
Abstract
Abstract
Objective:
To assess the influence of neonatal intensive care units (NICUs) on feeding practices at discharge of Portuguese very preterm infants.
Materials and Methods:
We analyzed data from 580 very preterm infants (<32 gestational weeks) discharged home from NICUs of two Portuguese regions and enrolled during 2011–2012 in Effective Perinatal Intensive Care in Europe population-based cohort. Maternal and infant characteristics were abstracted from medical records, and heads of NICUs provided the units characteristics. Feeding at discharge was classified as exclusive formula, exclusive breast milk or mixed, and differences among NICUs were obtained by comparison with pooled geometric mean odds of all NICUs, using multinomial logistic regression. Median odds ratios (MOR) were calculated to quantify variability among NICUs using multilevel logistic regression.
Results:
At discharge, 25.2% very preterm infants were exclusively on breast milk, 34.1% exclusively on formula, and 40.7% had mixed feeding, with a wide variation among NICUs. Exclusive breast milk increased in NICUs that had higher numbers of admissions, provided parents eating facilities, and by having designated members to support mothers who were breastfeeding. The individual NICU odds of mixed versus exclusive formula feeding ranged from 0.36 to 2.07 and for exclusive breast milk versus exclusive formula ranged from 0.16 and 5.11. Adjusting for individual and unit characteristics, heterogeneity across NICUs remained evident, being the MOR 1.33 for mixed feeding and 1.35 for exclusive breast milk.
Conclusions:
NICUs influence feeding practices independently of individual characteristics, highlighting the importance of institution-based interventions to promote breast milk.
Introduction
T
Moreover, across Europe, there is a large variation in breast milk feeding, despite current clinical guidelines and public health policy. 7 The MOSAIC study documented a large variation in breast milk feeding at discharge among very preterm infants in eight European regions in 2003, ranging from 19% in Burgundy (France) to 70% in Lazio (Italy), and showed a significant positive correlation with the national rates of breastfeeding for all infants. 3 In that study, 50% of Portuguese very preterm infants were discharged on breast milk (6% exclusive and 44% mixed). 3
Available research has shown that mothers who were not married,8,9 younger,3,8,9 of a lower social class,10,11 smokers, 10 multiparous, 3 and not attending prenatal care 12 were less likely to provide breast milk to their infants. Infants with lower gestational age,3,9 lower birth weight, 3 bronchopulmonary dysplasia, 3 and longer hospital stay 13 were less likely to be fed with breast milk.
Significant variations in the prevalence of breast milk feeding have also been observed among neonatal intensive care units (NICUs),9,12–15 which could reflect suboptimal use of evidence-based care, 16 with different attitudes and practices operating locally and influencing the initiation and maintenance of breast milk feeding beyond individual factors.17,18 One previous study showed that NICUs with better work environments, educated nurses, and providing breastfeeding support by nurses have higher rates of infants discharged on human milk. 15
Thus, we aimed to assess the influence of NICUs characteristics on feeding practices at discharge among Portuguese very preterm infants.
Materials and Methods
Study design and participants
Data were collected as part of the Portuguese participation in the study Effective Perinatal Intensive Care in Europe (EPICE), that recruited a population-based prospective cohort of very preterm infants (22–31 completed weeks of gestational age) born in 2011–2012, in 19 European regions. 16
In Portugal, all 724 very preterm live births that occurred between June 2011 and May 2012 in the two participating regions—North and Lisbon and Tagus Valley—were documented. 19 For analysis, only infants born in public maternity units (n = 703) and discharged home were considered (n = 581; 115 infants died and 7 infants were discharged to institutions). Infants were admitted to the NICU where they spent their first consecutive 48 hours of life. 3 We excluded one NICU with a single admission over the study period. The final sample comprised 580 infants admitted to 16 NICUs, with a median infants per unit of 29 (range 6–112).
Data collection
Data on maternal, pregnancy, infant, and clinical characteristics were abstracted from medical records by local healthcare professionals, using a pretested standardized questionnaire, 19 and later verified by the research team.
