
Abstract
Abstract
Background:
Maternal breast engorgement is one of the most common problems in the postpartum period. There are several alternative treatments, but there have not been any randomized controlled trial studies about the effects of herbal compresses for breast engorgement.
Objective:
The objective is to investigate the effects of herbal compresses for maternal breast engorgement.
Materials and Methods:
A randomized controlled trial was conducted. The postpartum mothers who had breast engorgement were randomly assigned to herbal or hot compress treatments. The breast engorgement pain scores were assessed by visual analog scales pre- and post-treatment. The pain reduction scales of the herbal compress treatments were analyzed and compared with the hot compress treatments. The adverse effects of each treatment were recorded and collected after 24 hours from treatments.
Results:
The data from 500 postpartum mothers with breast engorgement were available for analyses, 250 from the herbal compress group and 250 from the hot compress group. The baseline characteristics of both groups were similar except baseline breast engorgement pain score (herbal compress group higher than hot compress group). There were statistically significant mean differences of breast engorgement pain before and after treatment between the herbal and hot compress groups. No serious complications were found after treatment from herbal compresses.
Conclusion:
Among the postpartum mothers who had breast engorgement, the herbal compresses could decrease breast engorgement pain. The pain reduction after herbal compresses was found to be greater than with the hot compresses.
Introduction
M
The main ingredients of Thai herbal compresses include Plai or Cassumunar ginger (Zingiber cassumunar Roxb.), turmeric (Curcuma longa L.), and camphor. There are several published articles that have endorsed the anti-inflammatory and analgesic effects of Plai, turmeric, and camphor.3–5 The safety of herbal compresses used during the early postpartum and lactating periods was studied and no adverse effects were reported. 6 However, there have been few studies about the effects of herbal compresses on the outcomes resulting from breast engorgement discomfort. Thus, we are interested in the comparisons of breast engorgement treatment outcomes between herbal and hot compresses as seen in this study.
Materials and Methods
Setting
This study was performed in the Nakhon Nayok province, a rural area in the central part of Thailand. The data were collected during the period from July 2016 to October 2017 at the HRH Princess Maha Chakri Sirindhorn Medical Center. This is known as a Baby-Friendly Hospital. A routine practice in the postpartum ward is breastfeeding education. The 1-hour course in breastfeeding includes latching and is taught on the first day postpartum. One nurse teaches a group of three to five mothers. Mothers are encouraged to stimulate their infants to feed 8–12 times per day. Breast engorgement is a complication that has been routinely assessed by patients' nursing staff. If mothers have breast engorgement, a hot compress treatment is given according to our hospital guidelines. Mothers and infants are discharged if breast engorgement improves and they have shown no complications.
Procedure and collection of material
This study is a randomized controlled trial. Randomization was done using a computer-generated list with a block of five methods. After the allocating sequence was generated, the researcher enclosed herbal compress or hot compress in sequentially numbered sealed envelopes. These envelopes were kept with the nurses who opened each envelope when a new participant was recruited from mothers with breast engorgement at the postpartum ward. Mothers with breast engorgement must have no analgesics or nonsteroidal anti-inflammatory drug (NSAID) use before the breast engorgement treatment (6 hours at the least). Mothers were divided by treatment into two groups: herbal and hot compress groups. Each treatment was given only once and was started within 30 minutes after diagnosis. Pain scores were assessed immediately before and after breast engorgement treatments. The demographic data collected include age, marital status, educational level, income, occupation, route of delivery, body mass index, breastfeeding experience, and the time of the breast engorgement diagnosis. After 24 hours from treatment, the adverse effects of herbal and hot compresses were recorded in an adverse effects notation that was sealed in envelope by the mothers and were collected by the treating nurses. Differences in pain scores between the before and after treatments were analyzed and compared between the herbal and hot compress groups. The adverse effects envelope was then opened and reported by the researcher.
Breast engorgement
Assessment of breast engorgement was graded according to the criteria of Robson. 1 The degree of breast engorgement has a four-level scale. Grade 1: breast has minimal tenderness, minimal distension, and slight edema. Grade 2: breast is somewhat painful, has moderate distension, and mild edema. Grade 3: breast is very painful, has large distension, and moderate edema. Grade 4: breast is extremely painful, has marked distention, and severe edema. We recruited mothers with grades 3 and 4 for this study.
