
Abstract
Abstract
Background:
Many mothers experience barriers to maintaining a breastfeeding relationship with their infants upon returning to work and, consequently, terminate breastfeeding earlier than recommended or intended. As such, employers are in a unique position to help further increase breastfeeding rates, durations, and exclusivity.
Objective:
The purpose of this review is to examine the literature regarding employer-based programs, policies, and interventions to support breastfeeding among working mothers.
Materials and Methods:
A systematic literature search was conducted for peer-reviewed articles published before April 2016. Studies were included if they focused on workplace-based lactation/breastfeeding support programs, policies, or interventions to promote breastfeeding among employees. For inclusion, articles must have measured at least one outcome, such as breastfeeding duration, breastfeeding exclusivity, or employee satisfaction.
Results:
Twenty-two articles were included, representing 10 different countries and both public- and private-sector employers, including governmental offices, schools, hospitals, manufacturing/industrial companies, and financial settings, among others. Providing a lactation space was the most common employer-based support accommodation studied, followed by breastfeeding breaks and comprehensive lactation support programs. The majority of studies analyzing these three support types found at least one positive breastfeeding and/or nonbreastfeeding outcome.
Conclusions:
This review suggests that maintaining breastfeeding while working is not only possible but also more likely when employers provide the supports that women need to do so. Although some employers may have more extensive breastfeeding support policies and practices than others, all employers can implement a breastfeeding support program that fits their company's budget and resources.
Introduction
R
In the United States, years of multifaceted strategies have improved breastfeeding rates. Between 2002 and 2013, the proportion of infants who were ever breastfed increased from 71.4% to 81.1%. 4 Still, in 2013, only 22.3% of infants were exclusively breastfed through 6 months 4 as recommended by WHO, and mothers' return to work is a contributing factor to this low rate.5,6 Many mothers experience barriers to maintaining a breastfeeding relationship with their infants upon returning to work and, consequently, terminate breastfeeding earlier than recommended or intended. 7 To be sure, the lack of workplace support is a frequently cited barrier of breastfeeding,8,9 and mothers have expressed fears surrounding the difficulties of expressing, storing, and transporting breast milk at work.10–12
Effective March 23, 2010, the Patient Protection and Affordable Care Act (PPACA, P.L. 111-148) amended the Fair Labor Standards Act (FLSA, 29 U.S.C. § 207) to require employers to provide “reasonable” unpaid break time and a private nonrestroom space where employees can express breast milk. 13 In addition, as of December 2015, 27 states, the District of Columbia, and Puerto Rico have enacted laws pertaining to workplace breastfeeding. 14 Still, only 40% of employed women with infants had access to both break time and a private space to express breast milk 3 years after enactment of the Break Time for Nursing Mothers Provision (2010), and single mothers and low-income women were significantly less likely to have access to either accommodation, reflecting systematic disparities in the workplace. 15 This is significant, since women with both adequate break time and a private space to express breast milk are 2.3 times more likely to exclusively breastfeed at 6 months postbirth. 15
Given that 56% of women in the United States workforce are of childbearing age (16–44 years old), and 61% of United States mothers with children under 3 years old are employed, 16 employers are in a unique position to help further increase breastfeeding rates, durations, and exclusivity. National and international health authorities recognize the importance of employers in helping women to continue breastfeeding and recommend workplace supports such as on-site day care facilities, breastfeeding breaks, flexible work arrangements, and facilities for expressing and storing breast milk.3,17,18
Compared to the number of studies identifying the benefits of breastfeeding, barriers to breastfeeding initiation and duration, and interventions for promoting breastfeeding initiation, relatively few studies have evaluated workplace supports to encourage and promote breastfeeding among working mothers. In fact, a 2012 Cochrane Review found no randomized or quasi-randomized controlled trials assessing the effectiveness of workplace interventions to support breastfeeding among mothers returning to work. 19 The purpose of this review is to examine the literature regarding employer-based programs, policies, and interventions to support breastfeeding among working women. Given similar attempts in the past,19,20 this review is not limited to randomized and quasi-randomized controlled trials. Based on our findings, we also propose specific recommendations for all employers beyond the minimum requirements of the Break Time for Nursing Mothers Provision (2010). 13
Materials and Methods
On April 12, 2016, four databases (CINAHL, PubMed, Social Services Abstracts, and Web of Science) were searched for relevant articles. The search strategy used was breastfe* AND (work OR workplace OR employ*) AND (intervention OR support OR program), where * signifies a truncation search to account for various endings. All article titles and abstracts were extracted into a single spreadsheet for review. Articles unrelated to breastfeeding support in the workplace were immediately excluded. Full-text articles were retrieved for further assessment if they initially fit the inclusion criteria: peer-reviewed journal articles focusing on workplace-based lactation/breastfeeding support programs, policies, or interventions to promote breastfeeding among employees. For inclusion, articles must have measured at least one outcome, such as breastfeeding duration, breastfeeding exclusivity, attendance at work, employee satisfaction, and so on. The search did not restrict on date of publication or type of study design used. Articles were excluded from the review if they were non-English, lacked a quantitative evaluation of outcomes, or were not geared toward employees. Thirty-nine additional articles that potentially met the above criteria were identified from reference lists of those retrieved from the database searches and subsequently reviewed.
