
Abstract
Abstract
Background:
Little is known about how in-hospital supplementation with water, infant formula, or sugar water affects the relationship between breastfeeding intentions and duration, and whether this differs by gestational diabetes mellitus (GDM) history. Our study objectives were to assess the associations between GDM and exclusive breastfeeding intentions, hospital supplementation, and breastfeeding duration, including whether hospital supplementation mediates the association between exclusive breastfeeding intentions and breastfeeding duration.
Study Design and Methods:
Using data from the Infant Feeding Practices Study II (2005–2007), we included women with GDM (n = 160) and women without GDM or prepregnancy diabetes (no diabetes mellitus [NDM]) (n = 2,139). We used multivariable logistic and linear regressions to determine the associations between GDM history and exclusive breastfeeding intentions, and between breastfeeding intentions, hospital supplementation, and breastfeeding duration, by GDM. We used mediation analysis to assess whether hospital supplementation mediated the association between exclusive breastfeeding intention and breastfeeding duration, also by GDM. All analyses were adjusted for prepregnancy body mass index.
Results:
GDM was associated with lower odds of intending to exclusively breastfeed (adjusted odds ratio [AOR] 0.71; 95% confidence interval [CI, 0.51–0.99]). GDM and NDM women who did not intend to exclusively breastfeed had similarly increased odds of hospital supplementation (GDM: AOR 3.52; 95% CI [1.44–8.57], NDM: AOR 3.66; 95% CI [2.93–4.56]). Breastfeeding duration was similar by exclusive breastfeeding intentions and by hospital supplementation, regardless of GDM. Hospital supplementation partially mediated the association between breastfeeding intentions and duration in NDM women, but it did not mediate the association in women with GDM.
Conclusions:
Breastfeeding intentions, rather than hospital supplementation, are particularly important for women with GDM to optimize breastfeeding outcomes.
Introduction
G
Breastfeeding intention is a strong predictor of breastfeeding outcomes,8–11 and it may even be a stronger predictor than other predictors combined. 8 However, the body of literature on breastfeeding intentions among women with and without GDM history has only recently emerged, with inconsistent results likely due to varying definitions and comparison groups. For example, three previous studies examined breastfeeding intentions by different diabetes types, including GDM.12–14 In two of the studies,12,13 intention was not clearly defined (e.g., exclusive versus any), nor was the timing of when the intention was assessed (e.g., prenatal [before GDM diagnosis] versus at delivery [after GDM diagnosis]). In the third study, 14 feeding intentions were assessed at admission to one, large academic hospital; among women with GDM, 39% intended to engage in any breastfeeding (no differentiation of exclusive breastfeeding intention), 32% intended to exclusively feed formula, and 29% were undecided; because there was no comparison group in this study, it is unknown how these GDM intentions may differ from women without diabetes/GDM. Promoting positive breastfeeding intentions is an implementable intervention that can contribute to increasing the proportion of women who meet breastfeeding recommendations, and it can contribute to meeting national breastfeeding goals. 15 Understanding how intentions may differ, and how intentions are associated with outcomes, is critical to adapting these interventions to women with GDM.
Despite strong breastfeeding intentions, various maternal/infant factors can alter even the strongest intentions. Studies consistently show that women with GDM are more likely to supplement with formula during hospital stay compared with women without diabetes.12,16 Increased supplementation among women with GDM may or may not be related to common adverse outcomes that are associated with GDM and poor breastfeeding outcomes (e.g., obesity, cesarean section, Neonatal Intensive Care Unit (NICU) admission, delayed onset of lactogenesis, etc.). Regardless of the reasons for supplementation, high rates of hospital supplementation are of concern as multiple studies document that formula supplements during the maternity stay are associated with shortened durations of both exclusive17,18 and “any” breastfeeding.19,20 It is unclear whether early formula supplementation is causally related to shortened breastfeeding duration, 21 which is an essential research question considering that a maximum of 2 out of 3 of women with GDM are reported to experience hospital supplementation, 16 although this may vary considerably across hospital settings. The objectives of this study were to assess associations between exclusive breastfeeding intentions (in the first few weeks) and GDM; and to assess associations between intentions, hospital supplementation, and total breastfeeding duration by GDM history, including assessment of hospital supplementation as a mediator in the association between exclusive breastfeeding intentions and total breastfeeding duration.
