
Abstract
Abstract
Introduction:
Assessment of breastfeeding efficiency by objective means is essential to increase the success of breastfeeding.
Aims and Objectives:
To study the utility of LATCH score in predicting exclusive breastfeeding rates at 6 weeks postpartum along with an optimum cutoff between January 2016 and June 2016.
Materials and Methods:
One hundred mother–infant dyads born of vaginal delivery with gestational age ≥37 weeks and singleton births were included with LATCH scores assessed at birth and 48 hours/discharge and followed up at 6 weeks postpartum.
Results:
Sixty-two of 100 (62%) infants were exclusively breastfeeding at 6 weeks. Mean LATCH scores at birth (7.17 ± 1.13 versus 4.26 ± 1.7, p = <0.0001) and 48 hours/discharge (9.22 ± 1.01 versus 5.78 ± 1.29, p = <0.0001) were higher in mothers who were breastfeeding at 6 weeks. LATCH score ≥6 at birth had a sensitivity 93.5% and specificity 65.78% and these mothers were 5.92 times more likely to be breastfeeding at 6 weeks. LATCH score ≥8 at 48 hours/discharge had a sensitivity 93.55% and specificity 92.1% with these mothers being 9.28 times more likely to be breastfeeding at 6 weeks postpartum. Receiver operating characteristic (ROC) for LATCH score at birth and exclusive breastfeeding (EBF) at 6 weeks had an area under curve (AUC) 0.915 (cutoff ≥5.5 sensitivity 93.5%, false positive rate—34.2%). ROC for LATCH score at 48 hours/discharge and EBF 6 weeks had an AUC 0.979 (cutoff ≥7.5 sensitivity 93.5%, false positive rate—7.9%).
Conclusion:
LATCH represents a simple, cost-effective tool capable of predicting breastfeeding as early as in the first 24 hours of life, especially in resource-limited settings.
Introduction
T
Materials and Methods
This prospective cohort study took place in a tertiary care hospital in Chennai between January 2016 and June 2016 after approval from the institutional ethics committee (IRB-MCH/23/2016).
All the mother–infant dyads who underwent vaginal delivery during the study period were included in the study after consent. We included singleton births and babies ≥37 weeks gestation. Exclusion criteria were babies with APGAR score <7 at 5 minutes of life, babies requiring admission to the neonatal intensive care unit (NICU), and mothers who were sick and unable to breastfeed. Maternal and neonatal clinical details were collected from case sheets. The LATCH charting system (Fig. 1) assigns a numerical score (0, 1, or 2) to five key breastfeeding components identified by the letters of the acronym LATCH: “L” is for how well the infant latches onto the breast, “A” is for the amount of audible swallowing noted, “T” is for the mother's nipple type/condition, “C” is for the mother's level of comfort, and “H” is for the amount of help the mother needs to hold her infant to the breast. The total score ranges from 0 to 10, with the higher score representing successful breastfeeding (Table 1).