After initial review of full-text articles, it was noted by several studies that the duration of maternity leave and one's employment status (i.e., full-time, part-time, and not employed) were found to affect breastfeeding exclusivity and/or duration.21–26 However, most of these studies did not indicate whether maternity leave and employment status were employer directed or employee initiated. For example, studies did not specify whether maternity leave was paid or unpaid. Likewise, it is unclear from many studies whether part-time work was an employer-sponsored accommodation, or if postpartum employees either worked part-time before birth or left their full-time jobs for part-time opportunities. Due to this lack of clarity, for the purposes of this review, studies that looked solely at maternity leave and/or employment status were excluded from the final review.
Two authors assessed the full-text articles for inclusion based upon the criteria listed above. Any disputes were resolved through discussions with the other author. Data from the final articles were then extracted into a summary table, including sample characteristics (e.g., sample size and demographics), type of workplace, type of breastfeeding support (e.g., lactation space, breastfeeding breaks, training/education/classes, and so on), breastfeeding rate, data collection method, years of data collection, outcome measures, results, and limitations reported in the articles.
Results
A total of 2,104 articles were retrieved from the four databases and from the reference lists of other articles. After the removal of duplicates, 1,439 articles were screened by title and abstract. Of these, 1,261 articles were excluded because they were unrelated to breastfeeding support in the workplace, leaving 178 articles potentially meeting the inclusion and exclusion criteria. After reviewing the full articles, the two authors agreed that 22 articles met the criteria for inclusion in this review (Fig. 1). It should be noted that two articles describe data from the same study, for a total of 21 unique studies.
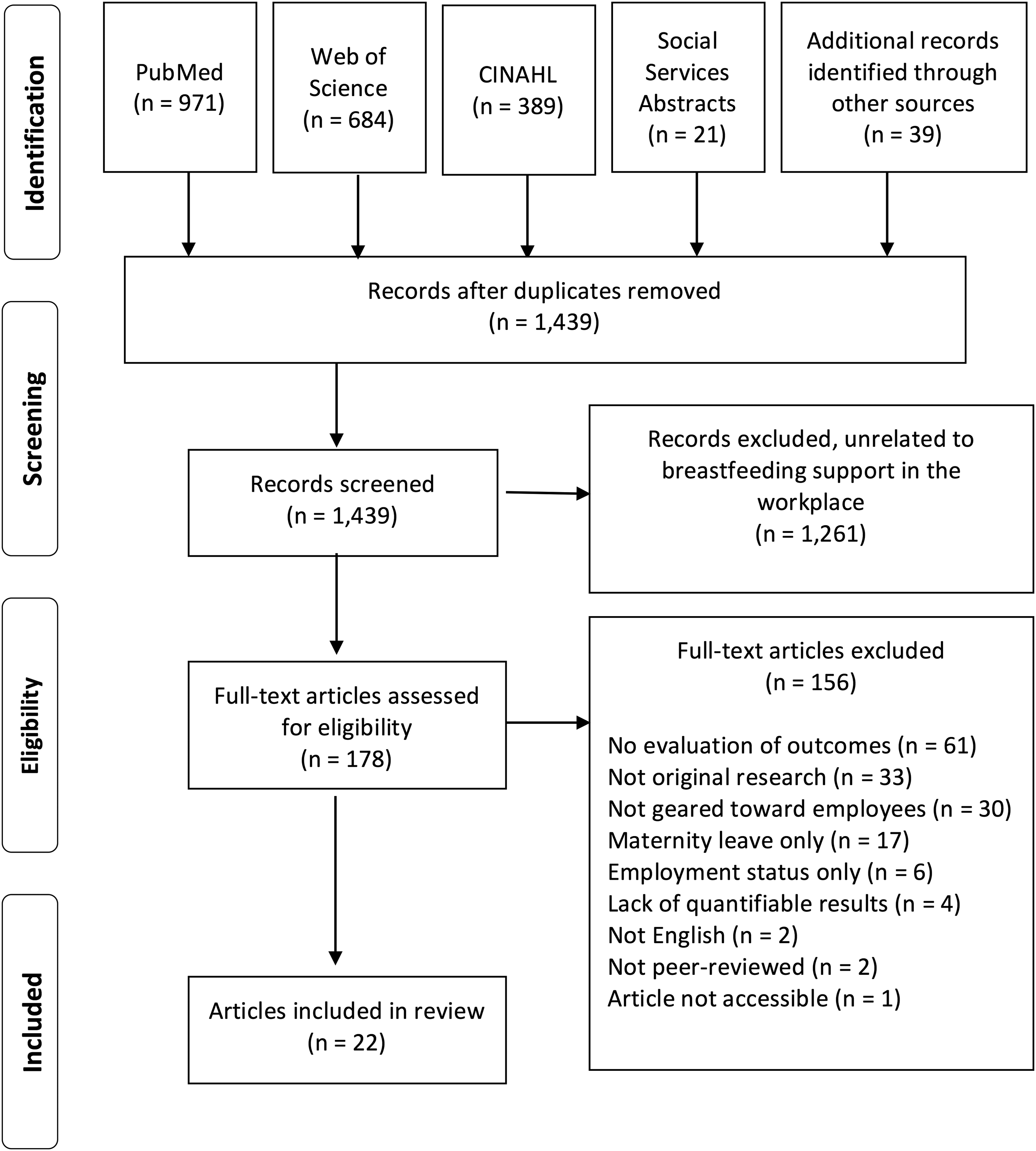
