
Abstract
Purpose:
To test the feasibility and possible effects of two iPad®-based breastfeeding interventions for expectant minority women and evaluate (1) the intervention effect on exclusive breastfeeding (EBF) intention, (2) intervention acceptability and satisfaction, and (3) follow-up rates of in-hospital EBF.
Materials and Methods:
This was a longitudinal survey study with follow-up chart review. Expectant women who completed clinically required breastfeeding education were eligible and were assigned to one of the following interventions by nonrandomized block design: the champion intervention utilized a free commercially available app to identify a supportive breastfeeding champion and the positive messaging intervention offered breastfeeding information in a question–answer format. Medical records were reviewed postpartum for in-hospital feeding choice. Data were analyzed using percentages, frequencies, chi-squared analyses, and McNemar's test.
Results:
We enrolled 243 publicly insured predominantly African American women: 132 and 111 completed the champion and positive messaging interventions, respectively. Thirty-two of 40 champion participants (80.03%) intended EBF and did in-hospital EBF; 39/86 champion participants (45.3%) not intending EBF did in-hospital EBF (p < 0.0001 for change). Similarly, 30/36 positive messaging participants (83.3%) intended EBF and did in-hospital EBF; 36/67 positive messaging participants (53.7%) not intending EBF did in-hospital EBF (p < 0.0001 for change).
Conclusions:
In this pilot of two brief, iPad-based prenatal interventions designed to promote in-hospital EBF among minority women, interventions were feasible and a statistically significant change in the proportion of women who intended (prenatally) and then chose (postpartum) EBF was noted. Additional controlled trials are needed to demonstrate the effectiveness of this approach.
Introduction
The evidence-based benefits of breastfeeding for the infant and mother are well known.1–3 Exclusive breastfeeding (EBF) through 6 months, followed by continued breastfeeding and addition of complementary foods, is endorsed by consensus of the World Health Organization (WHO), the American Academy of Pediatrics, the American College of Obstetrics and Gynecology (ACOG), and multiple other professional bodies.1–3 The Baby-Friendly Hospital Initiative (BFHI), launched by the WHO and UNICEF in 1991, aims to implement maternity practices that support, promote, and protect breastfeeding. 4 BFHI designation is associated with improved long- and short-term breastfeeding outcomes, including increased breastfeeding initiation, duration and exclusivity, and in-hospital EBF. 5 Although a sample of U.S. BFHI-designated hospitals had 13.6% higher rates of in-hospital EBF than those without designation, there was meaningful variation between hospitals, with less than half of the variability explained by either BFHI designation status or by the number of BFHI Ten Steps practices to which birthing hospitals adhered, even after controlling for demographic differences between hospitals. 6
Women's prenatal intentions regarding breastfeeding are the strongest predictors of their postnatal breastfeeding decisions, and this appears to be independent of race and other sociodemographic factors.7–10 However, even at BFHI-designated birthing hospitals with high rates of breastfeeding initiation, studies continue to demonstrate that low-income minority women are less likely to exclusively breastfeed in the hospital.10–12 Nationally, 17.2% of infants receive formula before the age of 2 days (breastfeeding report card), and this rate is higher among non-Hispanic African American mothers (20.9%) than non-Hispanic Caucasian mothers (12.7%), evidencing racial disparities well described for initiation and duration of breastfeeding.13,14 For example, Lewkowitz et al. found that among low-income minority women at a BFHI-designated hospital, 129 (86.8%) initiated breastfeeding, but by day 2, just 47 (31.5%) were exclusively breastfeeding and 51 (34.2%) were combining formula with breastfeeding. 12 Similarly, in a predominantly African American inner-city population also delivering at a BFHI-designated birthing hospital, of women who intended EBF, 74% did EBF postpartum, while 14% combined breastfeeding and formula, and 12% exclusively formula fed. 10 In a population delivering at a non-BFHI-designated birthing hospital, and including predominantly minority and Medicaid-insured mothers, of those who intended to breastfeed exclusively, just 40% were doing so at discharge. 15 Thus, although intention predicts choice, EBF rates are lower among minority women regardless of the birthing hospital's BFHI designation status. Interventions to support in-hospital EBF, particularly for minority populations, are urgently needed.