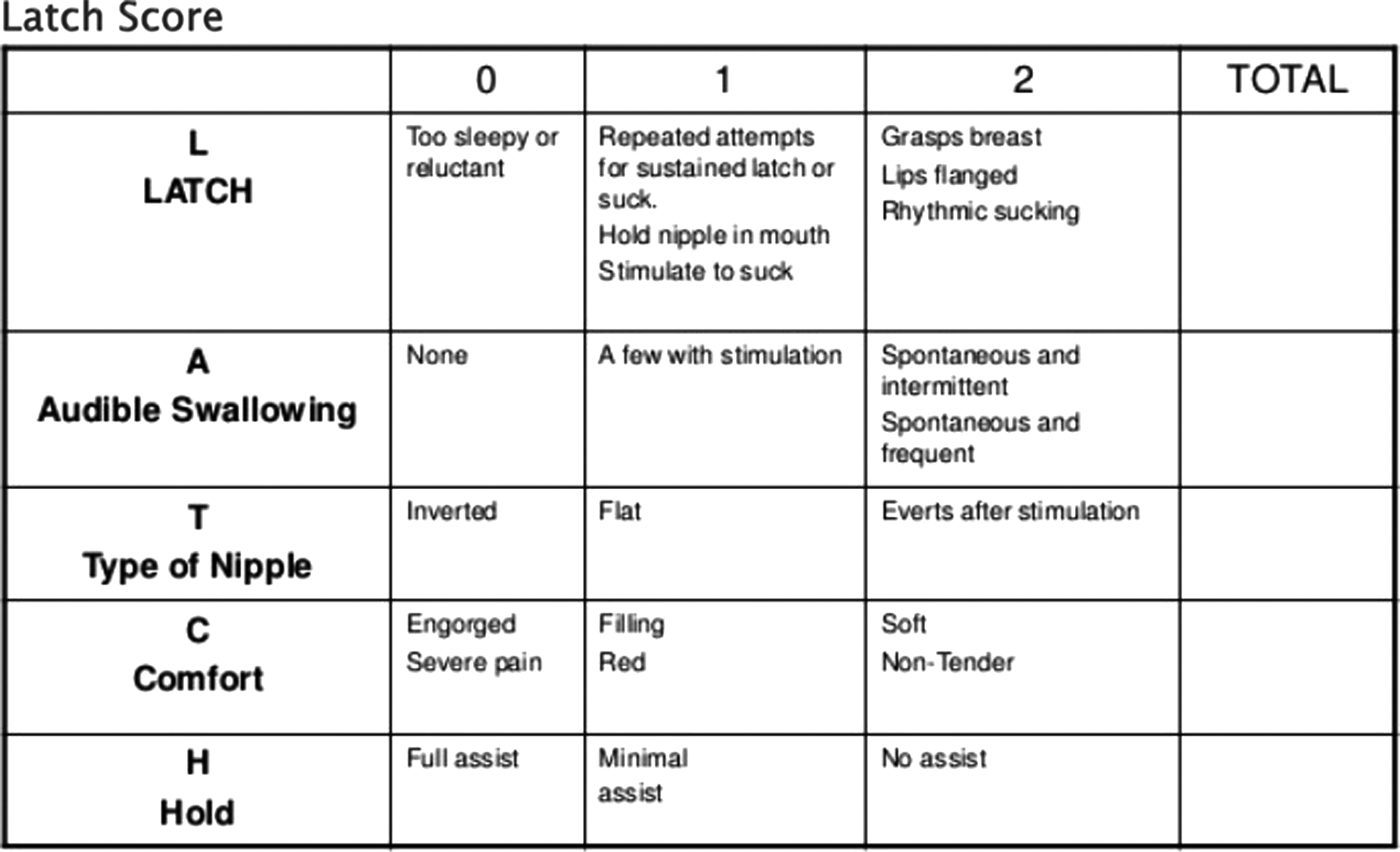
LATCH charting system.
An international board-certified lactation consultant trained the investigator, one labor delivery room (LDR) nurse, and two postpartum nurses in the use of LATCH tool. The time points of assessment were at birth and at 48 hours/discharge. The time given for the baby to LATCH was 10 minutes, that is, this was the time given before the scoring was done on the LATCH sheet. The staff nurse assessed the LATCH score for each mother–infant dyad. After giving birth, mother and baby stayed in the LDR for 1 hour. During this period, breastfeeding and skin-to-skin contact were attempted. LATCH assessment tool with individual scores was attached to the case sheets. To prevent interobserver variability in scoring LATCH tool, the trained staff nurses or the investigator in their absence scored the sheets. At 48 hours/discharge from the hospital, either of the two postpartum nurses or the investigator scored the LATCH tool and it was filed in the case sheet for future reference. We allowed at least 10 minutes time before scoring the sheets. The women who showed low LATCH scores at any point in our study were intervened by the lactation consultant as needed. Data were collected for the following variables: maternal age, gravidity, parity, socioeconomic status, level of education, type of family, place of residence, antenatal breastfeeding counseling, drugs used during labor, and contact number. For the newborn, birth weight, gestational age, and 1- and 5-minute Apgar scores were recorded. Based on definitions developed by Labbok and Krasovec, 8 we modified the definitions as “breastfeeding” when no other liquid or solid was given to the baby other than breast milk and as “not breastfeeding” when partial breastfeeding, that is, at least one or more feeds was a formula or no single breastfeed given at 6 weeks for the ease of application.