PRISMA flow diagram of search strategy and study selection.
Table 1 provides a summary of the sample characteristics of studies included for review. Eleven articles were based in the United States,5,6,9,10,15,27–32 three in Taiwan33–35 (two from the same study34,35), and one each from Indonesia, 36 Malaysia, 7 Thailand, 37 Iran, 38 Ghana, 39 United Kingdom, 8 Brazil, 40 and Puerto Rico. 41 Workplace type varied between public and private sectors, including governmental offices, schools, hospitals, manufacturing/industrial companies, and financial settings, among others. Studies reported the effects of between one and nine different workplace supports for breastfeeding employees. Providing a lactation space was the most common employer-based support accommodation studied (57.4%),5–7,15,33–36,38–41 followed by breastfeeding breaks (47.6%)6,7,10,15,33–35,38,39,41 and comprehensive lactation support programs (33.3%).5,10,27–29,32,37
This study focused on promoting breastfeeding through male employees (fathers). All other studies focused on female employees (mothers).
SD, standard deviation.
We report the effects of workplace supports by lactation accommodation; however in many cases, direct comparisons could not be made due to the differing intensities of workplace supports and/or varying outcome measures. Most studies measured the outcomes of breastfeeding initiation and duration (e.g., breastfeeding duration, breastfeeding at 6 months, and exclusive breastfeeding duration), although some studies assessed the use of infant formula,6,38 use of breast pumping breaks, 35 and employee satisfaction and job commitment. 39 Due to space constraints, we have only summarized the effects of the three most frequently evaluated workplace supports on breastfeeding initiation, breastfeeding duration, and exclusive breastfeeding. However, all workplace supports and their measured outcomes are summarized in Table 2. In addition, Table 3 provides a synthesis of the associations between workplace supports for breastfeeding and various breastfeeding and nonbreastfeeding outcomes.