Data on NICU characteristics were obtained using a structured questionnaire, completed by the head of the unit or a coworker(s), to assess information about how the care of very preterm infants was organized in the unit, including questions about admissions and activity, services and equipment, staffing, protocols/guidelines, and perinatal practices.
Outcome
Feeding practices at discharge were classified in three categories: exclusive formula (no breast milk); exclusive breast milk (receiving only maternal breast milk, without differentiating between mother's own milk and donor milk); or mixed (a combination of breast milk and formula). Breast milk was considered regardless of the feeding method: directly from the breast, bottle, tube, or cup.
Individual-level variables
Gestational age was based on the best estimate of the obstetrical team, using information on ultrasound measures and the last menstrual period. Maternal hypertensive disorders comprised chronic hypertension, gestational hypertension, preeclampsia, eclampsia, or HELLP syndrome. Bronchopulmonary dysplasia was defined as oxygen dependence or respiratory support (including nasal cannula, nasal continuous positive airway pressure, or mechanical ventilation) at 36 weeks of postmenstrual age. Severe brain injury was considered when there was a diagnosis of intraventricular hemorrhage grades III or IV using the classification defined by Papile et al. 20 and/or cystic periventricular leukomalacia, which was recorded only if cystic abnormalities were present on ultrasound or CT scan. Necrotizing enterocolitis was considered if stage II or III of Bell's classification was verified. Congenital anomalies included major congenital anomalies at birth and/or minor congenital anomalies defined as those considered reportable to EUROCAT. 21
Portuguese infants were georeferenced according to their home address using the ArcGIS Online World Geocoding Service and Google Maps, and it was possible to do so accurately for 574 (99.0%) infants. Neighborhood socioeconomic deprivation was assessed using the European Deprivation Index (EDI), used to classify small areas according to their level of socioeconomic deprivation. 22 The EDI classes were attributed to participants using ArcGIS version 10.4.1 by a point-in-polygon overlay operation. The EDI score was categorized in quintiles of increasing deprivation (1-least to 5-most deprived). The EDIs of England, Spain, and France were used for the four participants who resided in these countries. No EDI quintile could be attributed to two participants: one residing in Scotland and another in Angola. More details about the formula of EDI construction in those countries are reported elsewhere. 22
Neonatal unit-level variables
The unit variables were selected based on previous research showing the characteristics that could potentially influence the breast milk feeding outcomes23,24 and on the characteristics supporting family-centered care and family–friendly environment approaches.18,25,26 Thus, the unit variables covered four specific NICUs characteristics: (1) general aspects of the NICU (e.g., number of admissions, level of care); (2) policies toward parents (e.g., kangaroo care, parents were allowed to spend the night in the NICU); (3) facilities available in the intensive care unit area (e.g., a room for parents to relax and talk, a room specifically for breast milk expression and/or breastfeeding); and (4) breastfeeding-related characteristics (e.g., Baby-Friendly Hospital Initiative accreditation, written protocol available).
As the specialization of units by level of care varies internationally, we categorized it as level II and III, according to Portuguese guidelines, which consider the hospital services and grade, being level II defined as medium intensive care (often termed “perinatal support unit”) and level III as high-intensive care (often termed “differentiated perinatal support unit”). Baby-Friendly Hospital Initiative accreditation 27 variable was categorized as: (1) no accreditation; (2) in process of accreditation; and (3) maternity unit or both maternity and neonatal units accredited.
The variable “designated staff in the unit to support mothers expressing or breastfeeding” was considered if the unit had a healthcare professional with certified training in breastfeeding/lactation (e.g., lactation consultant/feeding coordinator) available, whose role is supporting mothers expressing or breastfeeding. Kangaroo care policies were based on the opportunity offered by the unit for parents to hold their baby close to their chest, skin-to-skin, categorized as offered routinely, sometimes, only on request, or generally no, and were recorded separately for mothers and fathers.
Ethical approval
The study was approved by the Portuguese Data Protection Authority (authorization 7426/2011) and by the Ethics Committee of each participating hospital.