Statistical analysis
Baseline and outcome data were recorded in a predesigned proforma and a master chart was prepared in Microsoft Excel sheet. Descriptive analysis of the study sample was done. We conducted a bivariate analysis to study the relationship between maternal and newborn characteristics and exclusive breastfeeding at 6 weeks postpartum. Differences were evaluated with a chi square test for categorical variables and with an unpaired nonparametric Wilcoxon's test for continuous variables not distributed normally and student t-test for continuous variables distributed normally. Sensitivity and specificity for different LATCH score cutoffs at birth and at 48 hours/discharge were calculated (Table 2). Relative risk (RR) and confidence interval (95% CI) were calculated for LATCH cutoffs with highest sensitivity and specificity. Receiver operating characteristic (ROC) was constructed for LATCH score at birth and 48 hours/discharge to predict exclusive breastfeeding at 6 weeks. Sensitivity is the ability of a LATCH score at or above the threshold to predict whether a subject will be breastfeeding at 6 weeks. Specificity is the ability of a low LATCH score to predict that a participant will no longer be breastfeeding at 6 weeks. We used SPSS for Windows 19.0 for all calculations. p-Values 0.05 or less were considered statistically significant.
Results
Flowchart of enrollment and follow-up of participants are shown in Figure 2. The baseline characteristics of the whole study cohort are given in Table 3. The mean maternal age was 28.96 ± 3.35 years. Mean birth weight and gestational age of the infants were 3.007 ± 0.38 kg and 38.61 ± 1.04 weeks. A total of 62% of the mother–infant dyads were exclusively breastfeeding at 6 weeks postpartum. We compared the subject characteristics among women exclusively breastfeeding at 6 weeks postpartum and those who had weaned (Table 4).
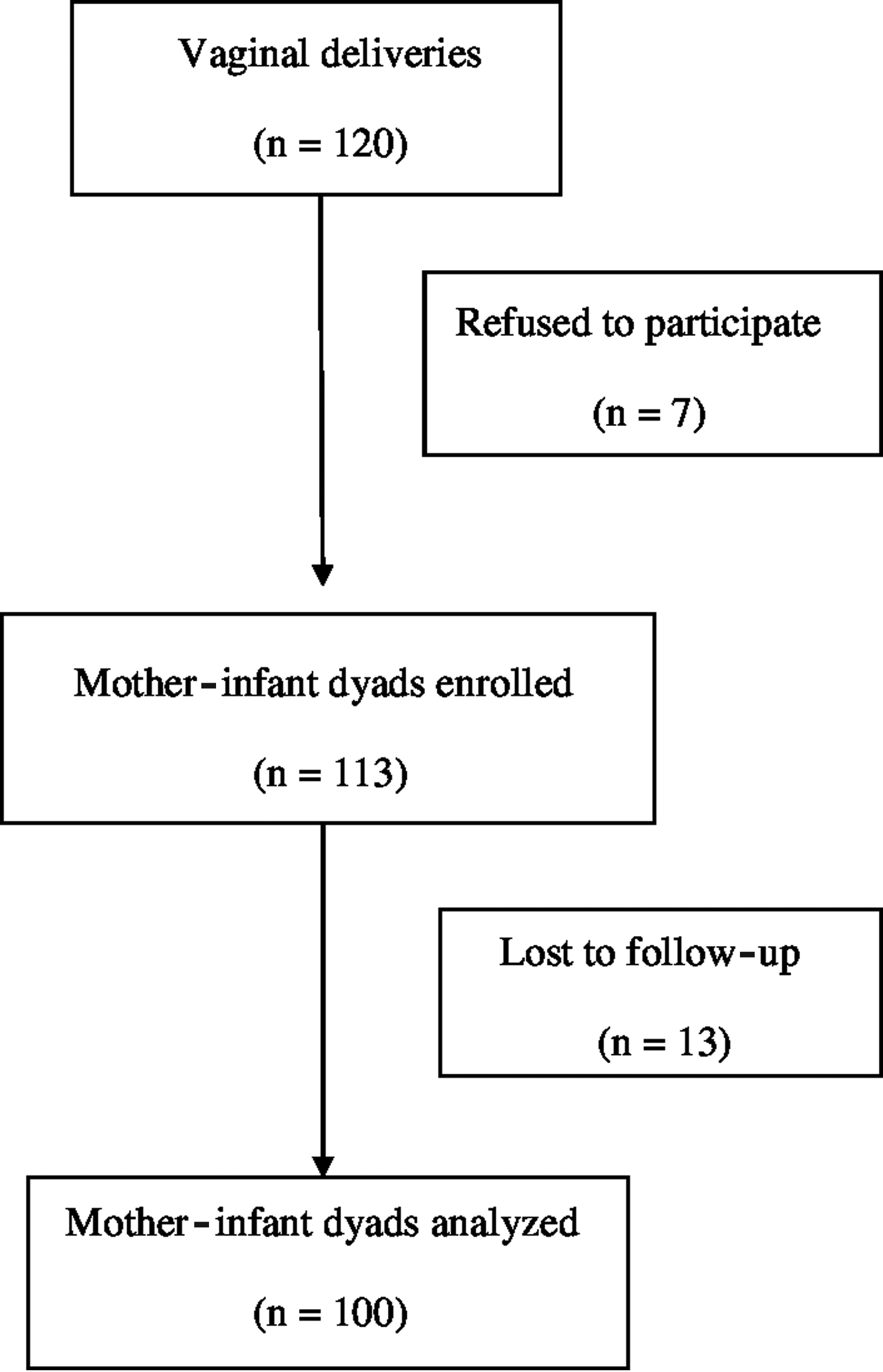
Flowchart of enrollment and follow-up of our study participants.
Mean and standard deviation.
Number and percentage.
Median and interquartile range.