Includes education and support by dedicated personnel for up to 12 months after birth.
Includes group breastfeeding education classes for fathers and their partners, individual or group lactation counseling, breast pumps to use at home/work, and daily lactation consultant availability.
Includes prenatal classes at work, electric breast pump and perinatal counseling by corporate lactation consultant, and RTW lactation maintenance services (lactation space, pumping equipment, education and counseling from lactation consultant, break time, portable cooler case, and milk storage bottles).
Includes electric breast pump, lactation space, refrigerator, breastfeeding consultation, and break time to pump.
Includes lactation spaces on campus, breast pump purchase program, free prenatal breastfeeding classes, Breastfeeding Resource Nurse course, loaner pump program for off-site, and breastfeeding breaks.
Includes lactation space, break time, breastfeeding education materials, job flexibility, breastfeeding support from nurse-midwives and/or lactation consultants, breast pumps, refrigerator, sink, comfortable chair and table, and Breastfeeding Committee.
aOR, adjusted odds ratio; aRR, adjusted rate ratio; CI, confidence interval; HR, hazard ratio; ME, marginal effect; OR, odds ratio; RTW, return-to-work; SE, standard error.
Numerals represent reviewed articles as listed in the reference list.
The type/method of training/education provided.
The length of time of breastfeeding after returning to work.
EBF, exclusive breastfeeding; RTW, return-to-work; +, significant positive association; Ø, no significant association;
Lactation space
Private spaces for milk expression were the most frequently studied lactation support, analyzed in 12 articles.5–7,15,33–36,38–41 Of these, Chen et al. 33 was the only study to assess the association with breastfeeding initiation, finding that female employees who were aware of the worksite lactation spaces had a 1.6 higher odds of breastfeeding initiation than women who were unaware of these spaces. In terms of breastfeeding duration, two studies found that women who were aware that their worksite had, 33 or was mandated to have, 41 a lactation space had 2.71 and 4.8 higher odds, respectively, of continuing breastfeeding after returning to work compared to women without such knowledge. Likewise, having access to a designated place for milk expression was associated with a 3.6 higher odds of continuing to breastfeed after returning to work compared to women working in workplaces without such spaces. 41 Conversely, two studies found that having access to a lactation space was not significantly associated with the extent of breastfeeding 6 or any breastfeeding 5 at 6 months compared to women without such access.
Several studies noted conflicting results depending on the breastfeeding duration outcome measure. For example, Tsai 34 found that women with access to a dedicated lactation space had a 2.38 greater odds of continuing to breastfeed beyond 6 months, but having access to such space was not predictive of breastfeeding continuation during the infant's first 6 months. Results from Kozhimannil et al. 15 were also mixed, showing that women with a private lactation space were not significantly more likely to breastfeed at all at 6 months postpartum compared with women without access to both a lactation space and breastfeeding breaks. However, women with a private lactation space breastfed for 1.36 months longer than women with no private space or breastfeeding break. 15 Among the sample in the study by Amin et al., 7 there was no significant difference in breastfeeding discontinuation between women with and without access to a lactation space. Yet for those women without both a lactation space and refrigerator, the odds of breastfeeding discontinuation were 1.8 times higher compared to women with access to both these accommodations. 7
Among studies examining the association between lactation space and exclusive breastfeeding, Basrowi et al. 36 found that women with access to a dedicated lactation space at work had a 2.62 higher odds of exclusively breastfeeding compared to mothers without access. On the contrary, Balkam et al. 5 found no significant differences in exclusive breastfeeding at 6 months between women who did and did not have access to a lactation space. Results from Kozhimannil et al. 15 were mixed, showing that women with a private space to express breast milk were not significantly more likely to exclusively breastfeed at 6 months postpartum compared to women without access to both a lactation space and breastfeeding breaks. However, women with a private lactation space were 3.8 times as likely to continue exclusively breastfeeding each month compared to women without access to either accomodation. 15
Breastfeeding breaks