Materials and Methods
Sample
We obtained data from the Infant Feeding Practices Study II (IFPS II), a longitudinal study of mailed surveys to women from late pregnancy through their infant's first year of life, conducted from 2005 through 2007 by the Food and Drug Administration collaboratively with the Centers for Disease Control and Prevention. Women were recruited in their third trimester of pregnancy through a consumer-opinion mail panel. Qualifying criteria included mothers who were at least 18 years old, both mother and infant being without medical conditions that would affect feeding, and the infant being born after at least 35 weeks of gestation and weighing at least 5 lb. Questionnaires were sent once prenatally and 10 times over a 1-year period postpartum, asking about various infant feeding practices. Extensive details of the IFPS II methodology and sample have been previously published. 22 Our study was exempt from ethical approval because it was a secondary analysis of a publicly available, de-identified data set.
Main exposure
Women were classified as having GDM if they responded “yes” to the following question in the prenatal questionnaire: “Have you had gestational diabetes with this pregnancy?” Self-reported gestational diabetes has been shown to be a valid measure of GDM. 23 Women completed the prenatal questionnaire during their third trimester, after they would have been screened for and diagnosed with gestational diabetes. In the same questionnaire, women were separately asked whether they had “juvenile onset diabetes (Type 1)” or “adult onset diabetes (Type 2)”? We used responses to these questions to create two categories for comparison: (1) women who responded yes to GDM versus (2) women who responded no to GDM, type 1 or type 2 diabetes, herein referred to as women without diabetes (no diabetes mellitus [NDM]). Women who responded yes to type 1 or type 2 diabetes were excluded from this analysis.
Outcome measures
Prenatal breastfeeding intention
We assessed the prenatal breastfeeding intention to exclusively breastfeed in the first few weeks, by using the following question from the prenatal questionnaire: “What method do you plan to use to feed your new baby in the first few weeks?” Women who responded “Breastfeeding only” were categorized as intended to exclusively breastfeed. Women who responded “Breastfeeding and formula” or “formula only” were classified as not intending to exclusively breastfeed.
Breastfeeding duration
We assessed the duration of any breastfeeding in weeks by using the following question: “How old was your baby when you completely stopped breastfeeding and pumping milk?”
Hospital supplementation
Infants who had ever breastfed were considered to have received hospital supplementation if they were not exclusively breastfed during the hospital stay, by using the following question from the neonatal questionnaire: “While you were in the hospital or birth center, was your baby fed water, formula, or sugar water at any time?”
Other variables
The following additional variables were assessed as potential confounders: maternal age (years), race ethnicity (White, Black, Hispanic, or other), marital history (currently married versus not currently married), mother received WIC support while pregnant (yes versus no), household income as a percentage of federal poverty level (<185%, 185–349%, ≥350%), smoking during third trimester (yes versus no), planning to go back to work (yes versus no), first birth (yes versus no), and prepregnancy body mass index (BMI; kg/m2) by using self-reported height and weight (as a continuous variable or grouped as a three-level categorical variable—Normal weight: 18.5 kg/m2 to <25 kg/m2; Overweight 25 kg/m2 to <30 kg/m2; Obese ≥30 kg/m2) according to Institute of Medicine criteria.
Statistical analysis
Our study included women with GDM (n = 160) and women without diabetes (NDM) (n = 2,139). We used χ2 and Fisher's exact tests of statistical significance for the comparison of categorical variables, and t-test and Wilcoxon rank sum tests for the comparison of continuous variables. We used two-sided p-values with a level of significance at p < 0.05.
Logistic regression was used to determine the crude and adjusted associations between GDM history and exclusive breastfeeding intention. We used multivariable logistic regression to assess the association between breastfeeding intention and hospital supplementation. We used multivariable linear regression to evaluate adjusted associations between exclusive breastfeeding intention and breastfeeding duration, and between hospital supplementation and breastfeeding duration. Our a priori hypothesis was that mediation of hospital supplementation would differ by GDM; therefore, we stratified all analyses by GDM. Each of the potential confounders was included in an adjusted model if their inclusion satisfied an a priori change-in-estimate criterion (a change in the odds ratio [OR] of ≥10%). Only prepregnancy BMI satisfied this criterion; therefore, prepregnancy BMI was the only variable included in the adjusted models.