Statistical analysis
Feeding practices at discharge by NICU were compared with the proportions in the whole sample, using the Chi-square goodness of fit test or the Fisher exact test, as appropriate. To evaluate differences among NICUs, we compared each NICU with the overall effect obtained as the pooled geometric mean odds of all NICUs, using the deviation contrast method. 28 Crude odds ratios (OR) and respective 95% confidence intervals were estimated using multinomial logistic regression, comparing mixed versus exclusive formula and exclusive breast milk versus exclusive formula, considering that the outcome has three categories.
Feeding practices at discharge by maternal, infant, and NICUs characteristics were described as counts and proportions for categorical variables, and median and 25–75 percentiles (P25–P75) for continuous variables. Proportions were compared using the Chi-square test and medians using the Kruskal–Wallis test for individual characteristics.
Multilevel mixed-effects multinomial logistic regression was fitted for each NICU characteristic with a random effect by NICU. The likelihood ratio test was used to compare the model with and without each NICU characteristic to evaluate the respective association with feeding practices at discharge. This comparison was provided if at least 2 of the 16 NICUs displayed each category of the characteristic considered.
A median odds ratio (MOR) was calculated to quantify the magnitude of variability, and can be conceptually described as quantifying the variation between clusters (second-level variation) by comparing two individuals from two randomly chosen different clusters. Thus, considering two infants with the same covariates, chosen randomly from two different NICUs, the MOR is the median value of the OR between the infant in the NICU with the highest breast milk feeding proportion and the infant in the NICU with the lowest breast milk feeding proportion. The MOR is equal to 1 (meaning no differences between clusters) or greater, and a greater variation between NICUs results in a larger MOR.29,30
We first estimated a null model, which only included a random intercept without any exposure variables. Then, we included maternal and infant characteristics in the model (Model 1) to assess the extent to which variability between NICUs was explained by individual characteristics. Afterward, additional models were computed incorporating each specific group of NICU characteristics as a block: (1) general aspects; (2) policies toward parents; (3) facilities available in the intensive care unit area; and (4) breastfeeding-related characteristics. NICUs characteristics included in each block were only the ones that were strongly associated with the variance between NICUs based on interval odds ratio (IOR) estimations calculated for each NICU characteristic (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/bfm). The IOR was defined as the interval centered on the median of the distribution comprising 80% of the values of the odds ratio (IOR-80). If the interval does not contain the value 1, it indicates that the effect of the NICU characteristic considered accounts for a strong amount of the variance between NICUs. 30
We calculated the relative increase of the variance between NICUs when moving from τ0(1) to τ0(2) [(τ0(1)−τ0(2)/(τ0(1))], where τ0(1) and τ0(2) were the variance of random effects of Model 1 and of each other model, respectively. The proportion of explained variance corresponds to the proportion of between-NICUs variance that could be explained by the variables selected. It is negative when the variance between NICUs increases, and it is positive when the difference decreases after adjustment. To evaluate how NICUs characteristics influence the variability between units independently of the individual level, we established the model adjusted for individual characteristics as the reference.
Analysis was performed using STATA 14.0 software (Stata Corporation, College Station, TX) or R version 3.2.3 using the MASS package.
Results
Feeding at hospital discharge was 25.2% exclusive breast milk, 34.1% exclusive formula, and 40.7% mixed feeding. As shown in Figure 1, feeding practices at discharge varied significantly among Portuguese NICUs, ranging from 3.3% to 50.0% for exclusive breast milk, 16.7–50.9% for exclusive formula, and from 21.4% to 61.5% for mixed feeding. Six of the 16 NICUs presented proportions of feeding practices significantly different from those observed in the total sample, but the two Portuguese regions, although they are administered by separate health authorities, presented similar results (26.7% North versus 24.0% Lisbon and Tagus Valley for exclusive breast milk; 43.3% North versus 38.7% Lisbon and Tagus Valley for mixed).