Herbal compress
The herbal compress balls were prepared by the Pharmaceutical Department, HRH Princess Maha Chakri Sirindhorn Medical Center, with proper manufacturing practices. The herbal compress ball weighed 250 g and contained dried herbs that included the following: Z. cassumunar Roxb. rhizomes (90.5 g), C. longa L. rhizomes (18.2 g), Cymbopogon citratus (DC) Stapf leaves and leaf sheaths (18.2 g), Acacia concinna (Willd.) DC leaves (18.2 g), Tamarindus indica L. leaves (54.3 g), Citrus hystrix DC peels (36.2 g), Blumea balsamifera (L.) DC leaves (5.4 g), salt (3.6 g), and camphor (5.4 g).
Before treatment, two herbal balls were steamed in a stacked steamer for 20 minutes. Then, the first herbal ball was wrapped with towels to protect the mother's skin from burns due to excessive heat. Next, the nurse gently touched and rolled the herbal ball on the breast area with exception to the nipple and areola areas. The contact time for each point was ∼10 seconds. Then, the towel was unwrapped when the herbal ball was sufficiently cool to apply directly to the skin. The first herbal ball was replaced when the second was lukewarm. The two herbal balls were alternately compressed and alternately steamed until each treatment session was completed. The total session duration was 20 minutes.
Hot compress
Before treatment, small towels were prepared and packed as herbal balls. Two ball-like towels were steamed in a stacked steamer pot for 20 minutes. Then, the first towel ball was wrapped with a towel to protect the mother's skin from burns due to excessive heat. The nurse gently touched and rolled the towel ball on the breast areas with the exception of the nipple and areola. The contact time for each point was ∼10 seconds. The towel was unwrapped when the towel ball was sufficiently cool to put directly on mother's skin. The second towel ball was replaced when the first one was detected to be lukewarm. The two towel balls were alternately compressed and alternately steamed until each treatment session was achieved. The total session duration was 20 minutes.
Inclusion criteria
The postpartum women who had deliveries without complications (i.e., multiple pregnancies, preeclampsia, antepartum hemorrhaging, and preterm labor) and who had grade 3 or 4 breast engorgement were recruited. Mothers had not been given any analgesics or NSAID drugs before breast engorgement treatments for at least 6 hours. Their infants had birth weights of more than 2,500 g and were born without complications. The mothers had suffered no acute postpartum hemorrhages and had no contraindications to breastfeeding.
Exclusion criteria
Mothers whose infants were diagnosed with galactosemia were excluded from this study.
Breast engorgement pain score
Pain levels from the breast engorgement were assessed by use of a visual analog scale (VAS). The pain scale ranged from a score of 0 (no breast pain) to 10 (severe breast pain) in 10-cm line. Postpartum mothers were asked by nurses to place a line perpendicular to the VAS line at the points that represent their pain intensity. After the mothers had marked, using a ruler, the score is determined by measuring the distance on the 10-cm line between the “no breast pain” and the mothers' mark.
Sample size
We set a mean difference of 17% between the herbal and hot compress groups from a pilot study of 20 cases. We used 0.05 of α error, a power of 0.95, and an effect size = 0.34. The calculated sample size numbered 226 cases in each group. The subjects were totaled with an additional 10% for data loss. The total samples collected were 249 per group.
Ethical considerations
This study was approved by the Ethics Committee of the Srinakharinwirot University, Faculty of Medicine, and registered with Thai Clinical Trials Registry (registration number TCTR20180208002).
Statistical analysis
Demographic data are reported in means and percentages. We use the t-test to compare the mean of maternal ages, income, body mass index, and pain scores between the herbal and hot compress groups. The data regarding marital status, education, occupation, route of delivery, and breastfeeding experience were analyzed by chi-square. A p-value less than 0.05 considered statistically significant. Statistical analysis was performed using SPSS software (version 23.0, SPSS, Inc.).
