
Abstract
Abstract
Introduction:
Management of breast abscess in lactating women remains controversial. During pregnancy, women may develop different kinds of benign breast lesions that could require a surgical incision performed under general anesthesia with consequent breastfeeding interruption. The purpose of this study was to prospectively evaluate the management of large breast abscesses with ultrasound-assisted drainage aiming at breastfeeding preservation.
Materials and Methods:
34 lactating women with a diagnosis of unilateral breast abscess have been treated with an ultrasound (US)-assisted drainage of the abscess. A pigtail catheter was inserted into the fluid collection using the Seldinger technique under US guide and connected to a three stop way to allow drainage and irrigation of the cavity until its resolution.
Results:
All procedures have been found safe and well tolerated. No recurrence was observed and breastfeeding was never interrupted.
Conclusions:
The described technique allows to avoid surgery and to preserve breastfeeding in well-selected patients with a safe, well-tolerated and cost-effective procedure.
Introduction
L
The best management of breast abscesses is a controversial topic. In many institutions, the preferred treatment, especially when dealing with large fluid collections, remains surgical incision and drainage under general anesthesia with consequent breastfeeding interruption and prolonged healing time, with potential unsatisfactory aesthetic results, because of bad scarring and/or adherences. 2
In the past decade, different authors described successful ultrasound (US)-guided percutaneous treatment of breast abscesses, few focusing on lactating women.3–5
We present an alternative management of large breast abscesses in lactating women with US-assisted drainage aiming at breastfeeding preservation.
From March 2014 to May 2016, 34 lactating women who referred to our department with a diagnosis of breast abscess on the basis of the presence of a painful unilateral breast palpable lump or swelling, associated with fever or not, have been treated with an US-assisted drainage of the abscess. All enrolled patients underwent US examination to evaluate the feasibility of a percutaneous catheter-assisted drainage. Exclusion criteria were ultrasonographic evidence of mastitis without any appearance of a fluid collection, abscesses smaller than 3 cm in diameter, multiple separated cavities, age <18 years, patients unwilling to sign informed consent, and allergy to penicillins or local anesthetics.
The aspiration of pus or milk, as the first step of percutaneous catheter-assisted drainage, helped us in the differential diagnosis between breast abscesses and galactoceles.
We injected local anesthetics (10 cc of 2% lidocaine chlorhydrate) in healthy breast tissue about 2 cm from the abscess to perform a 5 mm skin incision enabling catheter insertion (8 French × 25 cm, Hospital Service S.p.A., Aprilia, Italy). US-guided percutaneous drainage was then performed using the Seldinger technique (Fig. 1). While inserting the cranial part of the catheter into the cavity, the opposite end was connected to a three stop way, thus providing two more accesses, the first to be connected to a drainage bag and the second to be used for irrigation. Irrigation started immediately after complete abscess drainage. We washed the cavity three to five times with sterile saline. At the end of the procedure, the catheter was anchored to the skin. Every 2 days after the procedure, patients were called back to perform saline irrigations and US assessment of the residual cavity. The catheter was usually removed when no more pus or milk flew back and the cavity was no more visible at US.
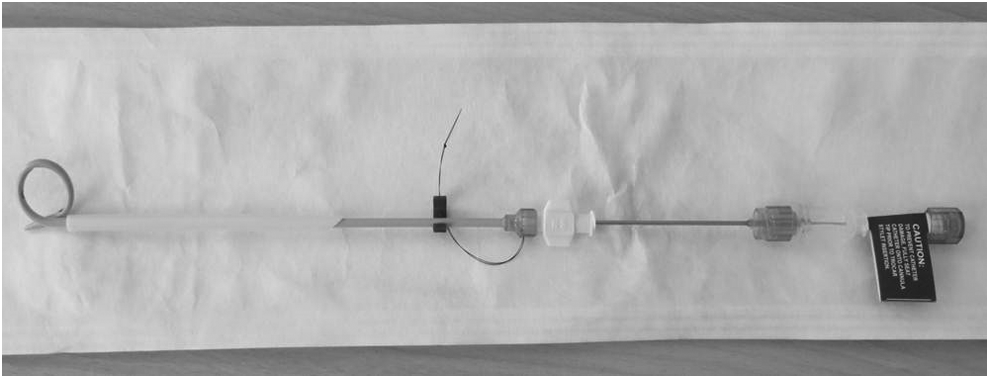
Eight French × 25 cm pigtail catheter HS general purpose L0825 Aprilia, Italy. HS, Hospital Service S.p.A.
Samples from all procedures have been submitted to the Department of Pathology for microbiological and cytological examination. Patients were strongly encouraged to continue breastfeeding from the unaffected breast and to use a breast pump to prevent milk stasis at the level of the affected breast (from which breastfeeding was not recommended). All procedures have been carried out without hospitalization and patients were discharged 2 hours after the treatment. Discharge therapy with paracetamol 1,000 mg up to four times/day and ampicillin 1 g twice daily was recommended. Breast abscesses resolution was clinically defined as no breast tenderness or palpable lump at the level of the previously affected breast area and complete absence of fluid collection at ultrasonographic examination.
The mean age of patients was 27.4 (range: 18–37) years. Twenty-three (67.6%) women were primipara and 11 (32.4%) multipara. Microbiological examination was negative in 10 patients. Sixteen samples have been found positive for Staphylococcus aureus and eight for Staphylococcus epidermidis. Cytologic examination was negative for malignant cells in all patients. The mean diameter of fluid collections was 5.4 (range: 3.3–9.7) cm and the volume of drained pus at first aspiration ranged from 25 and 70 mL (mean 47 mL). Clinical improvement was observed in all patients immediately after the procedure. Drainage through the catheter was maintained in place for an average of 11.5 days (range: 10–28). We found the procedure to be safe and well tolerated by all the patients, without reported complications. We reported no recurrences at a median follow-up of 9 months.
A randomized controlled trial in a larger population would be auspicable to achieve definitive results. However, our study demonstrates that US represents a useful tool for the diagnosis of breast abscesses, allowing the physician to evaluate the presence of single or multiple cavities. When a single-cavity large abscess is found, the surgeon has the possibility to avoid surgery, using an US-guided catheter drainage, a safe, well-tolerated, and cost-effective procedure, allowing women not to interrupt lactation with great advantages for both the mother and the child.
Footnotes
Disclosure Statement
No competing financial interests exist.