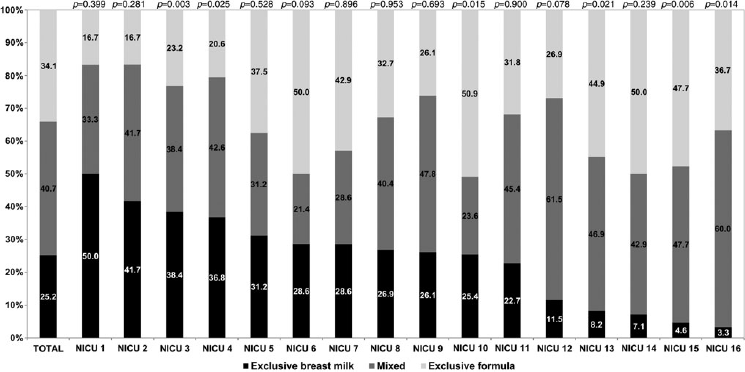
Distribution of feeding practices at discharge in very preterm infants, by NICU, Portugal, 2011–2012. p-Values for the comparison of each unit with the total sample. If there was a transfer, infants were assigned to the NICU where they spent the first 48 hours of life. NICU, neonatal intensive care unit.
The individual NICU odds of mixed versus exclusive formula feeding compared with the pooled geometric mean odds are presented in Table 1 and ranged from 0.36 to 2.07 showing a wide heterogeneity. For 2 of the 16 NICUs, the differences were statistically significant. The odds for exclusive breast milk versus exclusive formula varied between 0.16 and 5.11 showing an even wider heterogeneity, with four NICUs being significantly different from the pooled geometric mean odds.
A comparison of each individual NICU with the total sample. NICUs (where infants spent their first consecutive 48 hours of life). Reference class: Each NICU was compared to the overall effect obtained as the pooled geometric mean odds of all NICUs odds.
NICU, neonatal intensive care unit; OR, odds ratio; 95% CI, 95% confidence interval.
Table 2 summarizes feeding practices at discharge according to maternal and infant characteristics. The median length of hospital stay was greater in infants who received exclusive formula (64 days, P25: 47 − P75: 92; versus 47 days for mixed, P25: 34.5 − P75: 63; versus 46 days for exclusive breast milk, P25: 34 − P75: 63, p < 0.001).
In each variable, the total may not add up to 580 due to missing data.
NICU, neonatal intensive care unit.
Table 3 shows the prevalence of feeding practices at discharge considering NICU characteristics. In general, the units were very similar regarding the evaluated items. For example, all units allowed parents to stay with their baby as much as they wanted in each visit and routinely offered kangaroo care to the mother. Only one NICU reported to offer kangaroo care to the father sometimes. However, infants who were hospitalized in NICUs, which had a designated staff member to support mothers expressing or breastfeeding, had higher proportions of exclusive breast milk (30.7% versus 10.3%, p < 0.001), as was the case for NICUs that provided facilities for parents to heat food and/or make drinks (30.3% versus 15.9%, p = 0.002). On the contrary, infants who were hospitalized in NICUs, which provided a bathroom with a shower for parents, had lower proportions of exclusive breast milk (17.9% versus 32.4%, p < 0.001). NICUs that had higher numbers of admissions in 2011 presented higher proportions of exclusive breast milk (29.4% for ≥350 admissions versus 18.6% for <350, p = 0.032). Two NICUs reported use of human bank milk/donor's milk, one offered milk to infants with less than 32 gestational weeks and the other only to infants with less than 28 weeks.
NICUs (where infants spent their first consecutive 48 hours of life).
p-Values corresponding to the results of the likelihood ratio test using multilevel mixed-effects multinomial logistic regression with a random effect by NICUs.
NICU, neonatal intensive care unit.
Table 4 provides results from the random intercept model. After adjustment on maternal and infants characteristics, the MOR comparing mixed feeding with exclusive formula was 1.62, showing significant variation between NICUs. These variations decreased in Model 2 (1.55) and achieved a higher effect in Model 3 by adding the variable bathroom with a shower for parents (1.35), with an explained variance of 60.0%, without further changes, resulting from the addition of designated staff member to support mothers expressing or breastfeeding to Model 4 (1.33). When comparing exclusive breast milk with exclusive formula, the MOR results adjusted for maternal and infant characteristics revealed larger heterogeneity across NICUs (2.38). In Model 2, the variability between NICUs decreased to 2.23, a change associated with an explained variance of 11.5%. In Model 3, the additional adjustment resulted in an attenuation of the MOR estimate (1.88) with an explained variance that increased to 44.9%. Finally, we obtained 87.5% of the explained variation by adding the variable designated staff to support mothers expressing or breastfeeding (MOR = 1.35).