Ten articles6,7,10,15,33–35,38,39,41 analyzed the awareness, availability, or use of break time for breast milk expression. Of these, Chen et al. 33 was the only study to assess the outcome of breastfeeding initiation, finding no significant association between mothers' awareness of breast pumping break policies and breastfeeding initiation. With regard to breastfeeding duration, studies are conflicting. In the study by Chen et al., 33 women who were aware of breast pumping break policies had 2.68 higher odds of continuing breastfeeding after returning to work. Yet Tsai 35 found that women's awareness of the breast pumping break policy was not a significant predictor of continuing to breastfeed during the first 6 months postpartum or continuing to breastfeed for more than 6 months. 34
Among studies examining break time availability and use, most show positive associations with breastfeeding duration.7,15,34,41 For example, the study by Kozhimannil et al. 15 revealed that women with reasonable break time to pump were 2.6 times as likely to exclusively breastfeed and 3.0 times as likely to breastfeed at all at 6 months postpartum compared with women without access to either break time or lactation spaces at work. Likewise, in the study by Tsai, 34 use of breastfeeding breaks was a significant predictor of continuing to breastfeed during the first 6 months and continuing to breastfeed for more than 6 months. However, two studies found no significant association between break time for milk expression with the extent of breastfeeding at 6 months 6 or the duration of exclusive breastfeeding. 10
When looking at access to both lactation space and break time, Kozhimannil et al. 15 found that women were 2.3 times as likely to exclusively breastfeed, but not significantly more likely to breastfeed at all, at 6 months postpartum compared with women without access to either breastfeeding accommodation. Women with both accommodations were also 1.5 times as likely to continue exclusively breastfeeding each month compared to women without access to either accommodation. 15
Comprehensive lactation support program
Eight articles5,10,27–29,32,36,37 examined the association of comprehensive lactation programs (defined in this study as a combination of three or more support types analyzed together) and one or more breastfeeding outcomes. Of these, Spatz et al. 29 was the only study to assess the outcome of breastfeeding initiation, finding that hospital employees with access to a comprehensive lactation support program had significantly higher rates of breastfeeding initiation compared to national rates. 29
Among the studies analyzing breastfeeding duration, all showed that women with access to a comprehensive lactation support program at work either had significantly lower rates of breastfeeding discontinuation upon returning to work, 32 longer duration of breastfeeding, 32 higher rates of any breastfeeding at 6 months27–29,37 and 12 months, 29 longer duration of exclusive breastfeeding,10,32 and higher rates of exclusive breastfeeding at 6 months.5,36,37
Likewise, Balkam et al. 5 found that, with each additional breastfeeding support service received (between one and four services), the percentage of respondents who were exclusively breastfeeding at 6 months increased. This relationship did not appear for any breastfeeding at 6 months. In regression analysis, the number of services received was positively related to exclusive breastfeeding at 6 months. 5 Bai and Wunderlich 10 also found a significant and positive correlation between workplace environment and the duration of exclusive breastfeeding.
Discussion
Based on these studies, it is clear that breastfeeding supports have been implemented in a variety of workplaces across the world, including public and private companies, large and small organizations, and both male-dominated and more mixed-gender environments. This review highlights evidence that maintaining breastfeeding while working is not only possible but also more likely when employers provide the supports that women need to do so. Although some employers may have more extensive breastfeeding support policies and practices than others, all employers can implement a breastfeeding support program that fits their company's budget and resources.
Among the studies reviewed in this study, providing a lactation space and breastfeeding breaks were the two most common breastfeeding supports reported. The majority of these indicate at least one positive breastfeeding or employee satisfaction/commitment outcome as a result of these two supports. In the United States, both a private space and “reasonable” break time to express breast milk are required by employers covered by the FLSA. 13 While this is a great start to assist mothers who breastfeed, more can be done to help women succeed in meeting the WHO and UNICEF recommendations of exclusive breastfeeding for 6 months and continued breastfeeding for up to 2 years of age or more. 3 In fact, of the studies that analyzed comprehensive lactation support programs (each with three or more supports), all eight found at least one positive breastfeeding outcome. Results from Balkam et al. 5 show that the number of breastfeeding support services received was positively related to exclusive breastfeeding at 6 months, suggesting a dose–response effect. In other words, the more supports available for mothers, the better the chances of continued breastfeeding.
