
Abstract
Abstract
Objectives:
Recently, an increasing number of studies have implied that breastfeeding has a protective effect on maternal hypertension, but it remains controversial. The aim of this study is to evaluate the effect of breastfeeding on maternal hypertension through meta-analysis.
Materials and Methods:
Eligible studies were searched and identified in various databases. Meta-analysis was conducted to assess the association between the duration of breastfeeding and maternal hypertension.
Results:
Seven eligible studies that contained 444,759 participants were included in our study. Meta-analysis of these seven studies showed a significant protective effect of breastfeeding on maternal hypertension. Specifically, pooled odds ratios (ORs) of hypertension for >0–6, >6–12, and >12 months of breastfeeding were 0.92 (95% confidence interval [CI]: 0.88–0.96, I2 = 67.5%), 0.89 (95% CI: 0.86–0.92, I2 = 0), and 0.88 (95% CI: 0.84–0.93, I2 = 43.9%), respectively, compared with nonbreastfeeding mothers, and the pooled OR of hypertension was 0.93 (95% CI: 0.91–0.95, I2 = 40.8%) for women who breastfed compared with women who had not. Furthermore, the pooled hazard ratio of hypertension was 1.34 (95% CI: 1.17–1.52, I2 = 58.7%) for women who did not breastfeed compared with women who breastfed for more than 12 months for their first child.
Conclusion:
Different durations of breastfeeding have different protective effects against the development of maternal hypertension, and breastfeeding for >12 months has a better effect than <12 months.
Introduction
H
Breastfeeding is a unique biological phenomenon of mothers that is beneficial for both infants and mothers. 10 For infants, breastfeeding can not only provide nutrition for the body and promote neural development but can also prevent diseases in adulthood. 11 In addition, the risk of some chronic diseases, including diabetes and obesity, is also likely to be reduced through breastfeeding.10,12 Breastfeeding has also proven to be beneficial to mothers. It is well known that breastfeeding can reduce the risk of breast cancer and ovarian cancer. 13 Also, there is evidence that breastfeeding alters maternal cardiovascular function, and mothers who breastfeed have lower rates of obesity and cardiovascular disease.10,14 Experimental studies have also found differences in blood pressure and cardiac output between mothers who have a history of breastfeeding and mothers who do not.14,15 Although the mechanism of breastfeeding on maternal hypertension is not well understood, studies have shown that breastfeeding can maintain a normal level of blood pressure, and women who have never breastfed or who breastfed short term may have a higher risk of maternal hypertension compared with mothers who breastfed for a longer duration.16–18 Thus, promoting breastfeeding may help reduce the risk of maternal hypertension. In recent years, increasing numbers of studies have assessed the association of breastfeeding and risk of maternal hypertension, but the conclusion remains controversial. Therefore, to ascertain the effect size of breastfeeding on maternal hypertension by exploring which duration of breastfeeding is the best to reduce the risk of hypertension, we systematically reviewed the literature for the duration of breastfeeding and maternal hypertension.
Materials and Methods
Literature search
We comprehensively searched PubMed, Web of science, Science Direct database, China National Knowledge Infrastructure database (CNKI), Wanfang database, and Chinese Biomedical database (CBM) to find potential articles that explored the association between duration of breastfeeding and maternal hypertension. The final search was updated on August 26, 2017, and the language was limited to English and Chinese. The search strategy was performed in ti/ab/key fields as the following: (breastfeeding OR breastfeed OR lactation) and (high blood pressure OR hypertension OR hypertensive disorders). Potentially relevant articles were retrieved to review the full-text. In addition, we also reviewed the references in the articles to find more potentially eligible studies.
Study selection
Retrieved studies were included when they met all of the following inclusion criteria: (1) it was a cross-sectional or cohort study; (2) the participants included women who had given birth; (3) the study reported the duration of breastfeeding, which was measured by their live birth, and the measurement of hypertension in participants; (4) the study reported the number of hypertensive and nonhypertensive participants in the different durations of breastfeeding or offered the odds ratio (OR), relative risk (RR), and hazard ratio (HR) with their confidence interval (95% CI) of maternal hypertension in the different durations of breastfeeding.
To make the results of our meta-analysis more stable and credible, eligible studies not only met all of the inclusion criteria but also were not allowed to have any of the following characteristics: (1) it was a review, case report, animal experiment, or conference literature; (2) the study used inappropriate statistical methods or reported incomplete data that may cause a certain bias in our meta-analysis; (3) the measurement of hypertension had no clear standards; (4) if there were duplicate publications, only the one with the largest sample numbers and complete data was included.
All of the selection work was conducted by two authors (L.L.W. and W.W.), and disagreements were solved by consensus.
