
Abstract
Abstract
Objectives:
Idiopathic granulomatous mastitis (IGM) is a benign breast disease with no ideal treatment regimen so far. This study aimed to evaluate the complete remission/resolution (CR) rate and recurrence rate of different treatment options.
Methods:
We systematically searched and identified eligible studies from January 1, 2010, to December 31, 2015, in PubMed, EMBASE, Cochrane Central Register of Controlled Trials, and Medline databases. We included original studies reporting the CR and/or recurrence rate of each treatment used. The pooled incidence and 95% confidence interval (95% CI) for CR and recurrence rate were calculated using Stata 13.0.
Results:
Fifteen eligible studies were included in our study. Six, nine, and five studies with 138, 358, and 106 patients were analyzed for surgical managements, oral steroids, and oral steroids+surgical managements, respectively. The pooled estimates for CR rate of them were 90.6% (95% CI 83.8%, 95.7%), 71.8% (95% CI 67.1%, 76.3%), and 94.5% (95% CI 88.9%, 98.3%). The pooled estimates for recurrence rate were 6.8% (95% CI 3.3%, 11.5%), 20.9% (95% CI 9.2%, 16.1%), and 4.0% (95% CI 1.5%, 8.4%), respectively. Other interventions analyzed were topical steroids, observation, oral steroids+MTX, and steroids+prolactin lowering agent, with varied pooled estimates for CR and recurrence rate.
Conclusion:
Surgical managements had high CR rate with relatively low recurrence rate, with or without steroids. Thus, it was suitable for patients requiring rapid remission. However, for patients with concerns about surgical scarring, oral steroids could be an acceptable option. Further investigations are still needed to better understand the managements of IGM.
Introduction
I
A definitive diagnosis should be established based on clinical, radiological, or sonographic appearance, as well as the histological examination.2–5 To establish a diagnosis of IGM, other causes of granulomatous mastitis, such as infectious diseases, tuberculosis, sarcoidosis, foreign-body reaction, hormonal disruption, should be excluded. More importantly, malignant diseases should be excluded.
No consensus or guideline currently exists on the ideal treatment regimen for patients with IGM. Available treatment options include antibiotic therapy, systemic or topical steroids, immunosuppressive therapy such as methotrexate (MTX), wide local excision, mastectomy, and close follow-up.2,3,5–10 The complete remission/resolution (CR) and recurrence rates of different treatment options reported in currently available studies varied.
Hence, we conducted a systematic review and meta-analysis, including 15 studies,11–25 to evaluate the CR and recurrence rates of different treatment options.
Methods
Data source
Two authors (X.L., K.C.) did a systematic review to identify studies addressing the complete remission rate and/or recurrence rate of IGM using different treatments. We did a comprehensive search of databases, including PubMed, EMBASE, Cochrane Central Register of Controlled Trials, and Medline, to identify studies published between January 1, 2010, and December 31, 2015. The search terms used were “idiopathic granulomatous mastitis,” “IGM,” “granulomatous lobular mastitis,” “treatment,” “management,” “intervention,” “remission,” “recurrence,” and “prognosis.”
Selection criteria
Inclusion criteria
(1) Study design: published research articles, including randomized controlled trials, cohort studies, and case/control studies, were included; review articles, meta-analysis, editorial or comment articles, and case reports were excluded.
(2) Study that reported the CR rate and/or recurrence rate of different treatments for IGM.
(3) Published in English.
(4) Full-text available.
Subjects and intervention
(1) Subjects included: patients with a clinical manifestation and pathological feature of noncaseating granulomatous inflammation of unilateral or bilateral breasts, who have excluded other causes of granulomatous mastitis.
(2) Interventions: oral steroids; topical steroids; MTX; surgical managements including drainage, lumpectomy, wide local excision, and mastectomy; observation; prolactin lowering agents; or the combination of two or three of the treatments described above.
Observation index
(1) CR rate:
Definition of CR: skin changes were completely ameliorated, complete disappearance of inflammatory signs in the affected breast, inactivity of fistulas, close of the fistula orifices and/or skin erosions.
(2) Recurrence rate:
Definition of recurrence: reappearance of inflammatory skin changes, lump, ulcer, and fistula after the complete remission of IGM.
Exclusion criteria
(1) Studies about granulomatous mastitis with clear causes such as infectious diseases, tuberculosis, sarcoidosis, and foreign-body reaction.
(2) Studies about IGM without CR rate or recurrence rate for each treatment stated in that study.