We tested hospital supplementation as a mediator in the association between breastfeeding intentions and duration. A mediator is a variable that is on the causal pathway between an exposure and outcome of interest (Fig. 1). As hospital supplementation is a categorical variable, we used the counterfactual approach to mediation analysis as presented in Valeri and Vanderweele. 24 This approach allowed us to obtain natural direct, indirect, and total effects in scenarios where the product method, as is typically used when assessing a continuous mediator, is no longer valid due to nonlinearities that arise within the statistical models employed. Total effects indicate the effect of breastfeeding intentions on breastfeeding duration (Fig. 1, path C), whereas indirect effects indicate the effect of breastfeeding intentions on breastfeeding duration, specifically through hospital supplementation (Fig. 1, Paths A and B). To determine whether mediation differed by GDM history, we stratified the mediation analyses by GDM history. We used Mplus 7 to obtain effect sizes, such as indirect effects, total effects, and proportions for the indirect effect relative to the total effects, and statistical tests for indirect and total effects. All other statistical analyses were completed by using SAS Studio 3.4 (Enterprise Edition) SAS Institute, Inc. (Cary, NC).
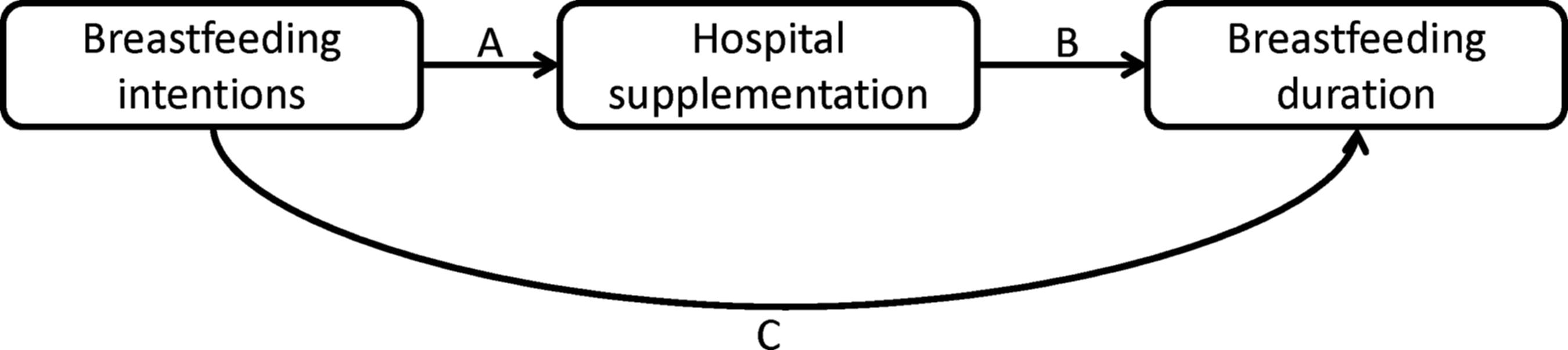
Conceptual model of mediation analysis.
Results
Women with GDM were older, more likely to report smoking during their third trimester, and more likely to be obese (Table 1). Duration of breastfeeding was shorter for women with GDM compared with NDM women (21.4 and 24.6 weeks respectively, p = 0.04). Significantly fewer women with GDM (51.9%) intended to exclusively breastfeed in the first few weeks compared with NDM women (63.0%) (Table 2A). Both GDM and greater prepregnancy BMI were independently associated with lower intentions to exclusively breastfeed during the first few weeks, and GDM remained significantly associated with lower breastfeeding intentions after adjusting for prepregnancy BMI (adjusted odds ratio [AOR] 0.71, 95% confidence interval [CI, 0.51, 0.99]; p < 0.001) (Table 2A).
Bold results are statistically significant (p < 0.05).
t-test or Wilcoxon rank-sum test, as appropriate, for continuous variables; χ2 or Fisher's exact test, as appropriate, for categorical variables.
