
Abstract
Abstract
Objective:
To explore the effects of exclusive breastfeeding and its duration on the development of childhood and early adulthood obesity.
Materials and Methods:
A random sample of 5,125 dyad children and their mothers was extracted from a national database. With the use of a standardized questionnaire, telephone interviews were carried out for the collection of maternal lifestyle factors (e.g., breastfeeding). The body mass index was determined based on International Obesity Task Force criteria. Body weight and height of the offspring at the age of 8 was calculated from measurements derived from the national database, while the corresponding body measurements at early adulthood were self-reported.
Results:
Mothers who had breastfed or exclusively breastfed ≥6 months were 22.4% and 15.2%, respectively. Exclusive breastfeeding ≥6 months (versus never) was associated with a lower risk of overweight in childhood (8 years old; odds ratio [OR] = 0.89; 95% confidence interval [95% CI], 0.82–0.96) and adolescence/adulthood (15–25 years old; OR = 0.83; 95% CI, 0.68–0.97). Also, exclusive breastfeeding ≥6 months (versus never) was associated with a decreased risk of childhood and adolescence obesity by 30% (95% CI, 0.54–0.91) and 38% (95% CI, 0.40–0.83), respectively.
Conclusions:
Exclusive breastfeeding had a favorable influence on offspring's overweight and obesity not only in childhood but also in adolescence/adulthood.
Introduction
B
In Greece, the prevalence of exclusive breastfeeding practices is far away from global recommendations. 6 Exclusive breastfeeding practice is affected by a wide range and complicated combination of factors, including family and maternal sociocultural demographics, biomedical factors, healthcare system, psychological factors, public health, and social support, besides the promotion of commercial formula milk.7–9
Breastfeeding is a crucial strategy to prevent the development of overweight/obesity and its complications not only in childhood but also in the long term.10,11 Breastfeeding may not be a panacea for the treatment of obesity, but it is one of the most easily applicable strategies as it combines both low cost and high efficacy.12,13 In Greece, findings showed that children who were exclusively breastfed were 0.49 and 0.54 times less likely to be overweight at the age of 6 and 12 months, compared with those who were not. 14
In our country, the available representative data on the frequency and duration of exclusive breastfeeding, as well as its longitudinal correlation with the development of childhood and adulthood obesity, are limited.6,14
Thus, we aimed to examine the effects of exclusive breastfeeding and its duration on the development of childhood and early adulthood obesity through a broad representative epidemiological research in Greece.
Materials and Methods
Study design
Population-based data were derived from 10 national, school-based health surveys. The national database included anthropometric data and information on age, gender, city and area, home address, and telephone number, which were collected yearly, at the same time period (spring), from 1997 to 2007, in almost all schools of primary education (roughly 85%). Thus, from 1997 to 2007, a total of 651,582 eight- to nine-year-old children (51% boys and 49% girls; over 95% of the total student population) participated in the study. Measurements were performed by two trained physical education (PE) teachers in each school. PE teachers followed a specific protocol taught in corresponding seminars held by the Greek General Secretariat of Sports.
Data extraction
A sample of 5,500 children (0.8% of the entire population) was randomly extracted from the database and their mothers were contacted telephonically. Random extraction was performed with a statistical software. The number of 5,500 subjects was adequate to achieve statistical power greater than or equal to 99% for evaluating 0.10 ± 0.05 changes in regression coefficients at 5% significance level of two-sided tested hypotheses. The random sampling was stratified according to the region and place of living (e.g., rural/urban), according to the National Statistical Agency and equally distributed during the study period (i.e., 500 mothers per year).
Information of the proposed protocol was collected through telephone interviews based on computer-aided telephone interview method. To validate the process, 100 face-to-face interviews were conducted to check for discrepancies with the information collected via telephone. No such discrepancies were noted in any of the variables evaluated.