The cause of decreased EBF among minority mothers appears to be multifactorial and may include a higher level of comfort with formula feeding, absence of personal support for breastfeeding, availability of free formula from the Special Supplemental Feeding Program for Women, Infants, and Children (WIC) despite WIC's breastfeeding supportive peer counseling, mistrust of mainstream medical advice, and societal and structural racism impacting health care access and beliefs.16–18 Two systematic reviews of interventions to promote breastfeeding among minority women have identified a total of 29 studies on interventions promoting and supporting breastfeeding among minority women.19,20 Chapman et al. reviewed 22 eligible studies and identified specific interventions that improved breastfeeding among minority women, including peer counseling, breastfeeding teams consisting of a peer counselor working with a health professional, group prenatal classes, breastfeeding-specific office appointments, and hospital and WIC policy changes. 19 Adding to this review, Jones et al. identified additional barriers specific to minority women, including negative perceptions of breastfeeding in the African American community and the absence of, or reduced access to, information that supports and promotes breastfeeding. 20 They identified seven additional studies with interventions targeting minority populations and reported that peer counseling and hospital- and WIC-based, enhanced breastfeeding programs appeared effective in increasing breastfeeding rates. While ACOG strongly supports breastfeeding, evidence regarding the impact of prenatal counseling by obstetrician–gynecologists is limited. Current literature does not include any individual prenatal breastfeeding interventions offered during obstetrical visits that target low-income African American mothers, and this is the knowledge gap our study specifically addressed, in the setting of a BFHI-designated birthing hospital. We sought to promote EBF and to address identified barriers noted above, including reduced intensity of counseling for African American mothers, absence of personal support for breastfeeding, and negative perceptions of breastfeeding.
The overall aim of this preliminary exploratory study was to evaluate the feasibility and possible effects of two iPad®-based interventions—champion and positive messaging interventions—on prenatal breastfeeding intention and postnatal EBF choice. The specific study objectives were (1) to evaluate the immediate effects of two prenatal breastfeeding interventions on EBF intention, (2) to evaluate the acceptability of the interventions, and (3) to evaluate the rates of in-hospital EBF among women who had received the prenatal breastfeeding interventions.
Materials and Methods
Study design, setting, and participants
This was a longitudinal survey study with follow-up chart review. Expectant women were recruited from on-site, urban women's health clinics located at University Hospitals Cleveland Medical Center (UHCMC) MacDonald Women's Hospital (MWH) in Cleveland, Ohio. Clinics serve expectant women who are primarily low income, publicly insured, and African American; care is provided by certified nurse-midwives, resident physicians, and attending obstetricians.
Expectant women aged 18 years and older, or aged 14–17 years with a consenting guardian present, and who had completed clinically required breastfeeding education (provided at 28–32 weeks of pregnancy) were eligible. UHCMC MWH is a Baby-Friendly-designated birthing hospital, and the required breastfeeding education informs all pregnant women about the benefits and management of breastfeeding as per Step 3. [13] No changes were made to prenatal breastfeeding education during the study period and no additional postpartum interventions were implemented. The UHCMC Institutional Review Board approved the study.
Study procedures
Consecutive eligible women were approached during the periods, May–June 2017 and March–August 2018, by the researchers (R.S.F. and F.R.). Signed informed consent was obtained from all participants. Participants completed a pretest survey, followed by one of the two interventions (champion intervention or positive messaging intervention, as described below and presented in Supplementary Appendix), and a post-test survey. Participants were assigned in nonrandom blocks to receive the champion and positive messaging interventions with the goal of enrolling approximately equal numbers to each group. The researcher was in attendance throughout the 5–10-minute-long session and presented the intervention to the participant. All surveys and interventions were completed by participants on an iPad within REDCap™ (a secure web-based application) before or after a scheduled prenatal visit. 21 At completion, the researcher used the teach-back method with participants to check for understanding of the intervention, and then participants were given a summary document written at a sixth grade reading level that outlined key points of the intervention they received. Participants were given an infant toy and picture book as an expression of thanks for participation.
Interventions
Interventions were empirically selected and (1) supported EBF, (2) could be administered in <10 minutes to minimize clinic flow disruption, and (3) were engaging and low technology. The champion intervention was in use at another Cleveland safety net hospital, and the positive messaging intervention was created by the study team. The champion intervention utilized one module from a free downloadable app (Coffective®) that helps mothers identify a supportive breastfeeding champion. 22 The positive messaging intervention offered breastfeeding information with associated pictures (selected to mirror the racial and ethnic characteristics of the study population) in a question–answer FAQ format.
Data collection
The pretest survey assessed the demographic information, intended infant feeding plan, and previous breastfeeding experience. Demographic factors included age, race, ethnicity, marital and partner status, educational level, and current and intended school and employment plans. Intended infant feeding options were (in the order listed) just formula, both breast milk and formula, just breast milk, or unsure. If breast milk was selected at all, the method of feeding (at breast and/or pumped milk) and planned duration were queried as well. If a mother had breastfed a prior child, she was asked for approximately how long.