GDM, gestational diabetes mellitus; NDM, no diabetes mellitus.
Bold results are statistically significant (p < 0.05).
Not applicable, prepregnancy BMI was assessed as a continuous variable; intentions by BMI categories were: 65.9% normal (18.5–24.9 kg/m2), 61.3% overweight (25.0–29.9 kg/m2), and 56.7% obese (≥30.0 kg/m2); p < 0.001.
Mean difference in breastfeeding duration (weeks).
Adjusted for exclusive breastfeeding intention and prepregnancy BMI.
BMI, body mass index; CI, confidence interval.
The mean duration of breastfeeding was longer for women who intended to exclusively breastfeed during the first few weeks, compared with those who did not intend to exclusively breastfeed, for both GDM and NDM women (mean difference in breastfeeding duration comparing women with exclusive intentions and those without exclusive intentions [adjusted beta coefficient]: 22.3 weeks [95% CI (16.6–28.0); p < 0.001] [GDM] and 20.7 weeks [95% CI (19.1–22.3); p < 0.001] [NDM]) (Table 2B).
Women with GDM were more likely to supplement compared with women with NDM (63.5% versus 46.4%, respectively, p < 0.001) (Table 3A). Not having exclusive breastfeeding intentions was associated with increased odds of hospital supplementation in both women with GDM and women with NDM (GDM: AOR 3.52; 95% CI [1.44–8.57], NDM: AOR 3.66; 95% CI [2.93–4.56]; results not shown). In turn, hospital supplementation was associated with shorter breastfeeding duration, in both women with GDM and women with NDM (mean difference in breastfeeding duration comparing women who did not supplement with those who did: 13.1 weeks [95% CI (5.8–20.4); p < 0.001] [GDM] and 10.1 weeks [95% CI (8.3–11.8); p < 0.001] [NDM]) (Table 3B).
Bold results are statistically significant (p < 0.05).
Not applicable, prepregnancy BMI was assessed as a continuous variable; supplementations by BMI categories were: 43.5% normal (18.5–24.9 kg/m2), 50.4% overweight (25.0–29.9 kg/m2), and 52.3% obese (≥30.0 kg/m2); p = 0.002.
Mean difference in breastfeeding duration (weeks).
Adjusted for in-hospital supplementation and prepregnancy BMI.
Mediation analysis
In NDM women, hospital supplementation was found to partially mediate the association between exclusive breastfeeding intention and breastfeeding duration, after adjusting for prepregnancy BMI (total effect: 14.54, indirect effect 2.03, p < 0.001) (Table 4). However, in GDM women, after accounting for prepregnancy BMI, hospital supplementation did not significantly mediate the association between breastfeeding intentions and duration (Total effect: 14.76, indirect effect 1.31, p = 0.22).
Bold results statistically significant (p < 0.05).
Discussion
No previous studies have addressed differences in breastfeeding intentions by GDM history or attempted to quantify mediating factors, likely because breastfeeding intention, hospital supplementation, breastfeeding duration, and GDM history rarely exist in the same, longitudinal dataset. Our results showed that after adjusting for prepregnancy BMI, fewer women with GDM have exclusive breastfeeding intentions than NDM women, which, in turn, increases the likelihood that they will supplement in the hospital. Despite similar relationships between exclusive intention and supplementation, and between supplementation and duration, regardless of GDM, hospital supplementation did not emerge as a significant mediator in the association between intention and duration among women with GDM. However, the association between exclusive intentions and duration remained significant in GDM women, indicating that intentions are particularly important for women with GDM to optimize breastfeeding outcomes. This finding suggests that it is important to identify prenatal counseling strategies that impact breastfeeding intentions among women with GDM, especially because of the lasting metabolic benefit from lactation that these women experience. 7
As previously mentioned, three studies assessed GDM and breastfeeding intentions.12–14 Two of these studies assessed breastfeeding intentions among women with GDM, but they did not include a reference group of NDM women, thereby limiting the ability to assess an association between GDM history and breastfeeding intentions.13,14 The third study found no difference in breastfeeding intentions between women with GDM and women with NDM. 12 Our study found conflicting results, likely because the previous study did not provide an indication of how breastfeeding intention was assessed or any nuanced detail regarding level of intentions. Our study also suggests that reporting crude differences in breastfeeding duration by GDM is not telling the whole story; we found no difference in breastfeeding duration by GDM among women who intended to exclusively breastfeed, indicating the importance of accounting for breastfeeding intentions when examining duration (by either adjusting for intentions or restricting the population to women who intended to breastfeed).
