
Abstract
Abstract
Introduction:
The protective effects of breastfeeding against developing breast cancer are well known; however, it is unknown whether women are aware of this breastfeeding benefit.
Research Aim/Questions:
The aim of this investigation was to determine whether mothers received information about breast cancer risk reduction during breastfeeding counseling and whether this knowledge affected their decision to initiate and sustain breastfeeding.
Materials and Methods:
The survey was conducted at The Ohio State University Comprehensive Cancer Center with women aged 18–50 who had at least one live birth. Participants were recruited through primary care practice and a national clinical research registry.
Results:
Six hundred sixty-seven (92%) of the 724 respondents breastfed. Over half of them (56%), that is, 407 women (60.4% Caucasian, 46.9% African American), were aware before their most recent childbirth that breastfeeding reduced the risk of breast cancer. Of the 407 women, 36.4% said this knowledge affected their decision to breastfeed. Of the 39 who did not breastfeed, 23 women (59.0%) responded that awareness of risk reduction would have influenced their decision to breastfeed. Only 120 of 724 respondents (16.6%) received this information from healthcare providers. Women with this knowledge breastfed longer than those without this knowledge (13.2 versus 9.3 months; p < 0.001). More Caucasian women (76.4%) breastfed any one child for more than 6 months compared with African American women (63.2%; p = 0.011; chi-squared test).
Conclusion:
While several factors affect the initiation and duration of breastfeeding, this study demonstrates that knowledge of association between breastfeeding and breast cancer risk reduction may influence breastfeeding practices. Our study illustrates the need for improved counseling for mothers by healthcare providers regarding this benefit.
Introduction
T
During the pregnancy–lactation cycle, breasts undergo permanent changes that may play a role in breast cancer risk. 4 Most breast cancers arise from functional structures of the breast, called terminal duct lobular units (TDLUs). TDLU involutions increase with breastfeeding and reduce the risk of breast cancer. 5 In 1926, Lane-Clayton identified an association between breast cancer and breastfeeding; specifically, women who did not breastfeed were more likely to develop breast cancer. 6 The protective effects of prolonged breastfeeding against developing breast cancer have been identified in many populations through epidemiological studies.7–9 For every 12 months of lifetime duration of breastfeeding, breast cancer risk is reduced by 4.3% (p < 0.0001). 10 Among women who inherit the BRCA1 mutation, breastfeeding for at least 1 year results in a 32% risk reduction in breast cancer, and the risk reduction is even greater in those who breastfeed for at least 2 years. 11 Breastfeeding has been shown to have a particularly protective effect against highly aggressive triple-negative breast cancer, which is especially prevalent among African American women.12,13
Breast cancer and breastfeeding statistics are highly variable by race. Of the racial groups in the United States, African American women have the lowest rates of breastfeeding with 60% “ever breastfeeding” and 28% sustaining breastfeeding at 6 months, compared with Asian women at 86% and 59%, respectively. 14 This is particularly important to note as African American women have a disproportionate burden of developing aggressive triple-negative breast cancer, and studies have shown that breastfeeding for at least 6 months reduces this risk.12,13 A study that conducted pooled analyses of reproductive factors and risk of triple-negative breast cancer in Caucasian and African American women showed that parous African American women aged 20–44 years who breastfed for 6 months or longer had an 82% lower risk of developing TNBC compared with African American women who never breastfed. 15 Some of the breastfeeding practice discrepancies in black women have been explained by social barriers such as lack of cultural breastfeeding acceptance and supportive breastfeeding practices in underserved communities. 16
Despite the strong epidemiological evidence regarding prolonged breastfeeding and reduced risk of breast cancer, the United States has not met the Healthy People 2020 goal for breastfeeding. In addition, there is no published data to demonstrate how much of this data regarding breast cancer risk is shared with mothers that could influence their awareness before making a decision to breastfeed. Therefore, we designed a survey to assess women's knowledge before their most recent childbirth about the benefits of breastfeeding as it relates to breast cancer prevention.