The title and abstract of all studies identified in the search were reviewed by two reviewers (X.L., K.C.) independently to exclude studies that did not meet the selection criteria. Full texts of the remaining articles were further examined to determine whether they contained information that could answer the research question of interest. We also checked reference lists of included articles for additional studies. Any discrepancies or inconsistent findings were solved by discussion, going through all the original materials, and counseling experts (S.R.L., F.X.S).
Data extraction
Two independent reviewers (X.L., L.L.Z.) extracted data from the selected studies using a predefined data extraction sheet. The extracted data included name of the first author of the study, year of publication, name of the journal, intervention, sample size, follow-up period, observation index, etc.
Data analysis
The meta-analysis was performed using Stata 13.0 (Stata.), the pooled incidence and 95% confidence interval (95% CI) were calculated. We also used I square (I2) for quantitative analysis of heterogeneity. If I2 ≥ 50%, it suggested that heterogeneity was significant among studies included. If there was no significant heterogeneity among studies included, the fixed-effects model, Mantel–Haenszel test, was used for meta-analysis. Otherwise, the randomized-effects model was used.
Results
We identified 264 potentially relevant citations, of which 1513–27 were finally included in our analysis (Fig. 1).
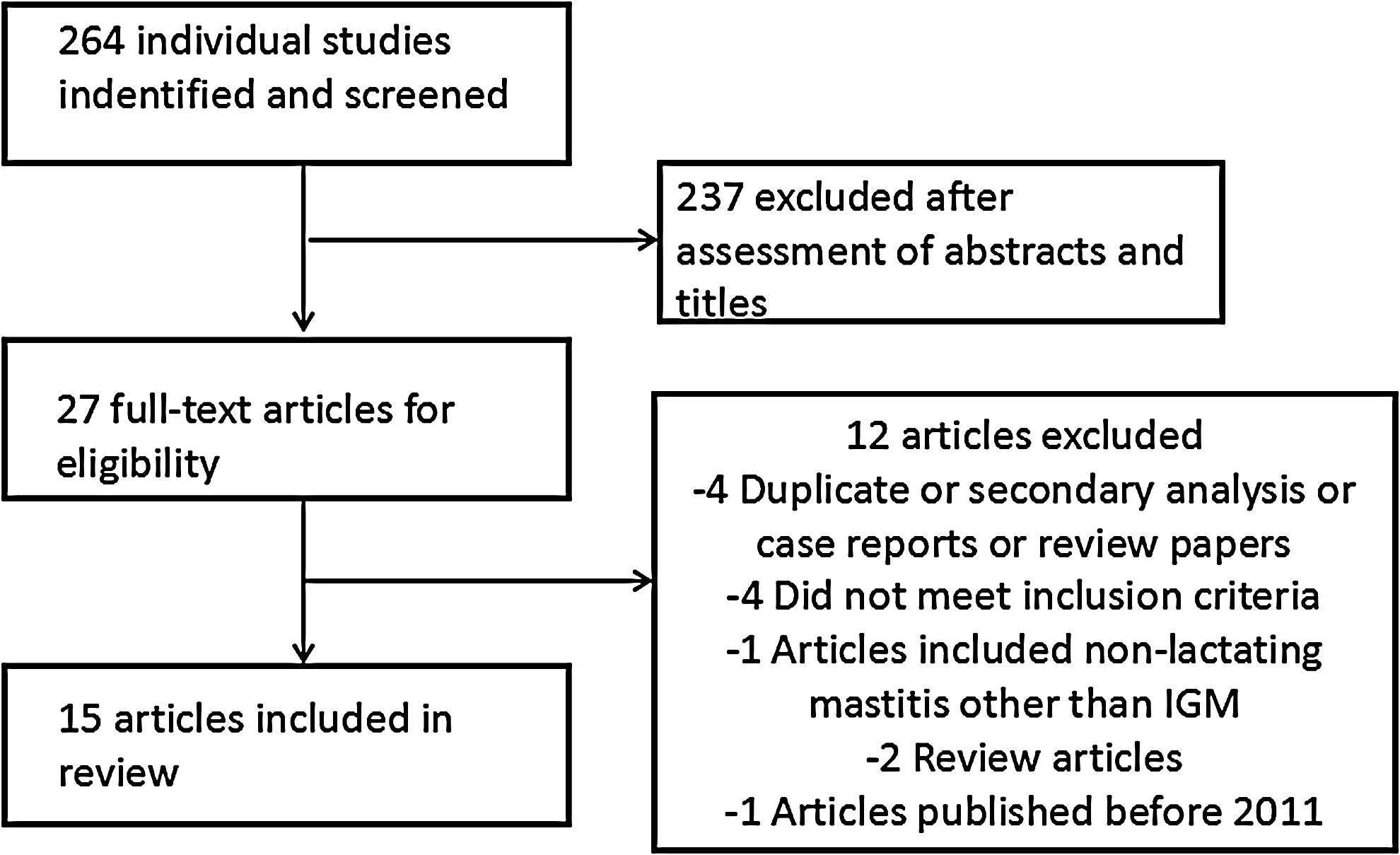
Flowchart for the systematic review.