Data extraction and quality assessment
Two authors (G.B.Q. and L.L.W.) independently extracted information from all eligible studies. The following information was extracted from included studies if available: the first author's name; year of publication; study design; location; the assessment criteria of hypertension; the number of hypertensive and nonhypertensive participants in different durations of breastfeeding; OR, RR, and HR with their 95% CI, which reflected the association between duration of breastfeeding and maternal hypertension after adjusting for a number of confounding factors; demographics of included studies in the final analysis in each breastfeeding category; and adjusted factors in multiple analyses. To assess the quality of included articles, two authors (G.B.Q. and X.T.) checked the full-text of all included articles independently. If there was any disagreement, it was resolved by the third author. The quality of each study was evaluated in reference to the STROBE statement from 22 items. 19
Statistical analyses
We conducted a meta-analysis among parous women who had different durations of breastfeeding. To ascertain the association between different durations of breastfeeding and maternal hypertension and its exact effects, we first collected the number of hypertensive and nonhypertensive women in different durations of breastfeeding groups. Then, comparison of different durations of breastfeeding groups was conducted to obtain various pooled ORs. Second, we extracted ORs, RRs, and their 95% CI reported from included studies, and effect sizes of the same category in duration of breastfeeding were merged into pooled ORs to assess this association. Furthermore, the separately extracted HRs were amalgamated as pooled HR to evaluate the risk of maternal hypertension for nonbreastfeeding women compared with women who breastfed for more than 12 months for their first child.