Our study assessed the knowledge of breast cancer risk reduction from breastfeeding in community and primary care-based populations of women who had at least one live-born child, as well as the breastfeeding patterns of these women. The primary goal of this study was to assess whether breast cancer risk reduction was part of breastfeeding counseling among our participants, as well as within the national population. The secondary goal was to assess whether participants believe this knowledge affected their decision to breastfeed and also to evaluate how these factors were affected by race and other sociodemographic variables.
The key findings from this study demonstrate a need to modify clinical messaging designed to improve patient education about the benefits of breastfeeding related to breast cancer.
Materials and Methods
This was a descriptive cross-sectional survey study developed by us at The Ohio State University Comprehensive Cancer Center (OSUCCC) to assess women's knowledge on the benefits of breastfeeding as related to the risk reduction of developing breast cancer (IRB Protocol Number 2016H0103). The survey study received approval before initiation by the local institutional review board, and responses to the survey were deidentified.
Inclusion criteria included women who aged 18–50, had at least one live-born child, and were able to read and comprehend English. Consenting women were provided a link to a survey administered through Research Electronic Data Capture (REDCap), a software application for managing online surveys and databases.
Our study was approved by the OSU institutional IRB in September 2016. Participants were recruited from primary care practices and from the community. Community participants were identified through Research Match, a national clinical registry pairing investigators and potential study participants. A total of 34,143 surveys were distributed through Research Match, while 851 surveys were sent through MyChart-Epic Systems. There were a total of 724 responses, and the study was closed to accrual in June 2017. The survey (Supplementary Appendix A; Supplementary Data is available online at www.liebertpub.com/bfm) was developed by the investigators of internal medicine and oncology departments with guidance from a database development team of behavioral measurement. This resource assisted investigators to incorporate behavioral research into cancer research by helping with research design, participant recruitment and accrual, and population-based data retrieval. The survey had a total of 20 questions that required objective responses regarding knowledge and other demographic data, excluding any open-ended questions. The survey pilot was forwarded to the study team, and it approximately took 10 minutes to complete. The main goal of the survey was to assess patients' knowledge of breast cancer risk reduction from breastfeeding. Therefore, this survey was not a validated tool.
Eligible primary care participants were identified by their primary care physicians through systematic screening of patient panels and were then messaged a link to the survey upon informed consent through secured patient portal messaging (also known as MyChart-Epic Systems).
An email describing the survey process, aims, and inclusion criteria was sent to participants who were able to provide consent by clicking on the link to complete the survey. Anonymity and confidentiality were assured as completed surveys were deidentified in REDCap. Women were not compensated for their participation.
All data analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC). Descriptive statistics was used to describe patient characteristics, including means and standard deviations or medians for continuous variables, and proportions for categorical variables. Survey questions with yes/no or multiple choice responses were compared between patient socioeconomic characteristics such as race using chi-squared or Fisher's exact tests. Duration of breastfeeding (responses to questions 9 and 10) was converted to months and were compared between patient socioeconomic characteristics (questions 14–19) using a Wilcoxon rank sum test. A p-value of 0.05 or less was considered statistically significant.
Results
Survey links were sent to a total of 34,994 women aged 18–50, with 34,143 surveys sent through Research Match and 851 through MyChart. A total of 724 women completed the online survey, answering all the key questions: 503 responses through Research Match, 197 through MyChart, and 24 did not specify method of survey access (Fig. 1). Of the participants, 454 responded as Caucasian only, 130 as African American only, and 140 responded with multiple races/other/unknown (Table 1). A vast majority (92%) of respondents breastfed at least one child.