No randomized control trial was found, and most studies were retrospective studies. The most common interventions used for IGM were steroids, surgical managements, and steroids combined with surgical managements. Two studies 15 did not report CR rate, and seven studies20,23,27 did not report recurrence rate. Follow-up period varied ranging from 1 month to 28 years (Table 1).
CR, complete remission/resolution; MTX, methotrexate; IGM, idiopathic granulomatous mastitis; IMAJ, the Israel Medical Association Journal; JKSS, Journal of the Korean Surgical Society; NA, not available.
CR rate and recurrence rate of IGM patients treated with surgical managements
Five14,18,19,25,27 studies (n = 85) reported the CR rate of IGM patients treated with surgical managements. Three18,19,25 of these five studies reported CR rate as 100%, and the other two studies had a CR rate of 88.9% 14 and 61.5%, 27 respectively (Table 1). We calculated a pooled estimate for CR rate of surgical managements of 90.6% (95% CI 83.8%, 95.7%) (Table 2). Six studies14,15,18,19,25,27 (n = 138) reported the recurrent rate of IGM treated with surgical managements, which ranged from 0%19,25 to 22.2%. 14 The meta-analysis of the incidence revealed an overall estimate of 6.8% (95% CI 3.3%, 11.5%) (Table 3).
CI, confidence interval; NA, not available.
NA, not available.
CR rate and recurrence rate of IGM patients treated with oral steroids
Nine (n = 358)12,14,17,19,20,23–27 and seven (n = 344)12,14,17,19,20,24,25 studies reported the CR rate and recurrent rate of IGM patients treated with oral steroids, respectively. The CR rates ranged from 30.8% 27 to 100.0%,23,26 and recurrent rate ranged from 0.0% 26 to 46.2% 14 (Table 1). The pooled estimates for CR rate and recurrent rate of steroids were 71.8% (95% CI 67.1%, 76.3%) (Table 2) and 20.9% (95% CI 9.2%, 16.1%) (Table 3), respectively.
CR rate and recurrence rate of IGM patients treated with oral steroids+surgical managements
Four (n = 85)13,17,20,27 and five studies (n = 106)13,15,17,20,27 reported the CR rate and recurrence rate of IGM patients treated with oral steroids with surgical managements, respectively. Three studies13,17,20 reported CR rate of 100%, and the fourth study 27 reported CR rate of 56.0%. Also, the recurrence rate was 0.0% in two studies15,20 and 5.0%, 13 9.0%, 17 and 11.0% 27 in the other three studies13,17 (Table 1). Furthermore, the meta-analysis of the CR rate and recurrence rate revealed overall estimates of 94.5% (95% CI 88.9%, 98.3%) and 4.0% (95% CI 1.5%, 8.4%), respectively (Table 3).
CR rate and recurrence rate of IGM patients treated with topical steroids
Two studies (n = 39)16,21 reported CR rate and recurrent rate of IGM patients treated with topical steroids. Both reported CR rate of 100%. The pooled estimate for CR rate of topical steroids was 98.8% (95% CI 93.3%, 99.8%) (Table 2). The recurrent rates were 10.7% 21 and 18.2%, 16 respectively (Table 1). The pooled estimate for recurrence rate of IGM treated with topical steroids was 14.3% (95% CI 5.4%, 26.6%) (Table 3).
CR rate and recurrence rate of IGM patients treated with observation
Four studies19,22,23,27 (n = 42) reported the CR rate of IGM patients treated with observation, and two of them (n = 30)19,22 reported the recurrence rate. The CR rate ranged from 75.0% 23 to 100%,19, 22 and the recurrence rate ranged from 0.0% 19 to 11.1%, 22 respectively (Table 1). The pooled estimates for CR rate and recurrence rate of IGM treated with observation were 95.1% (95% CI 87.0%, 99.4%) (Table 2) and 9.2% (95% CI 2.4%, 19.9%) (Table 3), respectively.
