
Abstract
Abstract
Purpose:
We sought to determine the role of depression and anxiety in breastfeeding cessation.
Materials and Methods:
Participants underwent a baseline visit with a structured clinical interview in the third trimester of pregnancy. Monthly phone interviews assessed current mood symptoms and infant feeding status. We assessed the association between baseline mood and infant feeding outcomes using Cox proportional hazards regression, adjusting for infant feeding intention and sociodemographic confounders.
Results:
We enrolled 222 mother–infant dyads in late pregnancy, of whom 206 completed assessments through 12 months postpartum. We enriched our study with symptomatic women by enrolling 87 women with current depression or anxiety (Current), 64 women with a history of depression or anxiety (Past), and 71 women with no psychiatric history (Never). In multivariable-adjusted analyses, baseline diagnosis was not associated with breastfeeding outcome, but baseline symptoms of depression (Beck Depression Inventory ≥11) or anxiety (Spielberger State Anxiety ≥40) were associated with earlier introduction of formula (depression: adj hazard ratio [HR] 1.52, 95% confidence interval [CI] 1.01–2.30; anxiety: 1.70, 95% CI 1.01–2.87); and any cessation of breastfeeding (depression: adj HR 2.02, 95% CI 1.23–3.31; anxiety: 1.83, 95% CI 1.00–3.33), as were depression symptoms among women who were being treated with antidepressants, compared with untreated asymptomatic women (formula: adj HR 2.27, 95% CI 1.29–4.02; cessation: 2.32, 95% CI 1.17–4.61). History of childhood trauma (adj HR 1.34, 95% CI 1.12–1.61), disordered eating symptoms (adj HR 1.22, 95% CI 1.02–1.46), and poor sleep quality in pregnancy (adj HR 1.32, 95% CI 1.09–1.60) were independently associated with earlier introduction of formula.
Conclusions:
Baseline mood symptoms were independently associated with earlier formula introduction and cessation of breastfeeding. History of childhood trauma, disordered eating symptoms and poor sleep quality were associated with earlier formula introduction. Targeted support may enable women with these symptoms to achieve their feeding goals.
Introduction
In the weeks after childbirth, mother and infant navigate a complex neuroendocrine and behavioral transition. The mother must establish lactation and care for her neonate while coping with the loss of placental hormones, and the infant must learn to feed and elicit maternal care, relying upon the mother to regulate emotional responses to stressful stimuli. 1 Unsuccessful navigation of this transition may manifest as perinatal depression (PND), which affects more than 400,000 mothers in the United States each year. 2 This condition typically presents as a depressive episode, and may include anxiety symptoms during pregnancy or the first 3 months postpartum. 3 Women with PND may also have suicidal ideation and/or fears of hurting the newborn.4,5 In addition, PND is associated with reduced maternal sensitivity, 6 which may adversely affect development of infant emotional regulation and attachment,7–9 even after mothers have received treatment for depressed mood. 10 Insecure attachment, in turn, increases risk of psychiatric disease in the child.6,11 Thus, PND is a common, morbid condition that adversely affects the health of both mother and child.
Recent evidence implicates dysregulation of hypothalamic-pituitary-adrenal axis activity, as well as genetic and epigenetic mechanisms, in the etiology of PND.12,13 In addition, reductions in the neuropeptide oxytocin may contribute to depression, both in the general population 14 and in the perinatal period.15,16 The central role of oxytocin in lactation and the strong association between failed lactation and PND further support this hypothesis. 17
We sought to define the role of oxytocin and stress reactivity in the psychobiology of PND and impaired dyadic development, indexed by maternal sensitivity, infant emotional regulation, and insecure attachment. In this study, we describe the study design, methods, and baseline characteristics of the Mood, Mother, and Infant study cohort, and we report the association between maternal depression and anxiety symptoms and subsequent breastfeeding outcome. We hypothesized that depression and anxiety symptoms in the prenatal period would be associated with reduced duration of exclusive and any breastfeeding.