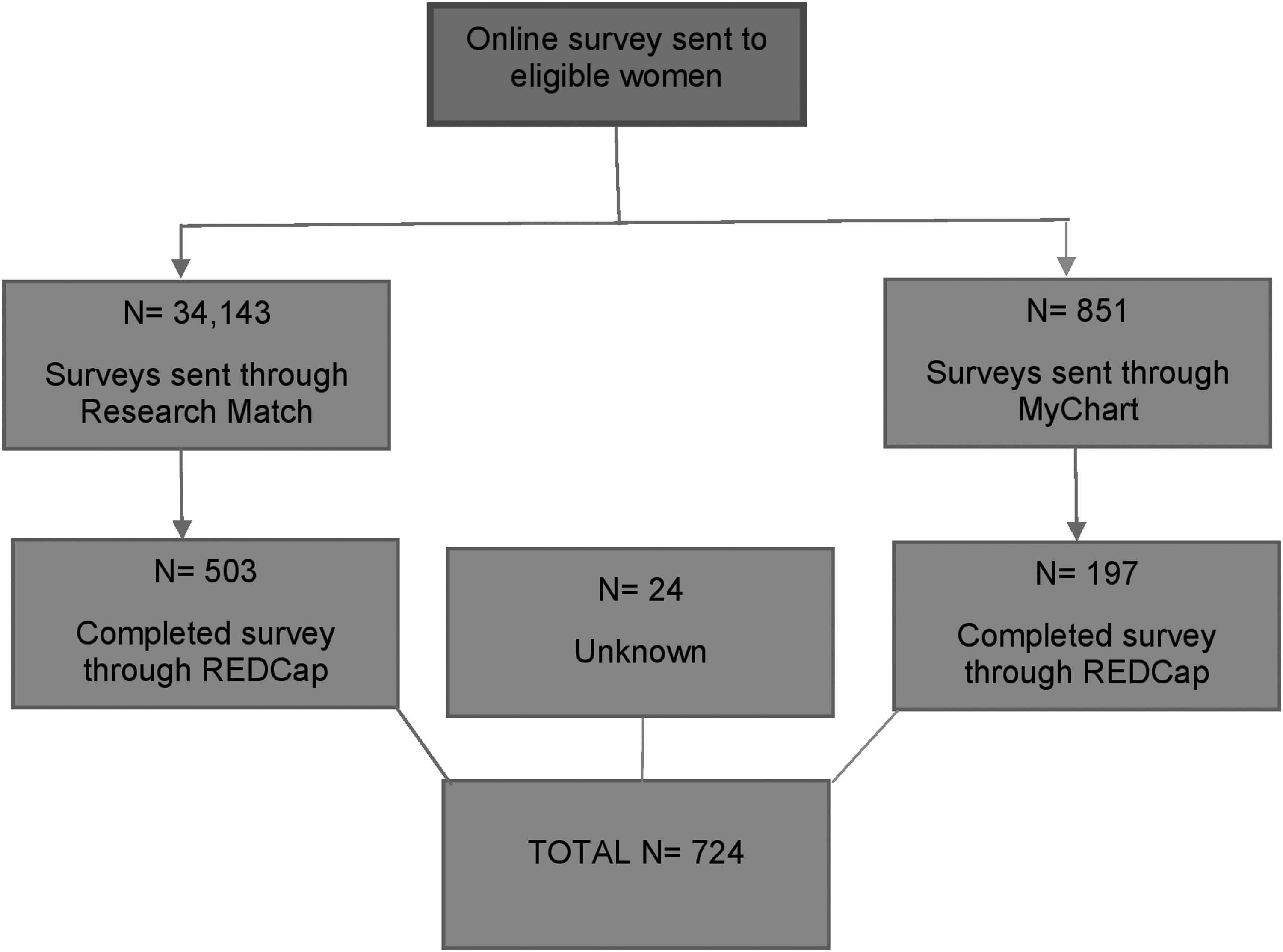
Survey administration: Number of eligible women (N) who were sent surveys through Research Match and MyChart, and of those women, the number who completed the survey on REDCap. REDCap, Research Electronic Data Capture.
Fifty-two women responded more than one race, including white and black. The numbers are those who selected ONLY white or ONLY black.
SD, standard deviation.