Model 0 is a null model, baseline model without any exposure variable.
Model 1 is adjusted for maternal age, multiple pregnancy, antenatal steroids, gestational age, birth weight, apgar score, congenital anomaly, bronchopulmonary dysplasia, early infection, late infection, any surgery, and number of transfers between NICUs.
Model 2 is additionally adjusted for parents may stay during ward rounds.
Model 3 is additionally adjusted for bathroom with a shower for parents.
Model 4 is additionally adjusted for designated staff or other members in the unit to support mothers who were expressing or breastfeeding.
MOR, median odds ratio; NICU, neonatal intensive care unit.
Discussion
In this first large sample of Portuguese very preterm infants representing approximately two-thirds of the national very preterm births during the study period, the overall prevalence of any breast milk feeding at discharge was 65.9%, ranging from 49.0% to 83.4%, and of exclusive breast milk 25.2%, ranging from 3.3% to 50.0% across units. We found differences across NICUs, suggesting that unit characteristics are probably more important than available national orientations for breast milk feeding. Moreover, results from the adjusted MOR provided strong evidence for the observed heterogeneity across NICUs. Differences of this magnitude across units have also been found in other countries. Exclusive breast milk feeding at discharge varied significantly between units from 53% to 83% in a prospective Danish cohort of preterm infants. 14 The proportion of high-risk infants fed with exclusive human milk (mother's or donor's milk) varied from 0% to 60% across centers in Italy. 13 In the United States, variations from 35% to 71% were recorded comparing low use with high-use sites across the country, 9 or hospital risk-adjusted rates of breast milk feeding that ranged from 19.7% to 100% in California. 12
It is considered critical to avoid mother–infant separation, by promoting early, prolonged, and continued skin-to-skin contact (kangaroo care). 31 A previous qualitative study, with mothers and fathers of preterm infants, identified the supportive factors and barriers for their performance of kangaroo care: parent-related factors, time, infants-related factors, and the NICU and home environment. 32 In our regions, all units provided unlimited visit duration throughout visitation, which was 24 hours for 11 of the 16 units, and 12 hours during the day for 3. Also, all NICUs routinely provided kangaroo care to mothers and 15 NICUs to fathers. Thus, per se, these factors cannot contribute much to the variation between units. However, maternity leaves in Portugal might not be fully paid if hospitalization periods are long and commuting from home to the NICU is not covered by social security, a difficulty confronted by many parents who have to travel long distances as a result of regionalization of care. Logistics and economic constraints may thus render parental visits rather challenging and increase the probability of mother–infant separation. 33 As we did not evaluate the actual length of parental presence and skin-to-skin contact in the NICU, this potential individual source of variability could not be addressed.
An appropriately trained health staff, with certified education and training in breastfeeding, has been shown to play a key role in NICUs for successfully establishing breast milk feeding, supporting mothers, informing about benefits and clarifying doubts, and helping to initiate and maintain lactation.15,33–35 In our study, five NICUs had no designated staff member to support mothers expressing or breastfeeding, and they presented the lowest prevalence of exclusive breast milk. When we evaluated feeding practices using a random intercept model, this staff-related characteristic explained per se the largest proportion of variance (42.6%), being a major determinant of exclusive breast milk feeding. Considering that in Portugal the population is served by a universal and free maternal and child health system whose professionals follow a nationally defined standard training, we did not expect such heterogeneity of the NICUs. It is important to consider the personal experience, beliefs, attitudes, and involvement of professionals17,36 as a major source of information, guidance, assurance, and support to parents, 37 but no such information was collected in the present study.