The between-study heterogeneity was accessed by the p value of the Cochran Q test and I2 test value. We considered significant heterogeneity between included studies only if p < 0.1. 20 We also defined an I2 test value of 25–50% as mild heterogeneity, 50–75% as moderate heterogeneity, and ≥75% as severe heterogeneity. Forest plots were created by the fixed-effects model (the Mantel–Haenszel method) if there was no obvious heterogeneity; otherwise, a random-effects model was used.21,22
Owing to the limited included studies, it was difficult for us to conduct subgroup analysis according to the characteristics of included studies. Thus, a sensitivity analysis was conducted to explore the influence of any study on pooled estimates by omitting studies by turns when there was severe heterogeneity between included studies. After sensitivity analysis, we excluded studies with great influence on the stability of the results in our meta-analysis and recombined reported statistics from the remaining studies.
Begg's rank correlation test and funnel plot were performed to quantitatively and qualitatively investigate whether there was any publication bias. If p values of Begg's test were greater than 0.05 and funnel plots were symmetrical, it indicated that there was no obvious publication bias in this meta-analysis. 23 All statistical analyses were performed using Stata software, version 14.0 (Stata Corporation, College Station, TX).
Results
Description of the included studies
After the literature searches through databases, we initially found 2,588 records. By screening titles and abstracts and viewing the full-text of these records, seven studies were finally included in our systematic review and meta-analysis.16,17,24–28 The details are shown in Figure 1. Seven included studies contained 444,759 total participants. Of the seven studies, two were prospective studies,17,26 and five were retrospective studies.18,22,25,27,28 Two studies were conducted in China,24,28 three in the United States,16,25,26 one 27 in Norway, and one 17 in Korea. According to the extracted duration of breastfeeding, we found five studies reporting that the assessment of the duration of breastfeeding started with the first live birth,16,17,24,25,27 and the sum of the duration of breastfeeding in each child is the final variable for analyses, but two other studies26,28 reported that the duration of breastfeeding was only measured for the first child. For the outcomes of included studies, four reported numbers of hypertensive and nonhypertensive subjects in each breastfeeding category,24,25,27,28 three displayed ORs about cumulative duration of breastfeeding and maternal hypertension,16,24,25 and two showed HRs of no breastfeeding compared with more than 12 months of breastfeeding for their first child.26,28 Major confounding factors such as age, smoking, and body mass index were adjusted in most studies. More characteristics are shown in Table 1 (See Supplementary Tables S1 and S2; Supplementary Data are available online at www.liebertpub.com/bfm).
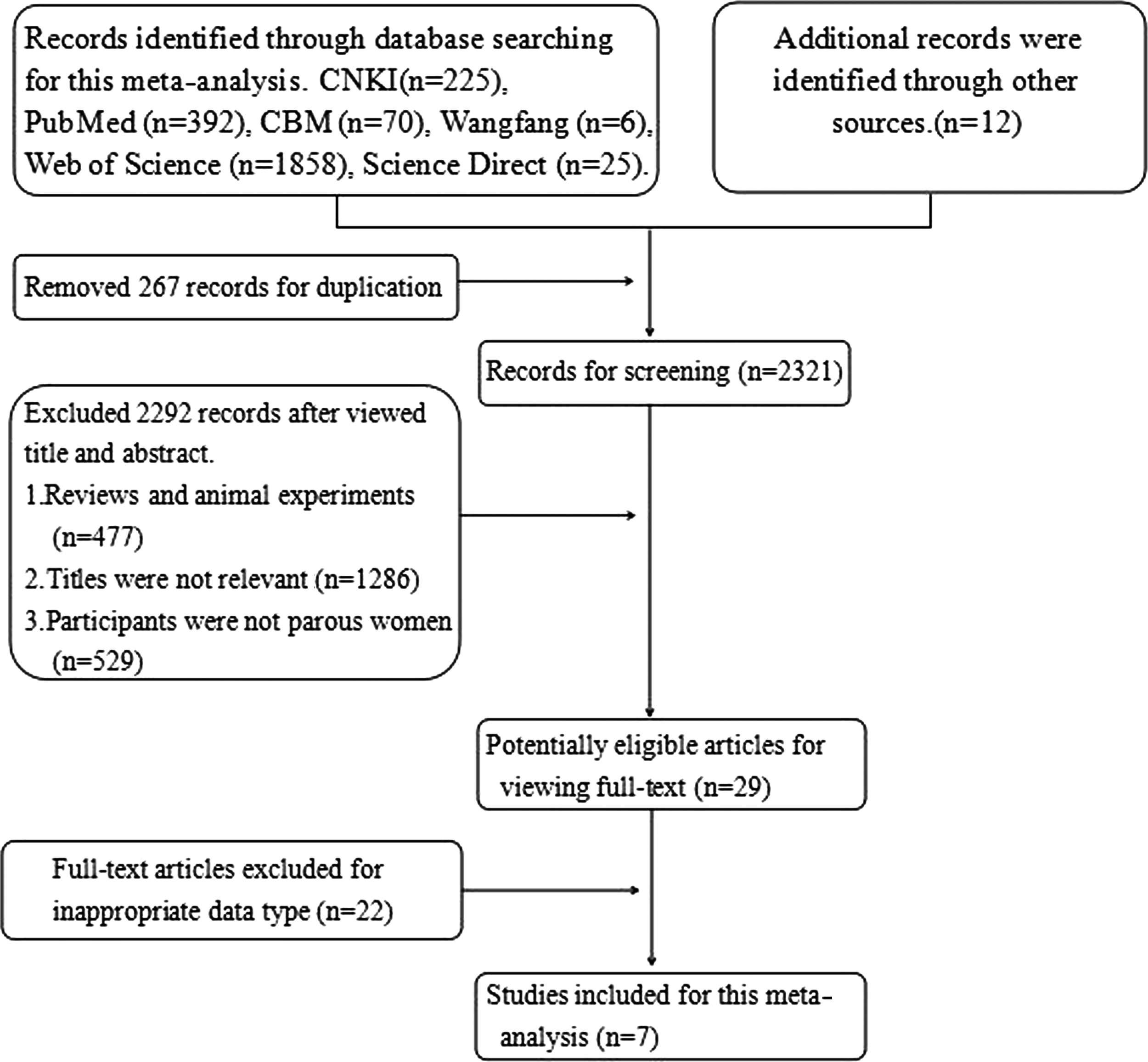
Flowchart of this meta-analysis.
NC, not clear.
The impact of duration of breastfeeding on the risk of maternal hypertension