When assessing knowledge, 56.2% said they were aware that breastfeeding reduces the risk of cancer. The proportion of women who said they were aware that breastfeeding reduces the risk of cancer differed significantly by race (p = 0.011; Caucasian 60.4%, African American 46.9%, and multiple/other/unknown race 51.4%). The longest time any one child was breastfed among women who were aware of this benefit was significantly longer than the women who were not aware (mean, 13.2 versus 9.3 months, respectively; p < 0.001). Of those who were aware of the benefit, 36.4% said this knowledge affected their decision to breastfeed. Interestingly, only 16.6% of women reported they received this information from healthcare providers, and others obtained this information mainly through magazine articles/books (31.8%) and the internet (29.6%).
Fifty-six (8%) of the women surveyed did not breastfeed. Of the 39 women who did not breastfeed and were unaware of the association between breastfeeding and breast cancer risk reduction, 23 (59%) acknowledged that if they had been aware of this risk, it would have influenced their decision to breastfeed.
As a secondary objective, we found that racial and educational differences had an impact on the length of time women breastfed. About 44.6% of African American women breastfed any one child for less than 6 months compared to 29.3% of Caucasian women and 30.7% of women who responded multiple/other/unknown race. Also, more women with a high school degree or below breastfed any one child for less than 6 months (59.1%) compared to women with some college or higher (30.1%). Most women (66.3%) returned to work within the first year of their most recent childbirth, and 39.2% of women indicated returning to work as a barrier to breastfeeding (Table 2). Other barriers included not producing enough milk, nipple damage and sores, and unsuccessful latching by the child.
Twenty-five respondents had missing data for education level.
One respondent had missing data on the number of children being breastfed.
Column percentages do not add up to 100%, respondents chose more than one response.
Sixty-eight respondents had missing data for time of returning to work since childbirth.
Discussion
Multiple epidemiological studies have shown that breastfeeding for at least 6 months reduces the risk of developing breast cancer, in particular, the aggressive triple-negative breast cancer.12,13 This is apparent even in patients with the BRCA1 mutation who had a 37% reduction in breast cancer risk after breastfeeding for at least 1 year. 17 Despite this enormous health benefit for the mother, only 51.8% of U.S. infants born in 2013 were breastfed through 6 months. Multiple barriers have been cited for this lack of breastfeeding initiation and maintenance. 3 Therefore, we sought to study whether mothers were aware of breast cancer risk reduction and whether that awareness had an impact on their breastfeeding practices.
A little more than half of the women surveyed stated they were aware that breastfeeding reduces the risk of breast cancer and around a third of these women said that this knowledge had an impact on their decision to breastfeed. For the women who were not aware and did not breastfeed, over half of them stated that such an awareness could have influenced their decision to breastfeed. Though we acknowledge the limitation in sample size, this still raises concern about the lack of clarity of message, information, and consultation from healthcare providers.
Previous studies have indicated a lack of effective education on the benefits of breastfeeding for younger women. Polek and Hardie demonstrated through a survey administered among high school students that ∼20% believed breastfeeding actually increases their risk of breast cancer. 18 This suggests a need to start breastfeeding education at an earlier age. Other studies have shown that healthcare providers have a significant impact on breastfeeding habits. One study that focused on obese mothers and their breastfeeding habits concluded that breastfeeding support from physicians or other health professionals had the most significant impact on the initiation and 6-month continuity of breastfeeding in both obese and nonobese patients. 19 In a study that explored African American women's experiences with breastfeeding, it was shown that efforts that promoted breastfeeding in this population included encouragement from the healthcare provider, knowledge of the benefits of breastfeeding, and assistance from support groups or classes. 20
Our study showed that only 16.6% of women learned this information through their healthcare providers, while most discovered the information from online sources or magazines and books. This is important to note as previous studies have indicated the impact of counseling from healthcare providers.