CR rate and recurrence rate of IGM patients treated with oral steroids+MTX
Three studies (n = 69)20,23,24 reported the CR rate of IGM patients treated with oral steroids and MTX. In Keren Mahlab–Gur's study, 23 only one patient treated with steroids and MTX was included, with the result of partial remission. Aghajanzadeh et al. 20 and Sheybani et al. 24 reported CR rate of 71.0% and 83.3%, respectively (Table 1). The pooled estimate for CR rate was 71.4% (95% CI 60.5%, 81.2%) (Table 2). Only in the study conducted by Sheybani et al. 24 (n = 12), the recurrence rate was reported. In their study, no patients treated with oral steroids with MTX showed recurrence (Table 1).
CR rate and recurrence rate of IGM patients treated with oral steroids+prolactin lowering agent
Only one study (n = 16) 20 included in our analysis reported the CR rate of IGM patients treated with oral steroids with prolactin lowering agent. The CR rate was 31.3%, but the recurrence rate was not available (Table 1).
Discussion
The primary treatments of IGM include steroids, surgical managements, MTX, and/or observations alone, based on the reported studies. However, there has been no consensus or guideline on the optimal treatment of this disease so far. No randomized clinical trials have been conducted on IGM, based on our knowledge, and most of the reported studies are retrospective, with varied efficacies of different treatments. Therefore, it would be important to know which treatment may have the best therapeutic efficacy. Our study was the first, based on our knowledge, to calculate the pooled estimated incidence for the complete remission/resolution rate and recurrence rate of different treatments for IGM. In general, we noticed that topical steroids, observation, oral steroids+surgical managements had the highest pooled CR rates of 98.8%, 95.1%, and 94.5%, respectively, whereas oral steroids and oral steroids+MTX had the lowest pooled CR rates of 71.8% and 71.4%, respectively. Only the pooled recurrence rates for oral steroids and topical steroids were >10%.
In our study, we found that surgical managements with or without oral steroids achieved a high CR rate and low recurrence rate. It is not surprising that surgical removal of the lesions is the most direct and efficient way to achieve CR. In Yabanoglu's study, 25 the average recovery period was 1.53 ± 0.67 months. In Hur's study, 27 the average recovery period was only 11.5 ± 9.2 days. Short time to achieve CR usually indicates quicker recovery to normal life and better quality of life. Meanwhile, the recurrence rates were 4.0% and 6.8% for surgical managements with and without oral steroids, respectively, suggesting its high efficacy for disease control. Taken together, surgical managements seem to be the best treatment for IGM. However, surgical procedures may cause stress and fear to patients, and sometimes might not be cost-effective. The potential of getting scars and/or asymmetry after surgical procedures may raise concern for some patients. Hence, patients may seek for more conservative treatments in practices. Oral steroids is one of the alternative treatments for IGM and is the most popular treatment to our knowledge. Our study showed that the pooled CR rate of oral steroids (71.8%) was much lower than that of surgical managements (90.6%) and oral steroids+surgical managements (94.5%), and the pooled recurrence rate of oral steroids (20.9%) was higher than that of surgical managements (6.8%) and oral steroids+surgical managements (4.0%). In addition, the recovery period of oral steroids was much longer when compared to surgical managements. In Yabanoglu's study, 25 the average recovery period was 5.21 ± 2.01 months. In Pandey's study, 19 it took an average of 5.3 months for patients to have complete remission. Hence, to avoid surgery, oral steroid is a valid alternative treatment method for IGM. However, patients need to be informed about its disadvantages, such as unknown optimal dose and regimen, longer period of time to achieve CR and higher recurrence rate. The potential adverse effects such as Cushing's syndrome, weight gain, osteoporosis, and glucose intolerance 5,15,20 should also be addressed during the decision-making.
IGM is mostly seen in young women in the child-bearing period, 28 and thus, the symptoms and complications of IGM and its treatments may affect patients' lactation in the future. IGM may cause nipple inversion, nipple retraction, sinuses, parenchymal distortion, scar formation, all of which may compromise a woman's lactation. One of the most common treatments for IGM is surgery,14,18,19,25,27 it requires removal of part or all of the breast tissue, which can also affect breastfeeding in the future. However, oral steroids alone such as prednisone and its metabolite are considered to be compatible with breastfeeding.29,30
In the scenario of malignant diseases such as breast cancer, the most important factors to consider when conducting a research and determining the optimal treatment are time to response, response rate, and local and systemic control rate. However, this might not always be the case in the setting of IGM treatment. The role of recurrence for predicting prognosis was different between IGM and malignant diseases. Recurrence of IGM after treatment may only compromise the quality of life, but not survival. Hence, the patients' preferences and complications need to be considered during decision-making. For patients who prioritized the cosmetic outcome of the breast, oral steroids, as a more conservative treatment, should be considered or recommended, rather than surgical managements. Topical steroids and observation might also be presented as treatment options to the patients. However, as the number of studies and sample sizes of these two treatments was limited and follow-up periods were short, we should be more cautious when making such recommendations.