Measurements
All the necessary information was collected using a standardized questionnaire, named the Childhood Obesity Pregnancy Determinants (ChOPreD) questionnaire, designed and developed in collaboration with the Harokopeio University Department of Nutrition and Dietetics and Department of Geography and the University of Texas Medical Branch Department of Internal Medicine. The ChOPreD questionnaire was tested and internally revised by study investigators during a pilot study, which confirmed its construct validity. During data collection, the mothers were asked to provide information from their pregnancy ultrasound records (e.g., body weight) and recall certain information (e.g., smoking patterns, alcohol consumption).
Mothers in Greece have ultrasounds at the start of pregnancy and several times during its progress and receive records of the results. Only mothers who had full set of records were included in the study, which finalized the sample of 5,125 mother–children dyads. Data recall relating to the perinatal period is very common in pregnancy-related studies. Also, recall of breastfeeding practice is considered a valid and reliable estimate. 15
The body mass index (BMI) data of children at the age of 8 years was calculated based on data retrieved from the national database. In addition, mothers provided self-reported anthropometric characteristics (body weight and height) of their children at the follow-up age (15–25 years old). A review of studies has shown that self-reported anthropometric data is valuable if it is the only source of data, although they underestimate the prevalence of overweight. 16 Also, it is considered that self-reported reports of anthropometric characteristics of young people when provided by their parents are better indicators of obesity status of young people.
However, according to researchers, using BMI based on self-reported anthropometric characteristics places 96% of the weight in the correct weight class, and therefore researchers can use self-declared weight and height to estimate obesity status of young people and its correlations. 17 BMI status of the offspring at the age of 8 and in early adulthood was determined based on cut-off points suggested by the International Obesity Task Force. 18
Main outcome
Mothers were asked whether they had breastfed their offspring, and, if so, what was the duration (in months) of (1) exclusive breastfeeding and (2) overall breastfeeding. Breastfeeding is a special practice among most mothers; so they can easily recall details about it.
Study approval
The study was approved by the Bioethics Committee of Harokopio University. Oral approval was obtained from all mothers who agreed to participate in the study. Written informed consent was obtained from those participants who took part in the validation process of the study.
Statistical analysis
Continuous variables are presented as means ± standard deviations given that they were normally distributed (as examined by the use of histograms and P–P plots). Categorical variables are presented as frequencies. The chi-squared test evaluated associations between categorical variables, and the Student's t test was applied to evaluate differences in mean values of normally distributed variables. Furthermore, to assess the potential effects of exclusive breastfeeding and its duration (<1 versus 1–5 months and <1 versus ≥6 months) on BMI, overweight, and obesity in childhood and adulthood, binary logistic regression analysis was implemented and odds ratio (OR) with the corresponding 95% confidence intervals (CIs) were calculated.
The Hosmer and Lemeshow's goodness-of-fit test was calculated to evaluate the model's goodness-of-fit, and residual analysis was implicated using dbeta, the leverage, and Cook's distance D statistics to identify outliers and influential observations. All analyses were performed using SPSS version 23.0 software for Windows (SPSS, Inc., Chicago, IL). Statistical significance level from two-sided hypotheses was set at 5% level (p ≤ 0.05).
Results
The number of mothers who did not have full set of data were 192 (3.5%). Also, the number of mothers who did not want to participate in the study were 183 (3.3%). Table 1 presents maternal, paternal, and offspring characteristics of the study sample. In the current study, percentages of mothers who had breastfed or had exclusively breastfed their offsprings for ≥6 months were 22.4% and 15.2%, respectively (Fig. 1). Table 2 shows demographic and clinical characteristics of children and their mothers by exclusive breastfeeding duration (e.g., <1, 1–5, and ≥6 months). The BMI at the age of 8 years and at follow-up of offspring who were exclusively breastfed ≥6 months was lower than those who were exclusively breastfed <1 month.