As a secondary objective, our study examined breastfeeding patterns between African American and Caucasian women. In our study, just under half of African American women were aware of the impact of breastfeeding on their breast cancer risk. Though the response rate was lower among African American women compared with Caucasian women, we still saw a trend that a greater percentage of Caucasian women breastfed for longer than the recommended 6 months compared with African American women. This is especially concerning given the association of lack of breastfeeding and risk of developing the aggressive triple-negative breast cancer, which is more prevalent among African American women and one of the attributed causes of higher mortality among African American women diagnosed with breast cancer.13,21,22 An editorial discussing the results of AMBER consortium study (African American Breast Cancer Epidemiology and Risk) stated that parous African American women have a lower prevalence of breastfeeding compared with parous non-Hispanic white women, confirming results from our study. Phipps and Li also analyzed the relationship between the incidence of triple-negative breast cancer among African American women and breastfeeding patterns, explaining that increased breastfeeding would lead to a decrease in the incidence of triple-negative breast cancer by two-thirds. 23 Another study that conducted pooled analyses of reproductive factors and risk of triple-negative breast cancer among Caucasian and African American women showed that parous African American women aged 20–44 years who breastfed for 6 months or longer had an 82% lower risk of developing TNBC compared with African American women who never breastfed. 15
Some other ethnicities have various motivators to breastfeed, such as reinforcement from their family and culture. Parous Hispanic women said they were encouraged to breastfeed due to the support and motivation from their relatives. Reasons for choosing formula feeding in the United States among this Hispanic population included embarrassment and need to return to work. 24 In a study among Malay women, it was noted that higher education and breastfeeding counseling had the greatest impact on women's beliefs on the benefits of breastfeeding. 25 Hence, these studies highlight the importance of culturally relevant communication strategies and healthcare counseling. The knowledge of the relation between breastfeeding and breast cancer is not universal, and increased awareness and support from healthcare providers with effective communication could impact the decision to initiate and maintain breastfeeding.
Many initiatives to increase breastfeeding rates focus on lactation groups, training and educational facilities, and immediate postpartum exclusive breastfeeding in the hospital. 3 Though professional support has been cited as a primary motivator in breastfeeding, this study revealed that education regarding breast cancer risk reduction through breastfeeding is not routinely discussed by the healthcare provider. Including information about breast cancer risk reduction in relation to breastfeeding as part of obstetric and postpartum counseling may have a substantial impact on increasing breastfeeding and consequently breast cancer prevention, particularly TNBC. In addition, our findings are relevant in addressing disparities in breast cancer mortality between African American and Caucasian women. African American women have a 39% higher risk of dying from breast cancer, and at least part of this discrepancy is attributed to the higher incidence of TNBC in this population. 26 Reducing incidence of this subtype of breast cancer through improved awareness is an important public health concern.
It is important to note the limitations of this study. Most of the women who responded to the survey (92%) reported they breastfed. This percentage is higher than what we would expect based on the 2016 Breastfeeding Report Card. 3 The vast majority of those surveyed nationally were through Research Match. The subscribers to this research database, as well as MyChart users, might contribute to selection bias as certain groups may be more motivated to respond or have access to this system. Another limitation is that this was not a validated survey and was developed by researchers at OSUCCC to investigate our aims. We also acknowledge that an increase in the duration of breastfeeding noted in the study is not solely attributed to the knowledge of breast cancer risk reduction as other variables, including various barriers, influence breastfeeding habits as well.
Lastly, participants were asked to recollect information and decision making regarding their past pregnancies, and this could have resulted in recall bias.
Conclusion
Consistent delivery of healthcare-based counseling on breast cancer risk reduction through prolonged breastfeeding can potentially improve the rates of breastfeeding initiation and maintenance. We showed that there are disparities among African American and Caucasian women in their knowledge that breastfeeding reduces the risk of breast cancer, which appears to have an impact on breastfeeding decisions. Hence, the development of culturally relevant communication strategies, especially for African American women, in addition to addressing other barriers can impact the initiation and maintenance of breastfeeding and ultimately result in the reduction of breast cancer risk and mortality.
Footnotes
Acknowledgment
The work was funded by Stefanie Spielman Breast Center funds.
Disclosure Statement
No competing financial interests exist.