First, we collected the number of hypertensive and nonhypertensive mothers in each duration of breastfeeding from four studies, and the duration of breastfeeding was classified into four categories: nonbreastfeeding, >0–6, >6–12, and >12 months. The pooled OR for >0–6 months of breastfeeding was 0.79 (95% CI: 0.65–0.96, I2 = 89.4%), compared with no breastfeeding. The sensitivity analysis showed that one study 25 had an influence on the stability of this meta-analysis. After omitting that one, the pooled OR increased (OR = 0.82, 95% CI: 0.74–0.91, I2 = 64.8%). Similarly, the adjusted pooled ORs for >6–12 and >12 months of breastfeeding were 0.88 (95% CI: 0.74–1.05, I2 = 85.6%) and 0.88 (95% CI: 0.84–0.93, I2 = 43.9%), respectively, compared with parous women who had not breastfed (Table 2). However, there was no significant difference in the risk of hypertension for >0–6 and >6–12 months of breastfeeding compared with >12 months (Fig. 2).
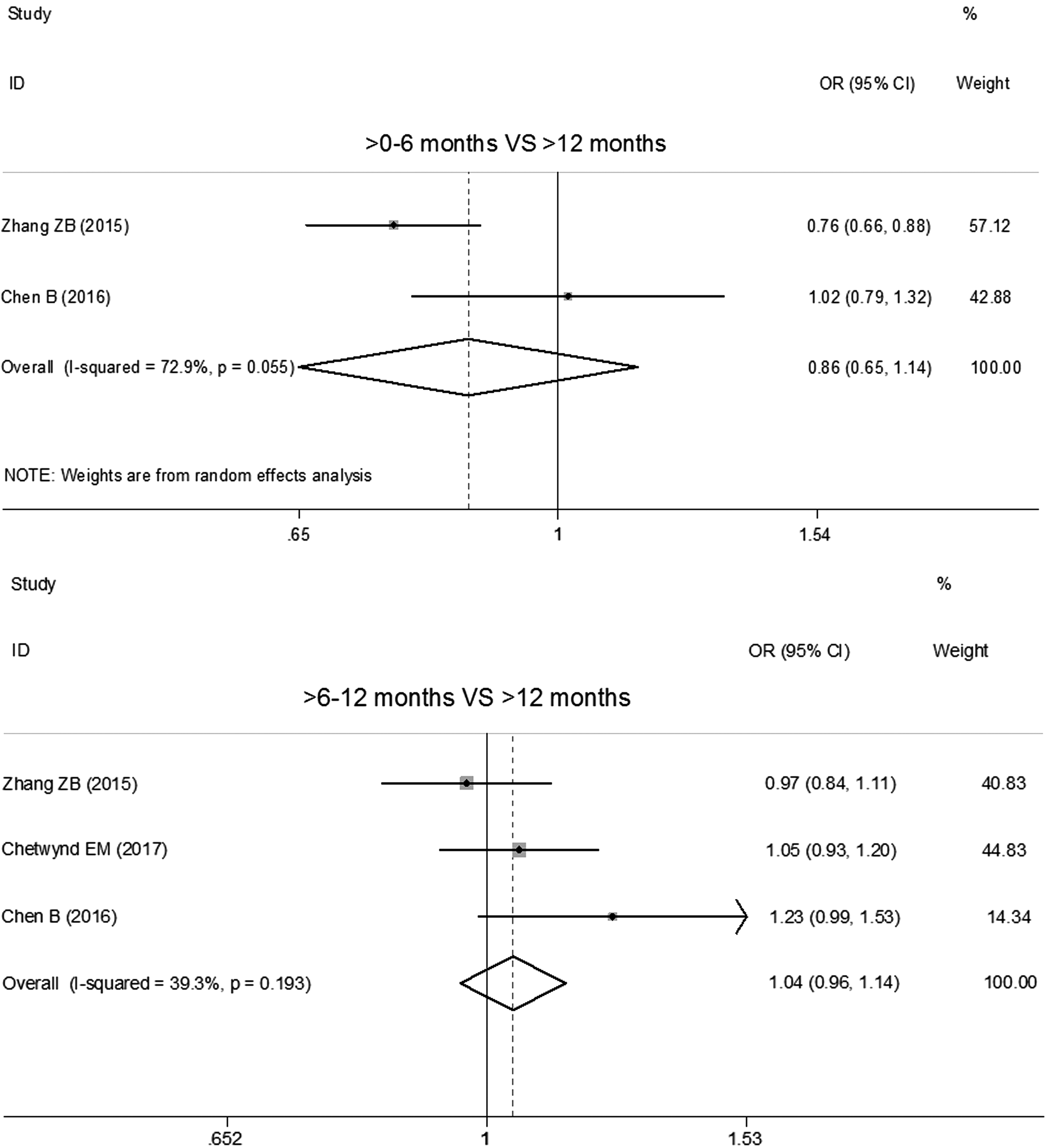
The ORs of maternal hypertension for > 0–6 and > 6–12 months of breastfeeding compared with >12 months. CI, confidence interval; OR, odds ratio.
CI, confidence interval; F, a fixed-effects model; NA, not applicable; OR, odds ratio; R, a random-effects model.
Second, we extracted OR, RR, and their 95% CI according to the same breastfeeding categories from the included studies. The pooled ORs for >0–6 and >6–12 months of breastfeeding were 0.92 (95% CI: 0.88–0.96, I2 = 67.5%) and 0.89 (95% CI: 0.86–0.92, I2 = 0) compared with nonbreastfeeding mothers after meta-analysis (Figs. 3 and 4). Simultaneously, we merged the OR of hypertension for women who had ever breastfed compared with women who had not, and the pooled OR was 0.93 (95% CI: 0.91–0.95, I2 = 40.8%) (Fig. 5).
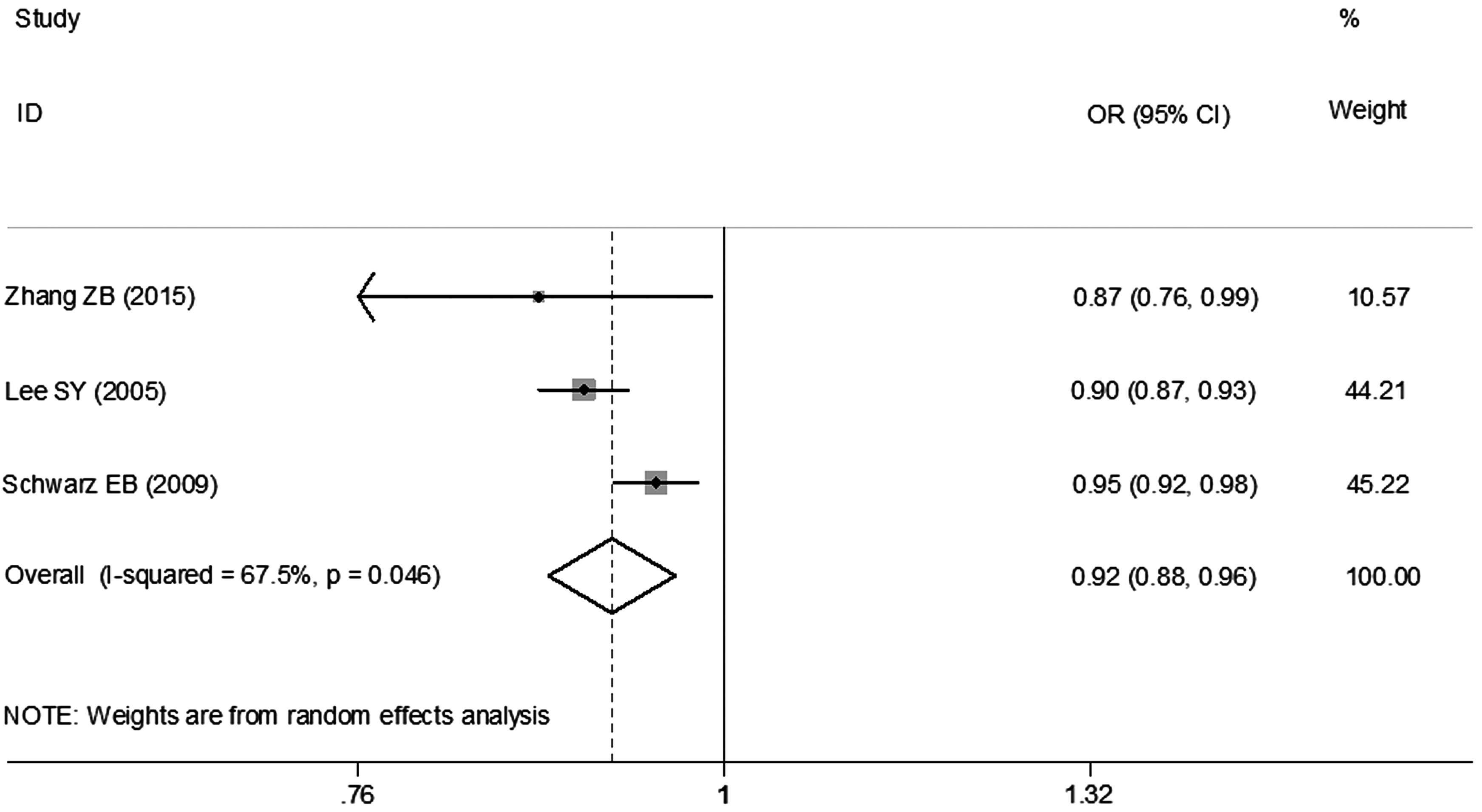
The OR of maternal hypertension for > 0–6 months of breastfeeding compared with nonbreastfeeding mothers.
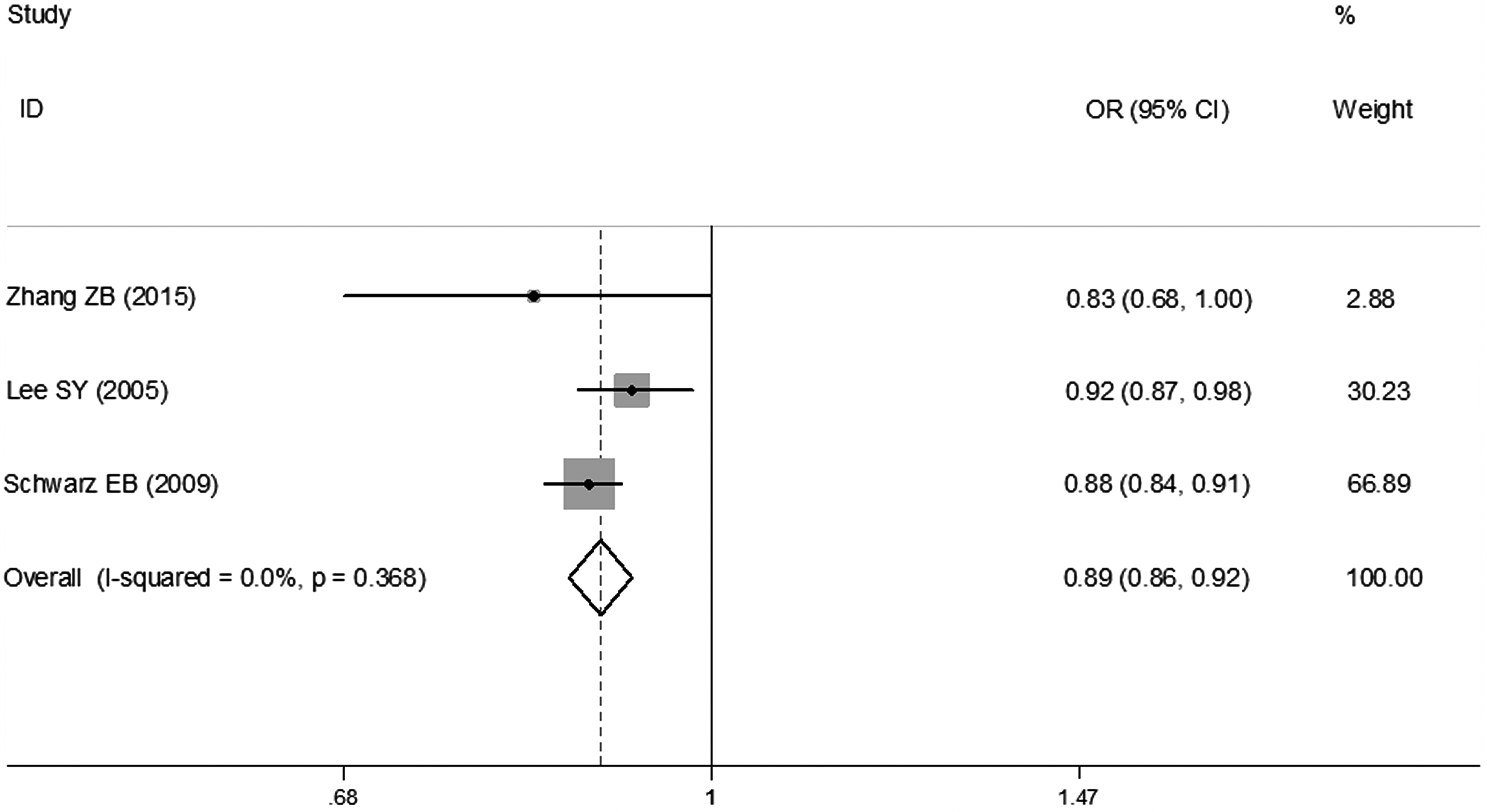
The OR of maternal hypertension for > 6–12 months of breastfeeding compared with nonbreastfeeding mothers.
