification. The etiology of the inflammation is unclear but may be related to antigenic exposure to cow's milk proteins, increased osmolarity of the fortified feeds, or, extrapolating from other physiologic changes that occur with formula feeds, altered GIT pH, decreased intestinal motility, fostered growth of pathogens, or other factors not yet understood following fortification.
It is also possible that other high-osmolarity agents, such as oral vitamin D or iron supplements, often temporally introduced around the same time as fortification, may have contributed to GIT inflammation and elevated fCP levels, as hyperosmolar feeds and medications have previously been implicated in contributing to NEC. 20 However, vitamin D and/or iron had been commenced prior to the postfortification stool collection in only five of the 17 infants who had samples included in the pre- and postfortification fCP comparison, and so this is unlikely to have contributed to the increase in fCP levels found.
Moreover, an in vitro study recently showed that digestion of bovine-based formula directly causes intestinal cell death via increased generation of cytotoxic free fatty acids but not breastmilk. 21
The days following bovine-based fortification may indeed represent a vulnerable pro-inflammatory period for VLBW infants with other risk factors for NEC.
The relationship between day of life or week of life and fCP in our study was not significant, although some of the highest fCP values observed were among stools collected in the first week of life. A trend of decreasing fCP level with increasing postnatal age and enteral feeds has been observed7,22; increased baseline fCP with decreased gestational age has also been reported. 14 The high fCP concentrations measured in VLBW infants particularly at birth are postulated to be due in part to the relative immaturity and permeability of the bowel of such infants, as well as potential inflammatory events, such as chorioamnionitis, that may surround their birth. 9 This maturational permeability could explain the relatively high fCP concentrations seen in the first week(s) of life that, coupled with potential GIT inflammation following fortification, then increased further postfortification in this study.
A limitation of this study is its small sample size, and this is likely why postnatal age-related effects were not significant. High intra- and interindividual variability in fCP concentrations was also observed, reflected in the large interquartile fCP values reported, and has been described among VLBW infants by others as well.8,9 As such, larger-scale studies are needed to establish reliable threshold ranges before this biomarker is accepted into wide clinical use in this population.
Conclusions
Addition of bovine-based nutrient fortifier to breastmilk appears to be associated with an acute increase in fCP level, which may reflect an increase in GIT inflammation among VLBW infants. Optimal nutrient fortification of breastmilk for VLBW infants requires further study. Calprotectin requires further investigation in this vulnerable population both as a promising research tool and as a clinical adjunct.
Footnotes
Acknowledgments
We wish to acknowledge Susanne Aufreiter for her laboratory assistance and Brock Williams for his contribution to data collection for the study. This work was funded by the Canadian Institutes of Health Research (MOP#125997) and the University of Toronto Post Graduate Medical Education Trainee Grant Program, including the Elizabeth Arbuthnot Dyson Fellowship and Joseph M. West Memorial Funds.
Disclosure Statement
No competing financial interests exist. Neither funding agency had a role in the design, execution, analysis, or write-up of this study.
J.K.P. wrote the first draft of this manuscript.