Studies also analyzed other types of supports that, in many cases, improved breastfeeding outcomes for working mothers. These include flexible work schedules, breastfeeding training and pumping education, employer-sponsored childcare, coworker and supervisor support, breast pumps at work, refrigerators for breast milk storage, and breastfeeding support groups. Several of these supports can be provided at little to no cost to the employer. For example, mini-refrigerators can be purchased for under $100, and lockers for women to store their pumps during the workday may cost between $200 and $400 or less, depending on the number needed. Instead of hiring a lactation consultant for the company, workplaces can make sure that employees are given the phone number to breastfeeding “warm lines” so that breastfeeding-related questions or concerns can be addressed. These “warm lines” are usually linked to hospitals and can be easily accessed from many states like California, 42 Rhode Island, 43 and Connecticut 44 for mothers to use after being discharged from the hospital.
We also recommend that employers alert their employees of the covered no-cost lactation services now available to them through their health insurance as a result of the PPACA, specifically a breast pump and lactation consultant services. Employees can find local lactation consultants through their insurance company or online databases, such as ZipMilk.org. 45 ZipMilk.org is currently available in eight states and serves as a listing of lactation consultants; educators; Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) Breastfeeding Coordinators; and other sources of lactation help within a designated zip code. 45 If a state is unlisted, mothers can contact their state's Breastfeeding Coalition or the Lactation Consultant Directory maintained by the International Lactation Consultant Association. 46 By promoting websites like ZipMilk.org, employers are also supporting the practice of breastfeeding and creating an encouraging breastfeeding-friendly environment in the workplace.
More organizations should create company-specific policies by referring to the Office on Women's Health website. 47 For one, this website illustrates simple and affordable solutions for various types of workplaces to implement a lactation space for working mothers. While constructing a lactation space may seem costly and time consuming, the website recommends cost-effective solutions like tents, vacant conference rooms, fitting rooms at retail stores, and other “space solutions” that can be used. 47 Nonetheless, employers may experience higher productivity, reduced absenteeism, and increased employee retention as a result of providing a lactation space and other supports for breastfeeding mothers. 47
Although this review illustrates the positive effects that employer-based lactation support services can have on breastfeeding and other outcomes, several limitations of this review must be noted. First, given the current lack of controlled studies,19,20 all studies included in the review utilized an observational research design. Less than half (43%) of studies measured and controlled for covariates, and among these, not all studies measured the same variables. As a result, there is a potential for unknown confounding and more controlled research is necessary to better understand the benefits of employer-sponsored programs to promote, encourage, and support breastfeeding among working mothers. Next, the definition of lactation supports and breastfeeding outcomes was not uniform (e.g., varying descriptions of lactation spaces) and at times undefined (e.g., predominant breastfeeding 40 ) making the results more difficult to compare across studies. Likewise, some studies focused only on employees of healthcare facilities and WIC centers. Given the nature of their work, these mothers may have relatively higher rates of breastfeeding intentions and behaviors even without lactation accommodations in the workplace, and thus, the findings of these studies may not be generalizable to other types of employers. Still, this review includes a variety of workplace lactation supports implemented in a diverse range of geographic locations and industries, and trends across the studies indicate positive and significant impacts between these supports and both breastfeeding and nonbreastfeeding outcomes.
Conclusion
Based on this review, most types of workplace lactation support services show promise in increasing rates of breastfeeding initiation, duration, and exclusivity among working mothers. Research also suggests that women with access to these supports have higher job satisfaction and job commitment. 39 Finally, it appears that the more workplace supports in place, the higher the likelihood of breastfeeding initiation and duration. More employers should consider adopting a workplace breastfeeding support policy to benefit not only their employees but also the company at large, since companies that adopt a breastfeeding support program save an average of three dollars for every dollar they invest. 48 With the federal mandate as a necessary first step toward creating supportive workplace environments, employers can also contribute to the success of breastfeeding mothers with the investment in and promotion of additional services, interventions, and supports.
Footnotes
Disclosure Statement
No competing financial interests exist.