The post-test survey followed immediately after the intervention and assessed both intervention completion and participant satisfaction with a 5-point Likert-scaled response to the question, “Was the intervention you received interesting and enjoyable?” To assess any change in feeding intention, participants were asked again about their infant feeding plans using the same phrasing and response choices as in the pretest.
Medical records were reviewed after participant delivery to determine basic information regarding the delivery (including gestational age at delivery and infant birth weight) and in-hospital feeding choice. The medical records of those who delivered at MWH were available for review.
Study outcomes
For aim no. 1, which relates to the immediate effect of the prenatal breastfeeding intervention on EBF intention, we compared the proportion of mothers who intended EBF before and after the interventions. Responses were paired by individual and analyzed by intervention. For aim no. 2, which relates to intervention completion and satisfaction, we first tabulated completion for each participant. We then compared those who said the intervention was very interesting (5 on the Likert scale) with those with all other responses (1–4 on the Likert scale, which included the following: somewhat interesting, neutral, not very interesting, and not interesting at all). Responses were analyzed separately for each intervention. For aim no. 3, which relates to comparison of the mother's original feeding intention with postpartum choice, we assessed the change in the proportions of mothers who originally did and did not intend to exclusively breastfeed before the intervention with proportions of mothers who did and did not exclusively breastfeed after the delivery. Responses were paired by individual and analyzed by intervention.
Statistical analyses
Nominal variables were described using frequencies and percentages. Normally distributed continuous variables were described using means and standard deviations, and non-normally distributed continuous variables were described using medians and interquartile ranges. We compared nominal variables for those who received the differing interventions (champion vs. positive messaging) using chi-squared analyses or Fisher's exact test, as appropriate. Distributionally appropriate two-sample tests were used to compare continuous variables. McNemar's test was used to assess if a statistically significant change in proportions of mothers who chose EBF occurred at two time points (after the intervention and postpartum) for each intervention separately. SAS, v9.4 (SAS Institute, Cary, NC), was used for all analyses. The level of significance was set at 0.05. There were no published data on aim no. 1 with which to calculate a sample size. Therefore, feasibility (researcher availability and funding for participant incentives) drove enrollment for this exploratory study. All eligible women during the study periods were approached.
Results
Population
Of the 265 eligible women approached, 243 (92%) consented to participate. Table 1 presents their demographic descriptors. Of these 243, 132 (54.3%) received the champion intervention and 111 (45.7%) received the positive messaging intervention. Demographic characteristics of all participants are presented in Table 1, and participant flow is shown in Figure 1. There were no statistically significant differences between participants who received the champion intervention versus the positive messaging intervention or between those receiving these interventions who could be followed through delivery at MWH.
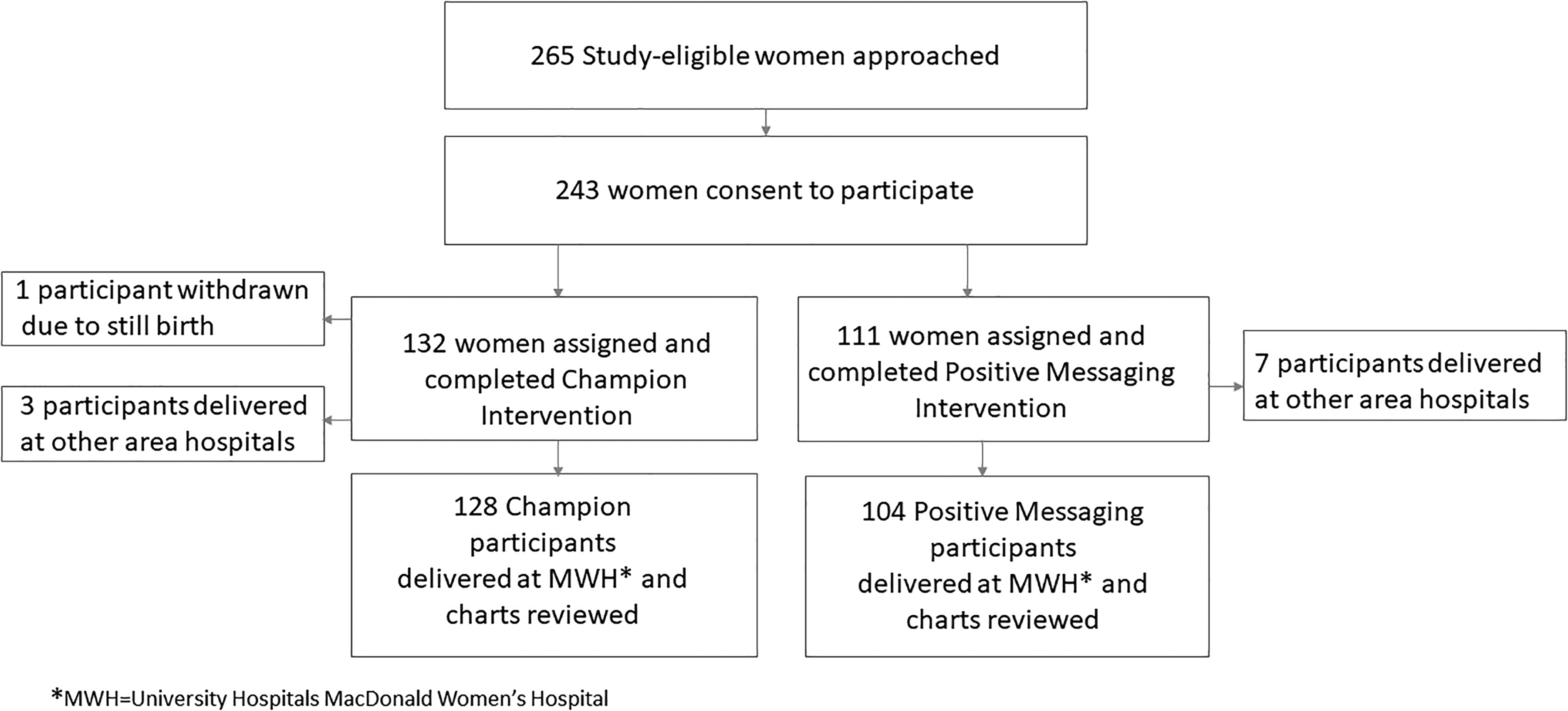