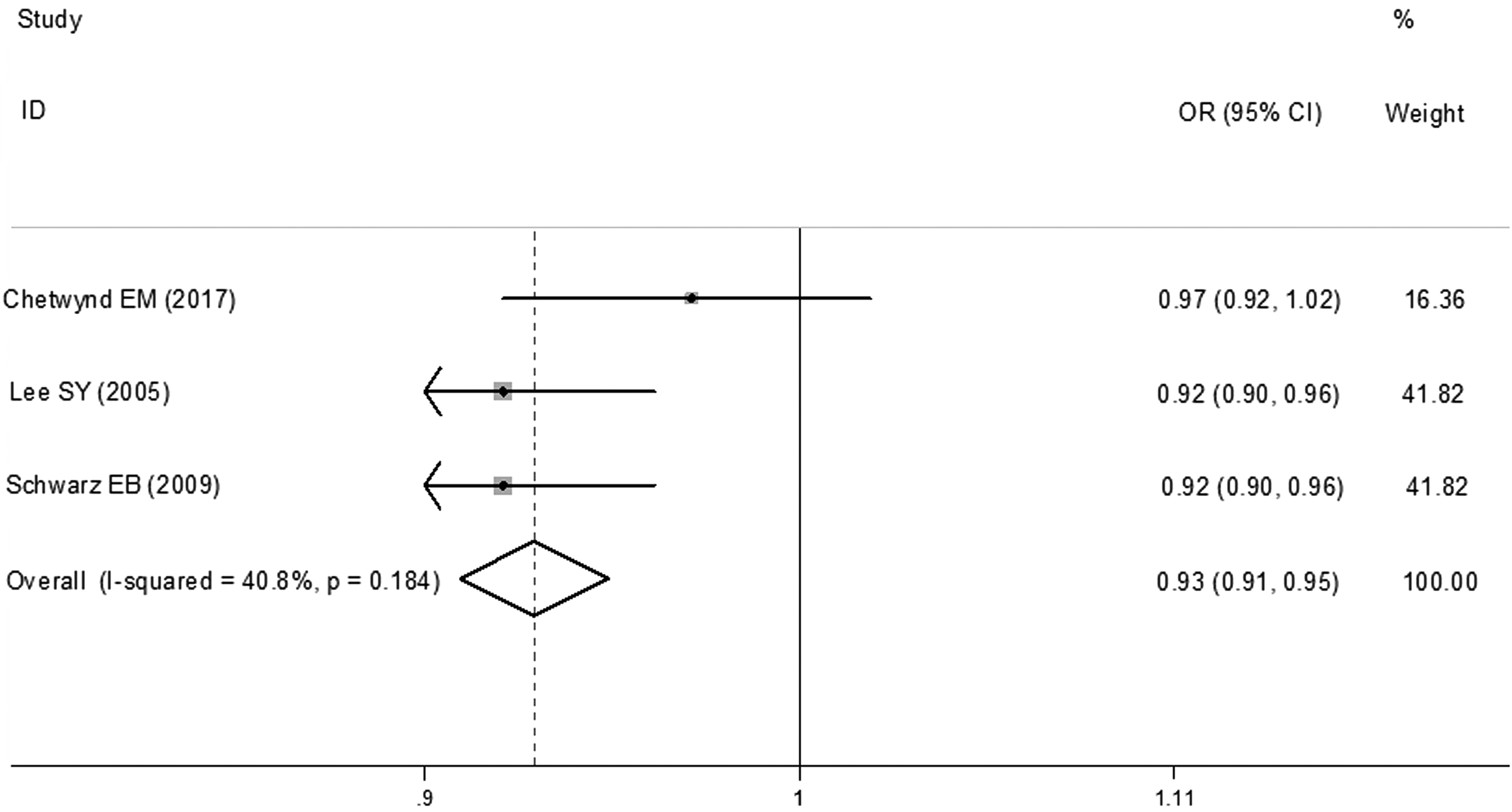
The OR of hypertension for women who breastfed compared with women who had not.
Finally, two studies also reported the HR of hypertension for women who had not breastfed compared with women who breastfed for more than 12 months for their first child. Meta-analysis showed that the pooled HR of no breastfeeding was 1.34 (95% CI: 1.17–1.52, I2 = 58.7%) (Fig. 6). There was no evidence of publication bias from the results of Begg's test in all analyses.