Materials and Methods
The Mood, Mother, and Infant study
We conducted a longitudinal study of mother–infant dyads from late pregnancy and through 12 months postpartum. To ensure at least 200 dyads for the 12-month visit, we recruited 222 mothers. Participants underwent a structured clinical interview at enrollment, and we enriched our study with symptomatic women by enrolling 87 women with current depression or anxiety (Current), 64 women with a history of depression or anxiety (Past), and 71 women with no psychiatric history (Never).
Recruitment of participants
We recruited women from prenatal and psychiatric clinics affiliated with the University of North Carolina Hospital, as well as through e-mail and social media. Eligible women presenting for prenatal care were approached by research assistants and invited to participate. In addition, fliers, posters, e-mails, and social media posts invited prospective participants to compete an online eligibility questionnaire or contact the study coordinator by phone. A total of 617 women completed the online eligibility questionnaire, and 362 women underwent phone screening. We enrolled about 5 women per month from May, 2013 through April 2017, for a total sample of 222 women.
Eligibility criteria
Inclusion criteria are (1) Singleton pregnancy; (2) intention to breastfeed; (3) intention to remain within 40 miles of UNC through infant's first birthday; and (4) ability to communicate in English. Exclusion criteria are (1) maternal diagnosis of Axis I disorders other than unipolar depression or anxiety disorders. We excluded women with a history of bipolar disorder, given their increased risk of postpartum psychosis. (2) Current substance use (Tobacco, alcohol, and illicits); (3) major congenital anomaly, Neonatal Intensive Care Unit admission >12 hours, and perinatal death; (4) chronic medication/medical condition contraindicated for breastfeeding; and (5) current use of tricyclic antidepressants, which alter cortisol 18 and heart rate variability.19,20
Study assessments
Demographics and medical history
Baseline demographic information was collected at the baseline interview, along with history of pregnancies and outcomes, pregnancy complications, and medications.
Maternal medications and health
Maternal medications were assessed at enrollment and monthly from 1 to 12 months postpartum. Starting at 1 month after birth, participants were asked about contraception use, dose and frequency of other medications, as well as current participation in psychotherapy, use of cigarettes or e-cigarettes, and any hospital admissions for mother or infant.
Infant feeding intention
We measured feeding intention using the Infant Feeding Intentions Scale. 21 This instrument uses Likert-scale questions to quantify the strength of maternal intention to initiate breastfeeding and sustain exclusive breastfeeding through 6 months postpartum. In a validation study, each one point increase in infant feeding intention (IFI) score was associated with 13.7% lower hazards of formula-feeding at 30 days postpartum.
Circumstances of pregnancy
The circumstances of pregnancy scale was developed based on qualitative interviews with 47 women in the United Kingdom regarding pregnancy circumstances. 22 Six domains were identified, including contraceptive use, desire for motherhood, expressed intentions, personal circumstances/timing, partner influences, and preconceptual preparations. Each domain is scored a 0, 1, or 2, with higher scores reflecting stronger pregnancy intention (total score range 0–12).
Maternal psychiatric history
At the baseline visit, subjects underwent a full psychiatric structured interview, including the Structured Clinical Interview (SCID-NP) for DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition). 23 Women were classified as having a current diagnosis of depression if they met criteria for current Major Depression Disorder, Dysthymic Disorder, Depression Disorder NOS, or Postpartum Depression. Women were classified as having a current diagnosis of anxiety if they met criteria for current Panic Disorder, Agoraphobia without history of Panic, Social Phobia, Specific Phobia, Obsessive Compulsive Disorder, Post-Traumatic Stress Disorder, or Generalized Anxiety Disorder. Women who were receiving active treatment for one of these disorders (pharmacotherapy or psychotherapy) were considered to have “Current” depression or anxiety. Women who had a history of any of these disorders but were asymptomatic and not being actively treated were classified as having a “Past” diagnosis. One woman with a history of PND but no symptoms during pregnancy had been prescribed an antidepressant before enrollment to increase her milk supply; as she was not being treated for depression or anxiety, she was classified in the “Past” group. Women with no current or past diagnoses of these disorders were classified in the “Never” group.