APGAR, Appearance, Pulse, Grimace, Activity, Respiration (a score at birth based on five components).
Statistically significant difference in the breastfeeding rates at 6 weeks with respect to the maternal characteristics has been highlighted in bold.
Mean and standard deviation.
Number and percentage.
Primiparous women were more likely not to be exclusively breastfeeding at 6 weeks postpartum (p = 0.0068). Women from urban areas had higher breastfeeding rates at 6 weeks (p = 0.02). Women belonging to upper middle class and those who graduated from college had higher breastfeeding rates at 6 weeks (p = 0.009 and 0.02). Mean LATCH score at birth was significantly higher in women breastfeeding at 6 weeks than in those who weaned (7.17 ± 1.13 versus 4.26 ± 1.7, p = <0.0001 CI −3.4 to −2.34). Similarly, the mean LATCH score at 48 hours/discharge was significantly higher in women breastfeeding at 6 weeks than in those who weaned (9.22 ± 1.01 versus 5.78 ± 1.29, p = <0.0001 CI −3.89 to −2.98). The sensitivity and specificity of different cutoffs of LATCH scores at birth and 48 hours/discharge in predicting breastfeeding at 6 weeks are summarized in Table 5. Highest sensitivity (93.5%) and specificity (65.78%) were noted for a latch score ≥6 at birth. The RR of a LATCH score of 6 or more at birth was 5.92 (2.37–14.81), P = 0.0001. This means that women with a LATCH score of 6 or more at birth are 5.92 times more likely to be breastfeeding at 6 weeks postpartum compared with women with lower scores. Sensitivity of a LATCH score at 48 hours/discharge of 8 or more was 93.55% with a specificity of 92.1%. The RR of a LATCH score of 8 or more at 48 hours/discharge was 9.28 (3.6–23.4), P = <0.0001. ROC analysis for the LATCH scores at birth (Fig. 3) and exclusive breastfeeding rates at 6 weeks showed an area under curve (AUC) of 0.915 with a cutoff ≥5.5, showing highest sensitivity (93.5%) with a low false positive rate (34.2%). Similarly, ROC analysis for the LATCH scores at 48 hours/discharge (Fig. 4) and exclusive breastfeeding rates at 6 weeks showed an AUC of 0.979 with cutoff ≥7.5 showing highest sensitivity (93.5%) with a low false positive rate (7.9%).