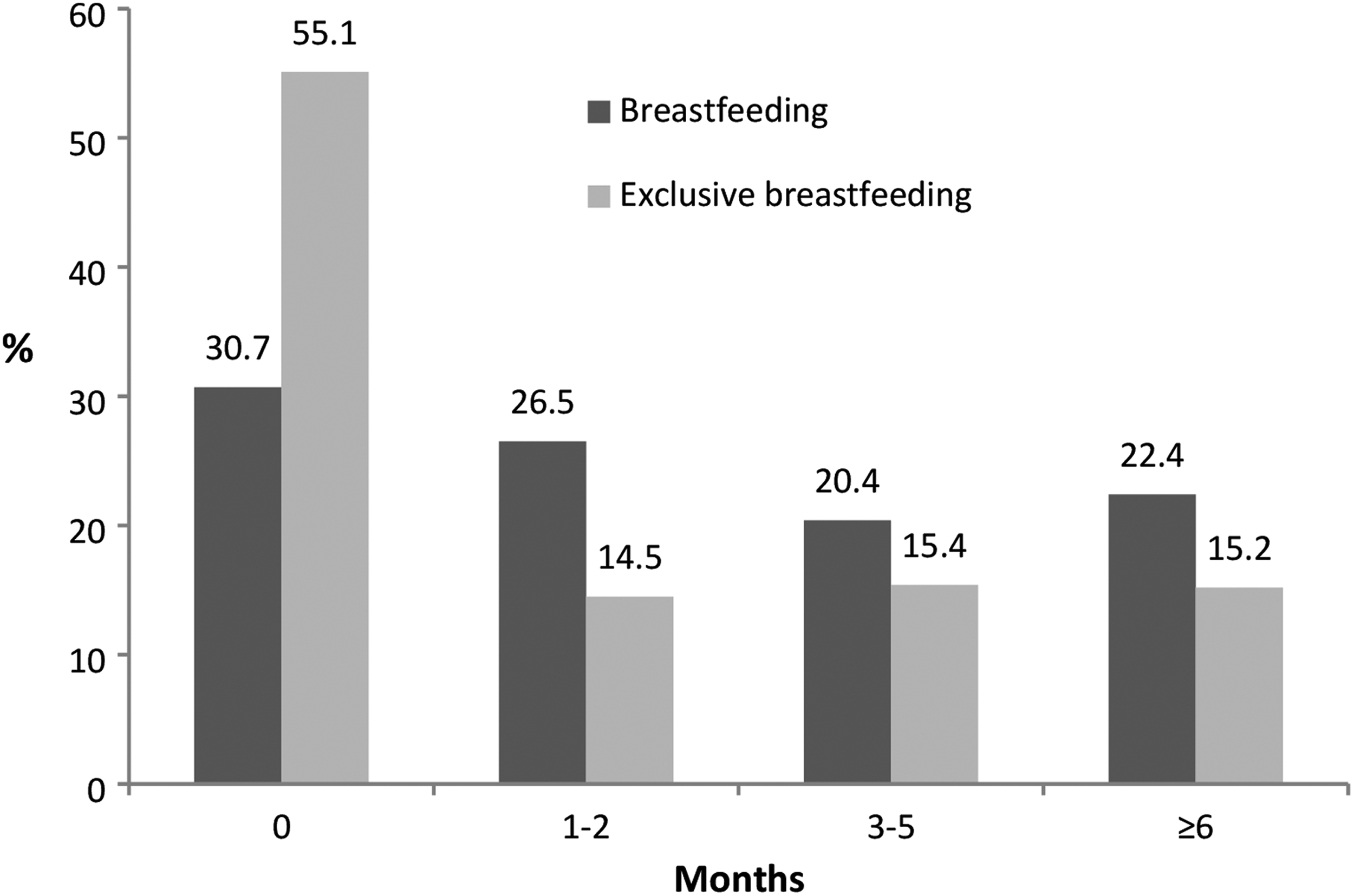
Prevalence (1997–2007) of breastfeeding and exclusive breastfeeding among 5,125 Greek mothers.