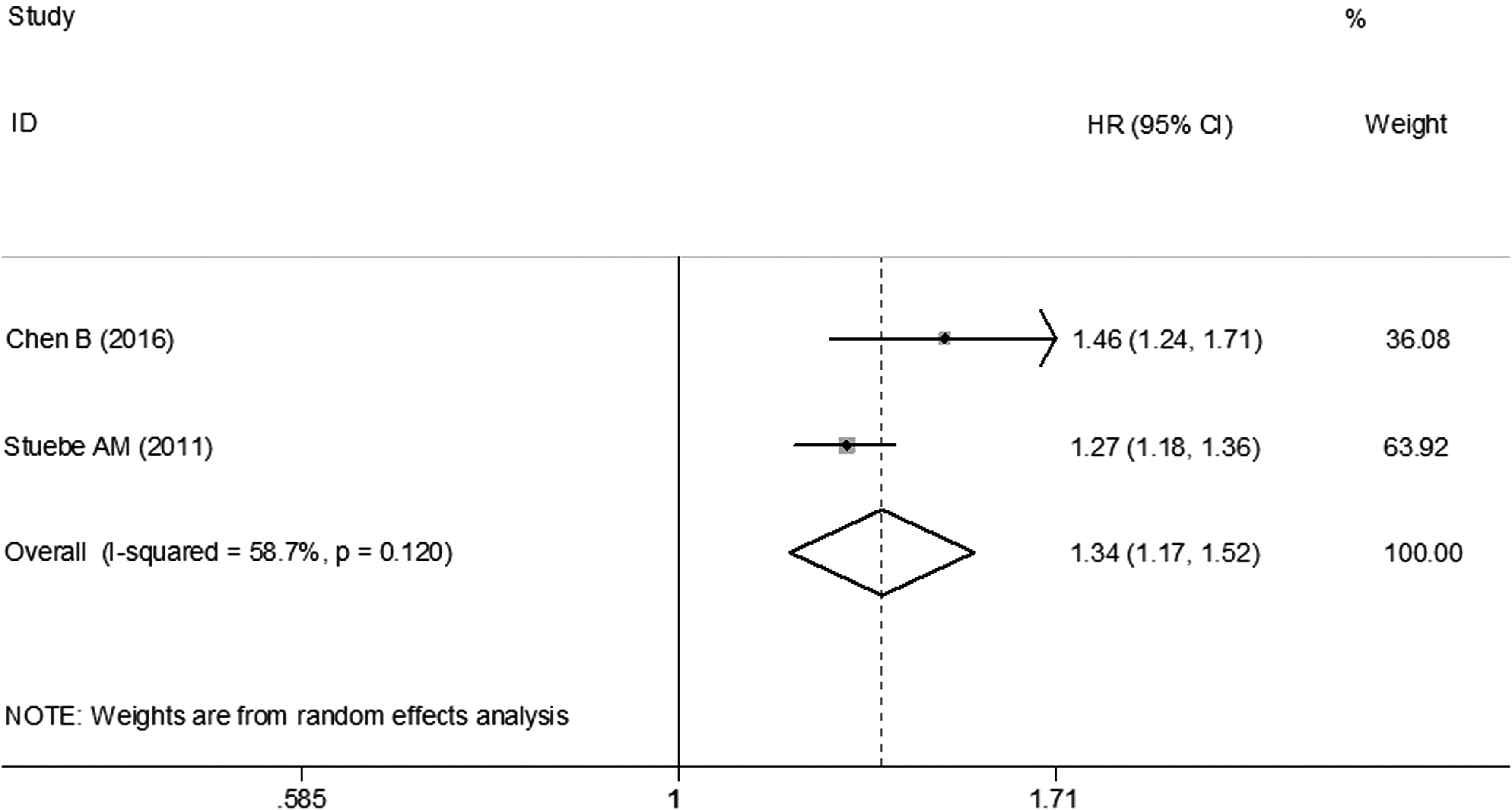
The HR of hypertension for women who did not breastfeed compared with women who breastfed for more than 12 months. HR, hazard ratio.
Discussion
Significantly, increasing numbers of studies on breastfeeding have been published over the last two decades. However, the definition of breastfeeding is inconsistent and should be better developed. 29 Accordingly, the synthesis and comparison of findings from these studies are severely limited. A previous systematic review also reported that the definition of breastfeeding remains inconsistent in published articles, and consistently utilized definitions are urgently needed. 29 Breastfeeding history was measured through a questionnaire in included studies of our meta-analysis, but a clear definition of any breastfeeding was still lacking. As we all know, the proportion of mothers breastfeeding varies during 24 hours, and the different proportions of breastfeeding have different effects on mothers and infants. Hence, the results of our meta-analysis may not completely reflect the effect of a certain proportion of breastfeeding on maternal hypertension.