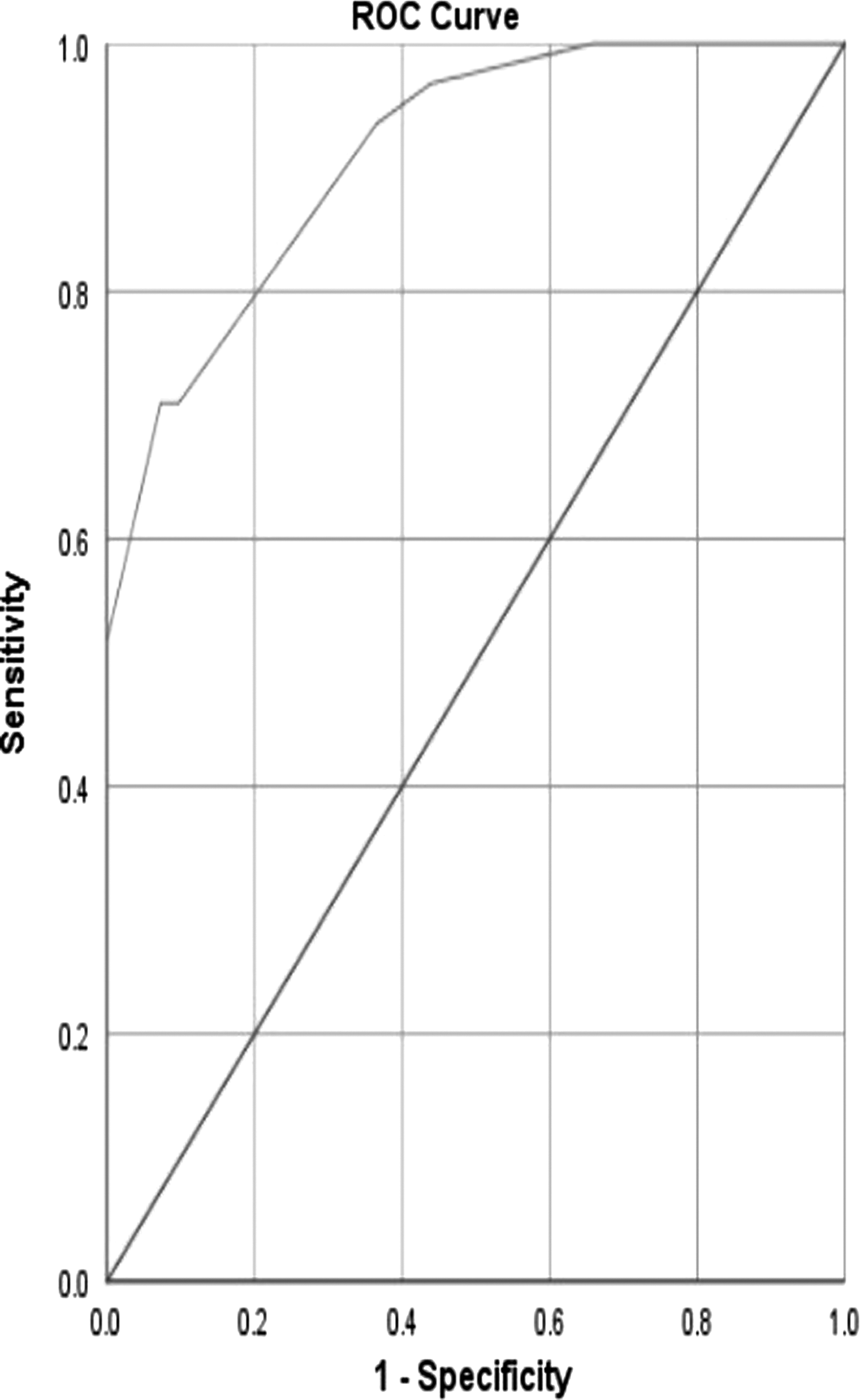
ROC for LATCH scores at birth and exclusive breastfeeding at 6 weeks postpartum. The AUC is 0.915. A LATCH score cutoff ≥5 at birth is found to have a sensitivity of 93.5% and false positive rate of 34.2% in predicting exclusive breastfeeding at 6 weeks postpartum. AUC, area under curve; ROC, receiver operating characteristic.

ROC for LATCH scores at 48 hours/discharge and exclusive breastfeeding at 6 weeks postpartum. The AUC is 0.979. A LATCH score cutoff ≥7.5 at 48 hours/discharge to have a sensitivity of 93.5% and false positive rate of 7.9% in predicting exclusive breastfeeding at 6 weeks postpartum.
Discussion
This study demonstrates the utility of LATCH scores in the first 48 hours after birth to predict exclusive breastfeeding rates at 6 weeks postpartum. Table 6 compares LATCH score and exclusive breastfeeding rates with those of other studies. In our study, we included only vaginal deliveries in contrast to other studies. All these studies found higher LATCH scores in those who breastfed at 6 weeks than those who had weaned by that time, which are similar to our study. In Kumar et al.'s 7 study, LATCH score evaluation was done at five time points within 72 hours after delivery. Exclusive breastfeeding rates in our study were comparable to other studies. In a study by Kumar et al, 7 24% of the mothers were lost to follow up at 6 weeks, which resulted in low (50%) exclusive breastfeeding rates at 6 weeks.
Mean and standard deviation.
EBF, exclusive breastfeeding; LSCS, lower segment cesarean section; VD, vaginal delivery.