Participant flow diagram.
Description of All Participants and by Intervention Received
Two subjects identified as Hispanic ethnicity (one in each intervention group); 61 (26%) did not respond to the question, so no comparison statistics were run.
p-Value for difference between intervention groups.
One infant whose mother received positive messaging is deceased, all 10 others delivered at outside hospitals.
One infant with ambiguous genitalia.
Two subjects with missing information.
NICU, Neonatal Intensive Care Unit; SD, standard deviation.
Results by aim
For aim no. 1, there was no statistically significant change in intent of EBF immediately before versus immediately after each intervention. For the champion intervention, 45 women (34.1%) intended EBF before the intervention versus 44 women (33.3%) after the intervention. For the positive messaging intervention, 41 women (37.3%, 1 with missing information) intended EBF before the intervention versus 40 women (36.4%, 1 missing) after the intervention.
For aim no. 2, the interventions were well accepted by participants: 100% of the champion and positive messaging intervention participants completed the presented intervention. There was no statistically significant difference in the number of champion intervention participants (83/125, 66.4%) versus positive messaging intervention participants (56/103, 54.4%) who rated the intervention as 5–very interesting, compared with any other ratings on the 5-point Likert Scale (p = 0.08). Only 4 participants (study-wide) rated either intervention as 2–not very interesting or 1–not interesting at all.
For aim no. 3, we found a significant change in the proportion of women who originally did not intend EBF, but then did in-hospital EBF postpartum. This was true both for women who received the champion intervention and for women who received the positive messaging intervention (Table 2). Thirty-two of 40 champion participants (80.03%) intended EBF and did in-hospital EBF; 39/86 champion participants (45.3%) not intending to exclusively breastfeed then did in-hospital EBF (p < 0.0001 for change). Similarly, 30/36 positive messaging participants (83.3%) intended EBF and did in-hospital EBF; 36/67 positive messaging participants (53.7%) not intending to exclusively breastfeed then did in-hospital EBF (p < 0.0001 for change). Based on an exact McNemar's test, we observed a statistically significant difference in the proportion of mothers who chose EBF prenatally (intent) and postpartum (actually in-hospital EBF) for each intervention separately.
Change from Feeding Intention to Feeding Choice by Intervention Group
Two subjects with missing information.
One subject with missing information.
BF, breastfeeding.
Discussion
There are many barriers to EBF for all women, such as latching difficulties, milk supply concerns, the necessity of returning to work, and commercial promotion of formula. Among minority women, rates of in-hospital EBF, even in Baby-Friendly-designated hospitals, are lower than those for other demographic groups.10–12 Since in-hospital EBF is the first goalpost on the journey to EBF through 6 months, addressing related health disparities at this time point is key. We demonstrate here the feasibility and acceptability of delivering a brief, targeted, iPad-based prenatal intervention designed to promote EBF among expectant minority women. We found a statistically significant change in the proportion of minority women who intended (prenatally) and then chose (postpartum) EBF, an exploratory finding that is clinically meaningful and noteworthy because it differs from current literature about breastfeeding intent and practice.