Results
The postpartum women who had enrolled in our research project totaled 500 cases, 250 cases from each group. A flow chart of the number of participants is shown in Figure 1. Mothers were predominately married and high school graduates or lower. The mean income was 23,988 bahts/month (∼769 U.S. dollars/month). The percentage of cesarean sections was 57 and 59 in the herbal and hot compress groups, respectively. The mean body mass index was within the overweight ranges. There were no significant differences in the demographic data between both groups except baseline breast engorgement pain score. The details of the demographic data are shown in Table 1.
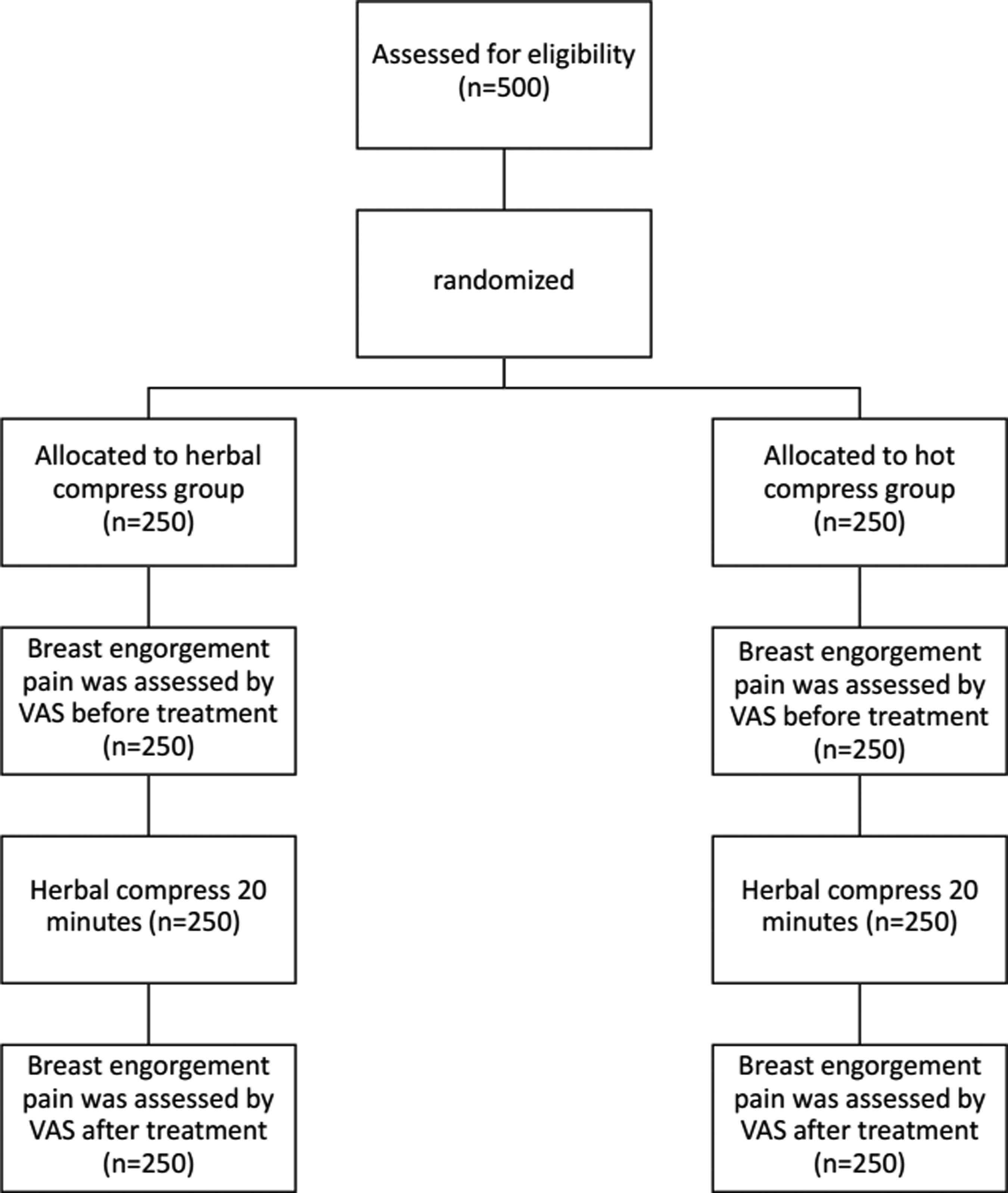
The flow diagram of participants through the study.