Several studies found that breastfeeding initiation was lower and breastfeeding duration was shorter among obese women compared with nonobese women.25–27 Despite the strong association between obesity and lower breastfeeding intentions, the association between GDM and lower exclusive breastfeeding intentions remained after adjusting for prepregnancy BMI. This highlights the importance of GDM history as an independent risk factor for lower breastfeeding intentions, and the importance of focusing on increasing breastfeeding education for women with GDM, in particular.
There are a few explanations as to why fewer women with GDM intend to exclusively breastfeed in the first few weeks. First, women with GDM may be educated on potential adverse delivery outcomes that are known to impact breastfeeding (e.g., obesity, cesarean section, NICU admission, delayed onset of lactogenesis, etc). Thus, women may decide that exclusive breastfeeding may be too challenging or not a priority compared with their own recovery or their infant's health. Conversely, due to the high-risk pregnancy that these women experience, healthcare providers may focus solely on the immediate concerns of a healthy baby, and less on discussing the importance of breastfeeding—a missed opportunity to provide prenatal breastfeeding education. Finally, some women with GDM may have lower breastfeeding self-efficacy, compared with women with NDM. 28 Improving self-efficacy may play a vital part in increasing breastfeeding intentions and as a result, increasing breastfeeding duration.
We found that among women with GDM, supplementation was not a significant mediator between intentions and duration, which is different from women without diabetes. This difference by GDM may indicate that for women with GDM, breastfeeding intentions play a more important role in determining breastfeeding duration than supplementation. Women with strong prenatal intentions to breastfeed are most likely to overcome hurdles to successfully initiate and continue breastfeeding.8,9,27 Furthermore, infant supplementation may not affect women with GDM in the same way that it does affect women with NDM, since women with GDM may be more likely to anticipate or accept breastfeeding problems in the early postpartum period, and as a result may be more willing to provide limited supplementation in combination with breastfeeding. Although the medical necessity for formula introduction during hospital stay has been questioned, 21 if the reasons for early supplementation cannot be avoided (due to either medical or nonmedical reasons) limited formula use may be beneficial to help mothers overcome temporary breastfeeding issues and even prolong breastfeeding duration.29–31 Such an approach should include prescribed, supervised limited formula use 21 with education to sustain breastfeeding and discontinue formula use after the medical/nonmedical needs subsides and after onset of mature milk production. 29
Our study is the first to explore the differences in intentions to breastfeed between women with GDM and women with NDM, and associations between breastfeeding intentions, hospital supplementation, and breastfeeding duration by using sophisticated analytical methods. However, our study had some limitations. First, IFPS II is not a nationally representative survey, which limits the generalizability of our findings. We recognize that the IFPS data are now over a decade old; however, it is still the best data source available to assess these issues of breastfeeding intention and duration, as IFPS II is the largest, U.S. prospective survey to date of breastfeeding intentions and outcomes. Second, the fact that there were only 160 women with GDM in our sample, of whom only 127 women had information regarding supplementation, restricted our analytical abilities. Finally, intention to breastfeed was assessed in the prenatal questionnaire, in the third trimester, after women had been diagnosed with GDM. It is possible that a GDM diagnosis influenced women's intention to breastfeed. Future studies should assess intention before and after GDM diagnosis, to understand the impact that GDM diagnosis has on women's intentions to breastfeed.
Conclusion
Efforts must be made to improve breastfeeding intentions among women with GDM. Even a brief 5 minute prenatal consultation can improve women's intention to breastfeed, 27 which is associated with improved breastfeeding outcomes. 8 Along with women themselves, healthcare providers 32 and hospitals play an important role in a woman's decision to breastfeed; 33 thus, targeting the woman, healthcare providers, and hospitals may be an effective multi-component approach 32 to increasing the prevalence of intentions and actual breastfeeding in women with GDM.
Footnotes
Disclosure Statement
No competing financial interests exist.