BMI, body mass index; GWG, gestational weight gain; IOM, Institute of Medicine.
Fewer obese mothers at first visit had exclusively breastfed ≥6 months than normal-weight ones (p < 0.001), while more mothers who had gained excess weight during pregnancy had exclusively breastfed their offspring compared with those who gained adequate weight (p = 0.006).
Considering that BMI of offspring at the age of 8 and later in early adulthood was lower in those children who were breastfed ≥6 months compared with those who were not, we performed binary logistic analysis to explore the effects of duration of exclusive breastfeeding on BMI, overweight, and obesity in childhood and adolescence/adulthood. The analysis revealed that increasing BMI (per one union, kg/m 2 ) decreased the odds of exclusive breastfeeding ≥6 months by almost 6% (95% CI, 0.90–0.98) in both genders (Table 3). Furthermore, after adjusting for several potential confounders, the results of the whole sample revealed that duration of ≥6 months of exclusive breastfeeding was associated with a lower risk of becoming overweight in childhood (8 years) and adolescence/adulthood (15–25 years; Table 3). This protective association was consistent for both boys and girls.
Overweight and obesity were defined according to International Obesity Task Force criteria.
OR, 95% CI: After adjusting for maternal characteristics (educational status, nationality, prepregnancy weight status, gestational weight gain, and parity before).
CI, confidence interval; EBF, exclusive breastfeeding; OR, odds ratio.
Moreover, exclusive breastfeeding ≥6 months had a significantly inverse association with the risk of obesity among boys and girls. Specifically, in the total sample, more than 6 months (versus never) of exclusive breastfeeding was associated with a decreased risk of childhood and adolescence obesity by 30% (95% CI, 0.54–0.91) and 38% (95% CI, 0.40–0.83), respectively (Table 3).
Discussion
To the best of our knowledge, the current study is among few studies aimed to present the effects of exclusive breastfeeding on the development of childhood and early adulthood obesity. Data from this representative cohort revealed that ≥6 months of exclusive breastfeeding decreased the risk of developing obesity in childhood and adulthood, even after adjusting for several covariates.
The results of this survey showed that the percentage of women who had breastfed was 60.3%, while those who had exclusively breastfed accounted for 44.9%. Nearly the same findings were revealed by another study in our country, which reported percentages of 70.2% and 30.4%, respectively. 14 Moreover, the current study showed that only about 15% of mothers had exclusively breastfed. Among European countries, it has been suggested that breastfeeding frequency and duration were higher in countries such as Sweden, Finland, and Austria, compared with countries such as Italy, Greece, and the United Kingdom. 19
The present study suggests that more mothers of non-Greek nationality as compared to those with Greek nationality had exclusively breastfed ≥ 6 months. One study in our country revealed that ethnicity was associated with the duration of exclusive breastfeeding, 20 while in another study immigrant status was found to be significant for breastfeeding initiation. 21 Potentially, different cultural norms, immigration, and lower economic status could influence the preference and duration of exclusive breastfeeding.