Edinburgh Postnatal Depression Scale
We measured maternal mood monthly using the Edinburgh Postpartum Depression Scale (EPDS), a validated assessment of perinatal mood that can be administered by phone. 24 A cutoff score of ≥10 was used to define mild depression, and a cutoff of ≥13 was used to define major depression. 25
Spielberger State/Trait Anxiety Inventory
We quantified anxiety symptoms with the Spielberger State-Trait Anxiety Inventory (Spielberger 1983). The trait inventory provides a stable measure of anxiety, whereas the state inventory captures perceived stress “right now.” We used a cutoff of >40 for state anxiety to define women as symptomatic. 26
Beck Depression Inventory-II
We quantified depressive symptoms with the Beck Depression Inventory-II (BDI-II). 27 We defined mild depression symptoms as BDI-II ≥11. 28
Pittsburgh Sleep Quality Index
We measured sleep quality with the Pittsburgh Sleep Quality Index, 29 which measures the seven domains of sleep quality, latency, duration, habitual efficiency, disturbance, use of sleeping medication, and daytime dysfunction, each on a 0–3 scale. Higher scores reflect worse sleep quality. A global score >5 provides a sensitive and specific measure of poor sleep quality.
Coping Strategies Questionnaire
We assessed maternal pain coping strategies using the Catastrophizing subscale of the Coping Strategies Questionnaire. 30 Higher catastrophizing scores are associated with greater affective pain scores and greater brain activity with a standardized pain stimulus. 31
Eating Disorder Examination Questionnaire 4
The Eating Disorder Examination Questionnaire 32 is a 36-item questionnaire that quantifies symptoms of disordered eating and body image in the prior 4 weeks, resulting in 4 subscales of restraint, eating concern, weight concern, and shape concern, as well as a global scale that is the mean of the four subscales.
Maternal Antenatal Attachment Scale
We quantified maternal feelings toward the fetus using the Maternal Antenatal Attachment Scale. 33 This 19-item instrument quantifies 2 factors: quality of attachment (positive/ambivalent) and intensity of preoccupation with the fetus, indexed by time spent thinking about the fetus (high/low).
Adult attachment style
At baseline, participants completed the Experience in Close Relationships Scale-Short Form, 34 which quantifies adult relationship style across dimensions of anxiety and avoidance.
Experience of being parented
We assessed the participant's experience of being parented before age 16 using the Parental Bonding Instrument, which quantifies dimensions of maternal and paternal care and overprotection. This instrument has shown retest coefficients >0.6 over 20-year follow-up. 35
Childhood Trauma Questionnaire
We used the 28-item instrument Childhood Trauma Questionnaire 36 to assess childhood abuse (physical, emotion, and sexual) and neglect (physical and emotional). For analyses, childhood trauma was dichotomized as “moderate/severe” or “<moderate/severe,” using previously established thresholds for abuse (physical = 10; emotional = 13; and sexual = 8) and neglect (physical = 10; emotional = 15).36,37
Partner conflict
We quantified partner conflict with the Conflict Tactics Scale Form R subscales for verbal aggression and violence. 38 This instrument includes 19 statements regarding different behaviors that partners might engage in an argument, ranging from “Discussed an issue calmly” to “Used a knife or fired a gun.” Items were summed to create three scores for conflict tactics for the respondent and for the spouse or partner: Reasoning, Verbal Aggression, and Violence.
Medical Outcomes Study Social Support Survey
We quantify social support using the Medical Outcomes Study Social (MOSS) Support Survey. 39 The MOSS includes subscales of emotional support, tangible support, positive interaction, and affection, using a 5-point Likert scale (0 = None of the time, 4 = All of the time).