Age, income, BMI, time of breast engorgement, and baseline breast engorgement pain score data are expressed as mean ± SD. Marital status, education, occupation, route of delivery, breastfeeding experience, and breast engorgement grading are expressed as number (percentage).
BMI, body mass index; baht, basic monetary unit of Thailand.
There were statistically significant differences in the pain scores between both groups before and after treatment. The details of pain scores before and after treatment are shown in Table 2. There was a statistically significant difference between the two groups in the mean difference of pain scores before and after treatment (Table 3).
Pain scores in herbal and hot compresses are expressed as mean ± SD.
VAS, visual analog scale.
Mean differences of pain scores between two groups before and after treatment are expressed as mean ± SD.
All adverse effects recorded in the notes of both treatment groups were collected (500 cases). There were two cases (0.8%) with skin irritation in the herbal compress group and no cases had shown this adverse effect in the hot compress group. The skin irritation resolved without any additional treatment at the 24-hour follow-ups.
Discussion
The demographic data of both groups were similar from that expressed in randomization except baseline breast engorgement pain score. These factors include mothers' ages, marital status, education, income, occupation, route of delivery, body mass index, and breastfeeding experience that can affect breastfeeding practices and outcomes.7–11 Baseline breast engorgement pain score in the herbal compress group, higher than the hot compress group, might cause a higher number of grade-4 breast engorgements. However, this difference was not statistically significant. We found that the cesarean section rate was high in this study. The cesarean section factor might be associated with breast engorgement as it delays breastfeeding initiation and makes latching difficult. 12 When the infant did not extract milk, stasis was more likely. However, the association between cesarean section and breast engorgement was not reported in previous studies. 13 The body mass index mean was within an overweight range. The weight might also be associated with breast engorgement as it is associated with delayed initiation of breastfeeding. 10 The factors associated with breast engorgement should be investigated in further studies.
There was a statistically significant difference between the two groups in the mean difference of pain scores before and after treatment. It showed that the herbal and hot compresses could reduce pain from breast engorgement. This result is consistent with the Cochrane Database of Systematic Review of Mangesi and Zakarija-Grkovic; the hot packs could significantly decrease breast temperature, engorgement, pain, and discomfort at 5 and 30 minutes post-treatment. 14 Herbal compress treatments have been showed to significantly decrease breast pain and decrease the pain scores more effectively than hot compresses in this study. We believed that the pain reduction of herbal compress was caused by the elevated temperature and the herbs that were the components of the herbal compress balls. Plai or Z. cassumunar Roxb. rhizomes, C. longa L. rhizomes, and camphor had anti-inflammatory and analgesic effects.3–5 The other components had relaxation effects as seen in aromatic volatile oils. 6
The adverse effect of the herbal compress treatment was skin irritation. The skin irritation might be caused by an allergic reaction to some of the herbs used as components of the herbal compress balls. However, it was rare and resolved spontaneously and was not considered to be a serious complication. The safety of herbal compress use during lactation might be concerning as no active substances were investigated or measured in the breast milk. However, herbal compresses have been used for hundreds of years and is accepted for the analgesic and anti-inflammatory indications. These indications include labor pain reduction and milk induction. 6 It is approved and listed in the Thai National List of Essential Medicines.
The strength of this study is that it is a randomized controlled trial. The definition of breast engorgement and the methods of treatment have been clarified. Mothers reported the adverse effects in sealed envelopes to decrease any bias. We found that the high cesarean section rates and the mothers' body mass index within an overweight range might have contributed to breast engorgement. The association of these factors with breast engorgement is a limitation of this study. Further research is needed to evaluate any associative factors. Besides, there is no long-term follow-up with regard to engorgement; this is another limitation of the study and may be the next step in assessing the effect of herbal compresses.
Conclusion
The herbal compresses can decrease breast engorgement pain. The pain reduction after herbal compresses was greater than was seen in hot compresses. There were no serious complications after the herbal compress treatments.
Footnotes
Acknowledgments
Thanks to the HRH Princess Maha Chakri Sirindhorn Medical Center and the Faculty of Medicine, Srinakharinwirot University, for supporting our research.
Disclosure Statement
No competing financial interests exist.