A woman's prenatal intention to breastfeed has been shown to predict her postnatal feeding practices with respect to initiation, exclusivity, and duration of breastfeeding, and contemporaneous data from our own setting agree with the work of others.7–10 Thus, it appears that the interventions we studied had an unexpected and positive impact. In our own and comparison populations demographically similar to ours, urban, publicly insured, predominantly African American women are at high risk for not breastfeeding exclusively in the hospital, even among those who intend to do so and deliver at a Baby-Friendly-designated hospital.10–12 Whether our finding that the iPad-based prenatal interventions had a significant impact on increased in-hospital exclusivity among women not planning on EBF is due to a temporal rather than causal relationship, an unrelated association, or unmeasured variables is not known. However, we can verify that no other changes to in- or out-patient breastfeeding education or hospital breastfeeding policy occurred over the study period, and the interventions as delivered by two different researchers appeared to perform equally well, suggesting the possibility that the interventions themselves drove the study findings.
The significant impact that intention has on EBF duration illustrates the importance of breastfeeding education in the prenatal period. Many studies have investigated the effectiveness of different forms of prenatal interventions. Bonuck et al. evaluated the effectiveness of prenatal visits with lactation consultants and/or electronically prompted guidance from prenatal care providers and found that the interventions increased breastfeeding rates at 3 months postpartum. 23 In another study, Kronborg et al. evaluated the effectiveness of a structured prenatal training program for women mid-pregnancy and found that the intervention group breastfed for a significantly longer period than the control group. 24 These highly successful interventions had meaningful limitations, in that they were time- and labor-intensive and required multiple sessions and the employment of breastfeeding specialists.
This study had several strengths. The interventions used here take only 5–10 minutes to perform and can be administered easily by personnel with limited training. Additional strengths include their cultural inclusiveness and demonstrated feasibility in a population with low health literacy. The interventions are interactive and use iPad technology, which is appealing to a young population and engaging for participants of all ages. The champion intervention uses an app that showcases a very diverse population with embedded pictures. The positive messaging intervention is customizable; the accompanying pictures can be chosen by the users to best represent their target population. Although used here to augment the Baby-Friendly (Step 3), prenatal education requirement, these interventions could be used as stand-alone methods of prenatal breastfeeding education or added to another curriculum. The strength of piloting by piggybacking this intervention on Step 3 educational material (with delivery at a Baby-Friendly-designated birthing hospital) is that it creates a best-case scenario for promotion of EBF in a high-risk population. This approach directly addresses the specific barriers identified in systematic literature review, including reduced intensity of counseling for African American mothers, absence of personal support for breastfeeding, and negative perceptions of breastfeeding. 20
We acknowledge major study limitations in this feasibility pilot. This was not a randomized study; however, the homogeneity of the target population resulted in similarity between the intervention groups without the benefit of randomization. There was no control group and hence the breastfeeding outcomes reported cannot be compared with those of expectant women not receiving the study intervention. Another limitation is the relatively small sample size, and thus the study will need to be replicated in a larger population. The generalizability of our results to nonminority, privately insured, or nonurban populations is uncertain, particularly since the intervention was intended for a high-risk minority population. We had a relatively short follow-up period and do not have data on duration of breastfeeding or exclusivity beyond the hospital stay. We attempted to obtain 2-week follow-up data through medical record review, but due to >50% missing data, an analysis was not performed.
Conclusions
This study demonstrates the promising feasibility of two brief, iPad-based prenatal interventions to promote in-hospital EBF in a predominantly publicly insured, African American urban population delivering at a Baby-Friendly-designated hospital, but at high risk for not breastfeeding. Recent systematic reviews have emphasized the critical importance, and current paucity, of breastfeeding interventions that engage and target minority expectant women, and this study was specifically intended to address this knowledge gap and health disparity. Further research performed as a randomized controlled trial with a sample size based on findings here is needed to replicate these findings and to assess whether the potential benefit identified in hospital is sustained beyond the brief postpartum stay. Additional research could also extend the use of this or similar prenatal interventions to other populations.
Footnotes
Acknowledgments
The authors thank Mitchell Balk, President, Mt. Sinai Health Care Foundation, for funding this project through a Presidential Grant and the staff and patients of the MWH Women's Health Center for their support and participation.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by a Presidential Grant from the Mt. Sinai Health Care Foundation, Cleveland, OH.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.