Breastfeeding duration and intensity
We assessed breastfeeding outcome with instruments adapted from the Infant Feeding Practices Survey II (IFPSII). 40 One-week recall of infant feeding, conducted via monthly interview, was used to calculate breastfeeding intensity. 41 Participants reported the number of days per week that they were with their baby, and the number of days they were away from their baby.
For both “with” and “away” days, mothers were then asked to report the number of times per day or per week that the infant was fed at breast, fed expressed milk, fed donor milk, fed formula, or fed solid foods. Total feeds per week was calculated as (at breast + expressed + donor + formula + solid), and intensities were calculated using total feeds in the denominator, including breastfeeding intensity (at breast)/total, breast milk feeding (at breast + expressed + donor)/total, mother's milk feeding (at breast + expressed)/total, and pumped milk feeding (expressed)/total. Each month, women were asked if they had stopped breastfeeding or introduced formula since the last study contact and, if so, the infant's age when this occurred. These data were used to calculate time to introduction of formula and to stopping breastfeeding.
Postnatal follow-up
Beginning at 1 month after birth, we contacted participants monthly via phone interviews to maintain contact and collect information on current feeding, mood, and medications (Supplementary Table S1). At the 1 month interview, participants also reported on details of their birth and early postpartum experience. Phone interviews were scheduled at the participant's convenience and conducted by the study coordinator. Study visits at enrollment and at 2, 6, and 12 months postpartum occurred at the UNC Mother–Infant Biobehavioral Laboratory, during which maternal blood and hair samples and infant saliva samples were collected for hormonal assays (Supplementary Table S2). For details of study visit protocols, see Supplementary Data, Additional Study Instruments and Visit Procedures.
Analysis plan
To characterize our study cohort, we compared baseline measures among women with current, past, or no history of depression or anxiety using chi square tests of analysis of variance, as appropriate. To quantify the association between baseline mood and breastfeeding outcome, we used Cox proportional hazards regression to model the time to first introduction of formula and to cessation of breastfeeding. To select sociodemographic confounders for inclusion in our adjusted models, we modeled the association between infant feeding intention score and outcome, adjusting for sociodemographic confounders. Sociodemographic confounders that were not significant in models for either exclusive or any breastfeeding (type 3 p-value >0.10) were removed from the model by backward elimination. The resulting set of confounders was used for adjusted analyses of associations between baseline mood and breastfeeding outcome.
In an exploratory analysis, we further quantified the extent to which a one standard deviation change in baseline psychometric measures was associated with breastfeeding outcome in unadjusted models and in models adjusted for baseline depression symptoms (BDI <11 versus BDI ≥11), infant feeding intention and sociodemographic confounders. p-Values <0.05 were considered statistically significant. All analyses were performed using SAS 9.4 (Cary, NC).
Ethics, consent, and permissions
The Mood, Mother, and Infant study was approved by the University of North Carolina Institutional Review Board (IRB 12-2016), and each participant provided written informed consent.
Results
In Figure 1, we present a flow diagram of eligible dyads according to STROBE guidelines.
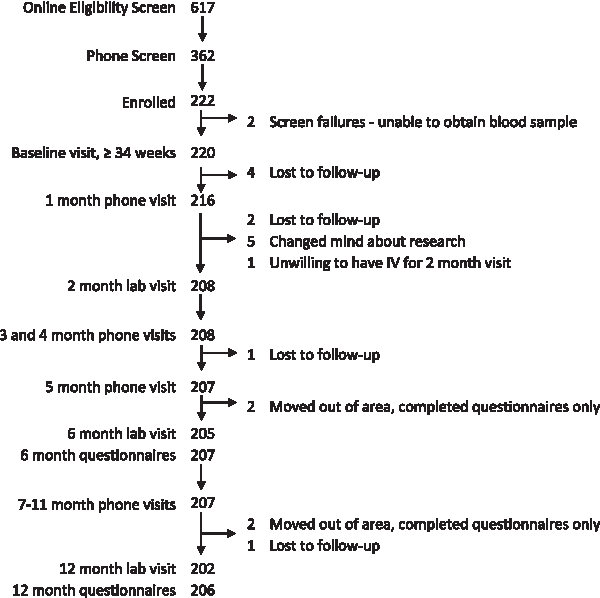
Study participant flow diagram.