Parents are also key actors for successful breast milk feeding. A systematic review of studies describing their views showed that knowledge about infant's and women's bodies and behaviors, reinforcement of mother's motivation, and alignment between NICUs routines and parents' needs are essential. 38 In Portugal, concerns related to inadequate milk supply, difficulties with expressing breast milk, and physical separation from infants were identified by parents as major barriers to provide breast milk to very preterm infants in the NICU, while their knowledge about breastfeeding benefits was a major facilitator. 39 This supports the importance of family-centered care and a family–friendly environment in NICUs that incorporate parents' needs and stimulate their active participation in infants' care. 25 In the United Kingdom, a large variation within and across types of neonatal units was observed regarding indicators of family-centered care, namely facilities, information, and policies. 26 In our study, 13 NICUs provided a room specifically for breast milk expression and breastfeeding, but feeding practices were similar in the remaining units. Unexpectedly, we found that NICUs with a bathroom with a shower for parents had lower exclusive breast milk proportions. In fact, we did not evaluate the utilization of available facilities or what units were offering as resources, namely chairs near the infants' cots, equipment, and access to breast pumps. This type of information could provide a deeper understanding of the observed variability.17,18,25
Differences across NICUs can also be related to local regulations and adherence to guidelines, such as the management of mother's own milk for infants born very preterm regarding fresh versus pasteurized human milk, regular bacteriological analyses, or storage time.17,40 We found that 13 NICUs followed written protocols for breastfeeding and human milk use, 8 had their own, and 5 used regional, national, or network protocols, but feeding practices were similar. In Portugal, there is only one human milk bank serving two NICUs, making a meaningful comparison impossible. Although donor human milk is recommended when mother's milk is not available, this is not a possible alternative in Portuguese NICUs for infants whose mothers choose not to breastfeed or cannot do it. However, it is well established that human milk banks are an instrument for breastfeeding promotion and support. 41
The observed proportion of breast milk feeding at discharge in our study was higher than in 2003 in the North region of Portugal, 3 reflecting a regional increase in exclusive breast milk feeding from 6.0% to 26.7% for exclusive breast milk and 50.0% to 70.0% for any breast milk, probably following adherence to the Baby-Friendly Hospital accreditation. 27
It is known that maternal, obstetric, and infant clinical factors influence breast milk feeding in NICUs. However, our study suggests that NICUs influence feeding practices independently of individual characteristics. A study from the EPICE cohort, including units from all 19 European regions, found that infants cared at NICUs with a Baby-Friendly Hospital Initiative accreditation were more often on any breast milk feeding at discharge and that those admitted to NICUs with protocols for breast milk feeding and access to donor milk had higher proportions of exclusive breast milk feeding at discharge. 23 Because of the heterogeneity of units across regions, this study was unable to investigate the organizational characteristics of the units or measure unit-level variability, as we were able to do within the Portuguese sample. International studies are, however, appropriate for investigating characteristics that vary more widely at the regional level.
A major strength of our study is the use of high-quality data, collected within a population-based prospective cohort, under common protocols and research tools, covering all NICUs in the two largest Portuguese regions. To avoid unnecessary confounding, infants were attributed to the NICU, where they spent their first consecutive 48 hours of life, as breast milk feeding success depends on establishing lactation in the period immediately after birth. 3 To the best of our knowledge, this is the first study using the MOR, which allows a multilevel analysis of heterogeneity between units within the same level.
Limitations should also be acknowledged. We have no information about duration of breast milk feeding in hospital, making it impossible to consider a time dimension in the comparison of feeding at discharge. Some variables potentially useful to understand the findings were not available, namely maternal intention and motivations to breastfeed or the reasons for not initiation or stopping breastfeeding, such as mother's own choice, physiological or psychological reasons, and mother's milk is not available or is insufficient. Detailed sociodemographic characteristics would be also helpful. However, we georeferenced the infants and used a neighborhood socioeconomic deprivation index, a valid proxy of individual socioeconomic position, and we did not find statistically significant differences. 22
Conclusion
There was a significant variation in the prevalence of breast milk feeding of very preterm infants in Portuguese NICUs, independent of individual characteristics, and only partially explained by the evaluated NICUs' characteristics. This highlights the importance of a better understanding of the complex determinants of breast milk feeding among this specific group of vulnerable infants and the role of institution-based interventions to promote breast milk in NICUs as a component of healthcare quality.