Limitations and expectations
Several limitations need to be addressed. First, there was no standard definition of complete remission/resolution of IGM. In Pandey's study, 19 CR was defined as absence of pain, swelling, erythema, tenderness, and lump after treatment. In Sheybani's study, 24 the definition of CR was decreased pain, swelling, and tenderness, and disappearance of sinus tracts and pus. And in Altintoprak's study, 21 CR was defined as skin changes were completely ameliorated, complete disappearance of inflammatory signs in the affected breast, inactivity of fistulas, close of the fistula orifices, and/or skin erosions. And in some studies,13–18,20,22,25,27 the definition of CR was not clearly stated. Different definitions of CR may lead to different conclusions. As shown in a study by Sakurai et al., 26 the median time to disappearance of pain, palpable mass, and ultrasound and MRI findings was 2, 5, 8, and 7 months, respectively. Hence, calculating pooled CR rate from different studies, without a standard definition, may not be accurate.
Second, some treatments may be more appropriate than others according to patients' clinical manifestations. According to our study, observation alone could have a 95.1% CR rate with only 9.2% recurrence. As IGM is a self-limited disease that may resolve spontaneously without any treatment, 22 some patients may be managed only by observation. Needle aspiration or drainage could be considered for patients with abscesses. For patients with localized lesions such as masses, surgical excision could be considered. For patients with more severe symptoms, such as extensive breast swelling and/or inflammatory changes of the skin, oral steroids therapy could be the initiated treatment. Therefore, it may be more appropriate to manage IGM patients with different clinical manifestations with different treatments. However, this cannot be further addressed in this study.
Third, several technical limitations of this study were noticed. For example, only studies reported in English were included. We did not perform a quality analysis of the eligible studies, as most of them were retrospective. We did not have any data regarding the effect of IGM and its varied therapies on breastfeeding. In addition, the sample sizes of the included studies were small and varied. Finally, our study obtained the pooled CR rates and recurrence rates of each treatment method, and therefore, we cannot statistically compare rates between different treatment methods.
Conclusion
IGM is a benign breast disease with unknown etiology and there is no consensus on the optimal treatments. Our study showed that surgical management was able to achieve CR in most patients, with low recurrence rate, which was suitable for patients requiring rapid remission. Oral steroids were also acceptable as an alternative, a conservative treatment for patients with concerns about surgical scarring. However, patients should be fully informed about the relatively lower CR rate and slightly higher recurrence rate. The number of studies and sample sizes was not sufficient to support the use of topical steroids, oral steroids+MTX, and observation.
More studies are still needed to address the following questions: (1) whether IGM patients with different clinical manifestations need different treatments, (2) what is the standard definition of complete remission/resolution, (3) what would be the appropriate endpoints for studies of IGM, shall it be complete remission rate, recurrence rate, or quality of life, and (4) what is the optimal timing and sequence of combining interventions?
Authors' Contributions
Each author certifies that he or she has made a direct and substantial contribution to the work reported in the article.
Xin Lei, conceiving and designing the study; collecting and analyzing the data; and writing the manuscript.
Kai chen, conceiving and designing the study; analyzing the data; and writing the manuscript.
Liling Zhu, collecting the data and writing the manuscript.
Erwei Song, providing critical revisions that are important for the intellectual content and ensuring the accuracy and integrity of the study.
Fengxi Su, conceiving and designing the study; providing critical revisions that are important for the intellectual content; and approving the final version of the manuscript.
Shunrong Li, conceiving and designing the study; providing critical revisions that are important for the intellectual content; and approving the final version of the manuscript.
Footnotes
Acknowledgments
All authors had full access to the original guidelines and consensuses and have accepted responsibility for the data analysis. This study was supported by the National Natural Science Foundation of China (Grant#81402201/81372817) and the National Natural Science Foundation of Guangdong Province (Grant#2014A030310070). We appreciated the statistical advices from Yilong Education, Inc.
The study sponsor had no role in the study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding authors had full access to the data in the study and had final responsibility for the decision to submit for publication.
All relevant data are within the article and its supporting information files.
Disclosure Statement
All authors declare that they have no potential conflicts of interest.