Sociodemographic characteristics and baseline psychometric measures of enrolled participants are presented in Tables 1 and 2. Our study sample is predominantly white (73%), married (79.7%), and educated, with 45.5% having completed a postgraduate degree (Table 1). During recruitment, we sought to frequency match our never, past, and current depression/anxiety diagnosis populations by race-ethnicity, parity, and marital status, and as intended, these characteristics were similar among the three groups (Supplementary Table S3). We found no differences by risk level in pregnancy intendedness or breastfeeding intention. As expected, depression symptoms were associated with more adverse scores on baseline psychometric measures (Table 2).
Sample Demographics, n (%) or Mean (Standard Deviation), by Baseline Depression Symptoms, Indexed by Beck Depression Inventory-II ≥11
BDI-II, Beck Depression Inventory-II.
Baseline Psychometric Measures, Mean (Standard Deviation), by Depression Symptoms, Indexed by Beck Depression Inventory-II ≥11
EPDS, Edinburgh Postpartum Depression Scale; MOSS, Medical Outcomes Study Social; STAI, State-Trait Anxiety Inventory.
Overall infant feeding intention in our sample was high; of the 222 women enrolled, 125 (56.3%) had an infant feeding intention score of 16, the maximum measure. We therefore dichotomized infant feeding intention as 16 or <16. Less than maximum IFI score was strongly associated with cessation of both any breastfeeding (unadj hazard ratio [HR] 2.72, 95% confidence interval [CI] 1.74–4.25, adj HR 3.53, 95% CI 1.08–5.99), and introduction of formula (unadj HR 2.23, 95% CI 1.60–3.13, adj HR 2.87, 95% CI 1.97–4.18). Sociodemographic factors that were predictors of infant feeding outcome independent of intention were marital status, race/ethnicity, education, employment in third trimester, income, parity, and insurance type. These covariates were included in multivariable adjusted models.
In proportional hazards models, baseline psychiatric diagnosis by structured clinical interview was not associated with earlier use of formula or cessation of breastfeeding (Table 3); however, both depression and anxiety symptoms were associated (BDI ≥11 adj HR formula introduction 1.52, 95% CI 1.01–2.30; adj HR cessation: 2.02, 95% CI 1.23–3.31; Spielberger State ≥40 adj HR formula introduction 1.70, 95% CI 1.01–2.87; adj HR cessation 1.83, 95% CI 1.00–3.33). When we modeled the association between BDI ≥11 and treatment with psychiatric medication, women with symptoms despite treatment had a higher risk than asymptomatic, untreated women for both formula introduction (adj HR 2.27, 95% CI 1.29–4.02), and breastfeeding cessation (adj HR 2.32, 95% CI 1.17–4.61).
Associations Between Infant Feeding Intention, Baseline Depression, and Anxiety Measures and Duration of Any and Exclusive Breastfeeding, Hazard Ratio, and 95% Confidence Interval
Bold indicates a statistically significant association.
Adjusted or marital status, race/ethnicity, education, employment in third trimester, income, parity, insurance, and infant feeding intention.
CI, confidence interval; HR, hazard ratio.
In an exploratory analysis, we evaluated the association between other psychometric measures and breastfeeding outcomes (Table 4). We found that childhood trauma, eating disorder symptoms, and poor sleep quality were associated with earlier introduction of formula in models adjusting for depression symptoms, feeding intention, and sociodemographic covariates. In adjusted models, none of the psychometric measures evaluated was independently associated with breastfeeding cessation.
Association of Psychometric Measures with Breastfeeding Outcome, Hazard Ratio, and 95% Confidence Interval per Standard Deviation Change
Bold indicates p < 0.05.
Adjusted for depression symptoms at baseline, indexed by BDI ≥11, marital status, race/ethnicity, education, employment in third trimester, income, parity, insurance, and infant feeding intention.