We derived cutoffs for LATCH score at birth and 48 hours along with sensitivity and specificity to predict exclusive breastfeeding rates at 6 weeks. A LATCH cutoff of ≥6 at birth and ≥8 at 48 hours/discharge had the highest sensitivity and specificity in predicting exclusive breastfeeding in our study. The cutoffs derived were similar to those in Kumar et al. 7 and Tornese et al. 9 studies (Table 7). In Kumar et al.'s 7 study, the cutoff at 48–72 hours was not statistically significant due to small sample size (n = 23) and due to early hospital discharge (<48 hours).
Limitations
Our sample size is small. We did not analyze the different components of the LATCH system separately with respect to duration of breastfeeding due to practical difficulties. The effect of intervention was not analyzed and we would like to continue the study.
Conclusion
LATCH score represents a simple cost-effective tool to assess and monitor breastfeeding more objectively, especially in low-resource settings. It is capable of predicting breastfeeding duration as early as the first 24 hours of life. Low LATCH scores indicate the need for active intervention, support, and postdischarge follow-up.
We recommend that the LATCH score can be used as an assessment tool at delivery in all hospitals to assist in identifying and targeting mothers at risk of early weaning to improve the breastfeeding duration as well as confidence in the mothers.
Footnotes
Acknowledgments
We thank Dr. Jayashree Jayakrishnan, our lactation consultant, and Mrs. Dharma, labor delivery room staff nurse, for their assistance.
Disclosure Statement
No competing financial interests exist.