Footnotes
Acknowledgments
The authors acknowledge all members of the staff in the Departments of Obstetrics and Neonatology from the participating hospitals. The authors thank Ana Isabel Ribeiro for her collaboration in georeferencing the infants and for computing the neighborhood socioeconomic deprivation index. This study was funded by the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement no. 259882. This study was also funded by FEDER through the Operational Programme Competitiveness and Internationalization and national funding from the Foundation for Science and Technology—FCT (Portuguese Ministry of Science, Technology and Higher Education), under the Unidade de Investigação em Epidemiologia—Instituto de Saúde Pública da Universidade do Porto (EPIUnit) (POCI-01-0145-FEDER-006862; Ref. UID/DTP/04750/2013); the PhD Grant SFRH/BD/111794/2015 (Carina Rodrigues); and the individual grant SFRH/BSAB/113778/2015 (Henrique Barros), cofunded by the FCT and the POCH/FSE Program.
Members of the EPICE-Portugal Network
Adelina Sá Couto, Aldina Lopes, Alexandra Almeida, Alexandrina Portela, Alice Vilas Boas, Almerinda Pereira, Ana Aroso, Ana Berdeja, Ana Bettencourt, Ana Campos, Ana Castilho Santos, Ana Isabel Machado, Ana Maria Andrade, Ana Melo Bento, Ana Neto, Ana Pita, Ana Rute Ferreira, Angelina Tavares, Anselmo Costa, Antónia Nazaré, António Braga, António Fonseca, António Lanhoso, António Vilarinho, Beatriz Sousa, Carla Sá, Carlos Moniz, Cármen Carvalho, Catarina Dâmaso, Célia Araújo, Clara Paz Dias, Cláudia Araújo, Conceição Casanova, Conceição Cunha, Conceição Faria Murinello, Conceição Telhado, Cristina Didelet, Cristina Leite, Cristina Martins, Cristina Trindade, Daniela Almeida, Domingos Jardim da Pena, Dulce Oliveira, Eduarda Reis, Eduardo Fernandes, Ester Casal, Eurico Gaspar, Fátima Fonseca, Fátima Romão, Fernanda Matos, Fernando Cirurgião, Filomena Nunes, Gabriela Pereira, Glória Carvalhosa, Graça Henriques, Gustavo Rodrigues, Helena Almeida, Helena Oliveira, Helena Sousa, Hercília Guimarães, Ilídio Quelhas, Isabel Canelas, Isabel Carolino Silva, Isabel Knoch, Isabel Martins, Jacinto Torres, Joana Saldanha, Joana Sampaio, João Mendes, Joaquim Marinho, Joaquina Baltazar, Jorge Ribeiro, Jorge Silva, José Amorim, José Furtado, José Guimarães, José Luís Fonseca, José Miguel Nogueira, José Oliveira, José Pombeiro, José Teixeira, Juan Calviño, Judite Marques, Lucília Araújo, Luís Caturra, Luís Graça, Maria do Carmo Serra, Maria do Céu Machado, Maria Paula Arteaga, Margarida Cabral, Margarida Pontes, Margarida Seabra, Maria Lurdes Pinho, Maria José Carneiro, Mário Furtado, Mário Paiva, Marisa Cabanas, Marta Aguiar, Marta Barbosa, Micaela Serelha, Nuno Montenegro, Olímpia do Carmo, Óscar Vaz, Osvaldo Soares, Paula Costa, Paula Pinheiro, Paula Soares, Pedro Rocha, Pedro Silva, Pedro Tiago, Raquel Maciel, Ricardo Mira, Rosa Rodrigues, Rosalina Barroso, Rosalinda Rodrigues, Rubina Mendonça, Rui Carrapato, Rui Costa, Rui Pinto, Sara Noéme Prado, Susana Gama de Sousa, Teresa Oliveira, Teresa Rodrigues, Teresa Teles, Teresa Tomé, Teresa Ventura, Valdemar Martins, Vítor Neves, and Zélia Nunes.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.