Discussion
Consistent with our hypothesis, we found that depression and anxiety symptoms were associated with earlier introduction of formula and earlier cessation of breastfeeding. Women with persistent depression symptoms while being treated with antidepressants were at the highest risk. In addition, childhood trauma history, eating disorder symptoms, and poor sleep quality were associated with earlier introduction of formula.
Our findings confirm and extend earlier work on the association between depression symptoms during pregnancy and curtailed breastfeeding. While some authors have found that depression symptoms during pregnancy are associated with reduced breastfeeding intention,42,43 others have not. 44 The preponderance of studies has found that women with antenatal depression symptoms have shorter durations of any45–48 and exclusive49,50 breastfeeding, although others have not found an association with continuation through 1 month 51 or 3 months 44 postpartum. Antenatal anxiety has also been linked with reducing breastfeeding intensity and duration. 52 Our findings extend this work by quantifying associations with mood disorder diagnosis, symptoms and treatment, and adjusting for antenatal breastfeeding intention using a validated instrument. 21 We were further able to measure associations of childhood trauma, disordered eating and sleep quality with postnatal feeding outcomes. Although Prentice et al. 53 found that women with a history of sexual abuse were more likely to initiate breastfeeding, most studies have found that women who were maltreated in childhood are less likely to sustain breastfeeding.54–56 Body image dissatisfaction has similarly been associated with reduced breastfeeding intention and duration,57,58 especially among women who are overweight. 59 No prior studies to our knowledge have quantified associations between poor sleep quality during pregnancy and subsequent exclusive breastfeeding; however, in cross-sectional studies, mixed feeding has been associated with worse sleep quality than exclusive breastfeeding.60,61 Our findings suggest that preexisting maternal sleep problems may be a risk factor for mixed feeding, rather than mixed feeding causing sleep disruption.
Strengths of our study include assessment of mood history with a structured clinical interview, comprehensive psychometric measures, and longitudinal follow-up of feeding outcomes through 12 months. However, our findings must be interpreted in the context of the study design. Because assessment of oxytocin during breastfeeding is a central component of the parent study, we enrolled women who intended to breastfeed for at least 2 months. These inclusion criteria may affect generalizability, in that associations between mood and feeding patterns may differ in women without a strong prenatal intention to breastfeed. In addition, our sample is predominantly white, highly educated, and middle to upper-middle class, and thus not subject to structural determinants of health that may impact other populations. Finally, although we enrolled 88 women with a current diagnosis of depression or anxiety, mean symptom scores on the Edinburgh Postnatal Depression Scale, BDI-II, and Spielberger State Anxiety Inventory were below clinical thresholds. We speculate that women with more severe symptoms may be reluctant to engage in an intensive longitudinal study, resulting in a cohort of women with relatively mild symptoms. Associations between well-controlled depression or anxiety and outcomes of interest may differ from those among women with more severe symptoms.
Conclusions
We have successfully recruited and retained a longitudinal cohort of mothers and infants recruited during the third trimester of pregnancy with detailed phenotyping data on mood, relationships, infant feeding, and social supports. We found that maternal symptoms of depression and anxiety during pregnancy were associated with earlier cessation of exclusive and any breastfeeding. We further found that women with a history of childhood trauma, disordered eating symptoms, and poor prenatal sleep quality were at increased risk. Targeted support in these domains may enable more women to meet their breastfeeding goals.
Footnotes
Acknowledgment
The authors are grateful to the families who participated in the Mood, Mother, and Infant study.
Disclosure Statement
A.M.S. and S.M.B. receive grant support from Janssen Research and Development, and S.M.B., receives grant support from Sage Therapeutics, Inc., awarded to the University of North Carolina (Chapel Hill, NC). These grants are outside the submitted work. The other authors have no competing interests.
Funding Information
This research was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01 HD073220-01). The National Institutes of Health had no role in the design of the study and collection, analysis, and interpretation of data and in writing the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.