Our findings proposed that fewer prepregnancy overweight/obese mothers had exclusively breastfed ≥6 months compared with normal-weight ones. One study in the United States, including a huge sample of 1,161,949 unique observations, proposed that obese women had 20% lower probabilities to initiate breastfeeding, 22 while Castillo et al. found that offspring from prepregnancy overweight/obese mothers had higher possibility of early weaning compared with offspring from normal-weight mothers. 23
More mothers with excess weight gain had exclusively breastfed their offspring than those with adequate weight gain. Studies from other countries have published conflicting results. Specifically, one study among Norwegian mothers indicated that gestational weight gain (GWG) above recommendations adds to the risk of inability to initiate or sustain breastfeeding, 24 while another study among Brazilian and U.S. mothers concluded that GWG was not associated with exclusive breastfeeding initiation and duration.23,25 Perhaps the different results could be attributed to the sample sizes (representative or not), metabolic and/or social factors, as well as adequate support from the healthcare system toward breastfeeding. 26
In this study, only one to four mothers who gave birth to low-birthweight offspring breastfed (>1 month) exclusively. A review assessing breastfeeding to low-birthweight infants concluded that exclusive breastfeeding was reported in 11.1% in the cohort studies and 31.2% in randomized control studies. 27 Also, a previous review including seven prospective randomized trials conducted between 1990 and 1997 showed that only 4% of low-birthweight infants were exclusively breastfed. 28
Less educated mothers who participated in the current study were more likely to exclusive breastfeed ≥6 months than those with secondary/higher education. However, the analysis revealed that a lower proportion of mothers with basic education (<6 years) had exclusively breastfed from 1 to 5 months compared with mothers with secondary and higher education. Research conducted among five counties in Greece showed that higher maternal education decreased the probability of breastfeeding initiation. 6 In general, it seems that in industrialized countries, women who breastfeed less were most commonly found to have a low level of education. 29
Exclusive breastfeeding is probably a critical factor in reducing the risk of overweight/obesity during both puberty and adulthood.1,2 As concerning the influence of duration of exclusive breastfeeding on BMI status, our data indicated that exclusive breastfeeding time was associated with lower odds of overweight and obesity at the age of 8 as well as during adolescence/adulthood. Specifically, we found that exclusive breastfeeding ≥6 months connected favorably with BMI in childhood and adolescence/adulthood. Also, offspring who were breastfed 1–5 months had 19% and 24% decreased odds of obesity in childhood and adolescence/adulthood, respectively, than those who were not.
In addition, exclusive breastfeeding ≥6 months reduced the odds of overweight (11% and 13% in childhood and adolescence/adulthood, respectively) and obesity (30% and 38% in childhood and adolescence/adulthood, respectively) compared with non-breast-feeders.
Several meta-analyses have been published in this field, which supports the beneficial effects of breastfeeding on body composition across the life.15,16,30 In line with our results, a meta-analysis by Owen et al. speculated that breastfeeding was associated with a slightly lower mean BMI (by an average of 0.04 kg/m 2 ) compared with formula feeding in later life. 31 Similar to the current results, a recent meta-analysis showed a 15% reduction in the risk of childhood overweight/obesity of offspring who were breastfed relative to those who were not. 31 Also, a meta-analysis by Arenz et al. has found that children who were breastfed presented 22% less obesity risk compared with those who were not. 13 Moreover, another meta-analysis concluded that breastfeeding was associated with a decreased risk of obesity in later life, compared with formula feeding (OR = 0.87; 95% CI, 0.85–0.89). 32 In Greece, it has been proposed that children who were exclusively breastfed were 0.49 and 0.54 times less likely to be overweight at the age of 6 and 12 months than those who were exclusively fed formula milk. 14
The main strength of this work is that it explored the influence of exclusive breastfeeding on offspring's BMI status at two different developmental stages (e.g., childhood and adolescence/adulthood) using a large, representative sample.
Limitations
The information that was collected during telephone interviews was self-reported. Therefore, although mothers could provide information for self-reported pre-pregnancy data based on health records, deliberate overreporting, underreporting, or recall bias can not be excluded.
Conclusions
Exclusive breastfeeding had a favorable influence on offspring's overweight and obesity not only in childhood but also in adolescence/adulthood. Healthcare professionals should recommend mothers to exclusively breastfeed their offspring as long as possible.
Footnotes
Acknowledgments
We wish to thank the study subjects for their willingness to participate. We are also very grateful to Mrs. Stavroula Parastatidou, Markella Symeopoulou, and Mema Lampropoulou for their assistance with data collection.
Disclosure Statement
No competing financial interests exist.