Our systematic review and meta-analysis found that breastfeeding did have a protective effect on maternal hypertension. The OR of maternal hypertension for ever breastfeeding was 0.93, compared with no breastfeeding, and the HR of maternal hypertension for no breastfeeding was 1.34, compared with more than 12 months of breastfeeding. It is in contrast to results of the study of Chetwynd et al., which indicated that there was little evidence of an association between ever breastfeeding and incident hypertension. 25 Interestingly, our meta-analysis found that different durations of breastfeeding had different effects on the generation of maternal hypertension. Specifically, more than 12 months of breastfeeding had a greater effect on preventing hypertension compared with less than 12 months of breastfeeding. However, this precise effect needs more studies to verify. On the contrary, the results of the meta-analysis from different types of extracted data showed subtle differences, and there were several causes for these differences. Extracted numbers of hypertensive and nonhypertensive subjects in the different durations of breastfeeding were initially reported in included studies. However, statistical indicators reflecting the association between the duration of breastfeeding and maternal hypertension were calculated from raw values and were adjusted for numerous confounding factors. Furthermore, the included studies were conducted in various regions with diverse study designs. These reasons might cause dissonance in the results of this meta-analysis. Importantly, using numerical data, the meta-analysis qualitatively or quantitatively compared the risk of maternal hypertension in the different durations of breastfeeding to some degree.
Although few studies have explored the relationship between the duration of breastfeeding and maternal hypertension, some researchers have also pointed out that breastfeeding can alter maternal cardiovascular function. Evidence has shown that breastfeeding mothers have lower systolic blood pressure levels in reaction to laboratory-induced stress than bottle-feeding mothers, and breastfeeding mothers have lower systolic and diastolic blood pressure during infant feeding and for 1 hour afterward.15,30 Choi et al. 31 also indicated that the OR of elevated blood pressure was 0.67 for women who breastfed for 6–11 months compared with those who breastfed for less than 5 months, adjusted for possible confounding factors in a multivariable logistic regression analysis. Conversely, Robson 32 reported that there was no significant difference in blood pressure between breastfeeding and nonbreastfeeding groups. Similar phenomena have been observed in some animal experiments in which breastfeeding affected cardiovascular function in rats and rabbits.33,34
The mechanisms underlying the associations of breastfeeding and maternal hypertension are not yet clear. The hypothesis proposed in human and animal studies is that oxytocin release plays a crucial role in the control of blood pressure. During infant feeding, breastfeeding mothers released higher levels of oxytocin than bottle-feeding mothers, and mothers with increased levels of oxytocin had lower blood pressure, meaning that oxytocin has an antihypertensive effect.15,35–37 In animal experiments, male and female rats had a sustained decrease in blood pressure without effects on the heart rate after subcutaneous or intracerebroventricular oxytocin injection. 34 These short-term effects of oxytocin on blood pressure primarily reflect direct effects of circulating oxytocin on the vasculature, but the long-term effects of oxytocin do not seem to be obviously related to a direct effect of oxytocin because of the short half-life period of oxytocin. The mechanisms of long-term effects of oxytocin involving cortisol, central α2-adrenergic activity, and female hormones have been proposed. It is known that oxytocin has inhibitory effects on cortisol secretion in humans. 38 In fact, a significant attenuation of serum cortisol concentrations was measured not only during the first week but up to 6 months postpartum in lactating women as well. 39 Furthermore, the long-term effect of oxytocin observed by investigators is that chronic oxytocin exposure induces an increase in central α2-adrenergic activity, which lowers blood pressure by decreasing sympathetic drive on both the heart and vessels. 40 Also, female sex hormones can stimulate oxytocin synthesis and release or increase binding to oxytocin receptors, which may potentiate the oxytocin-induced effects on blood pressure.41,42
To our knowledge, this was the first systematic review and meta-analysis to assess the association between breastfeeding and maternal hypertension. The larger sample size of included articles made the results of this meta-analysis more stable and reliable. The association between different durations of breastfeeding and risk of maternal hypertension that were explored helped us to better understand the various effects of different durations of breastfeeding. However, there were also several limitations in our meta-analysis. First, our meta-analysis only included seven studies that explored the association between breastfeeding and hypertension in women, and these studies were performed in different locations and contained various characteristics of women. Limited numbers and inconsistent characteristics of the included studies made us unable to further analyze this association by subgroup analysis according to the characteristics of included studies. Therefore, it is unclear to us whether this association is the same in different populations or regions. More studies on these aspects should be performed in the future. Second, owing to the different breastfeeding categories reported in the included studies, we could only collect the similar categories, which gave us little chance to analyze the association between breastfeeding and hypertension according to the various durations of breastfeeding. Therefore, it is not clear which duration of breastfeeding is the best for protecting mothers' health later in life. Finally, most of the included studies were retrospective, and our study could only report the strength of the protective effects of breastfeeding on maternal hypertension but could not infer a causal correlation or the clear mechanism of them. Prospective, high-quality studies are needed to solve these deficiencies.
Conclusion
Our systematic review and meta-analysis suggest that breastfeeding plays a protective role in the development of maternal hypertension. There are differences in the strength of the protective effects in the different durations of breastfeeding. With an increase in the duration of breastfeeding, this effect will be increased. Moreover, compared with mothers who breastfeed their first child for more than 12 months, nonbreastfeeding mothers have a higher risk of maternal hypertension, which means breastfeeding for more than 12 months assuredly has a protective effect against hypertension. In summary, breastfeeding for >12 months is better protection against the development of maternal hypertension than <12 months. Consequently, it is strongly recommended that mothers should breastfeed their children and properly prolong the duration of breastfeeding.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.