
Abstract
Abstract
Background:
We aimed to assess the relationship between breastfeeding and myopia in a school-based study in rural China. In addition, we performed a systematic review and meta-analysis to confirm the association from available observational studies.
Materials and Methods:
The school-based study of 2,346 grade 7 students (mean age: 13.8 years) was conducted in southwestern part of China. Myopia was defined as spherical equivalent of less than −0.50 diopter and information regarding breastfeeding was ascertained through a questionnaire. We also performed the literature search in three databases (PubMed, EMBASE, and Cochrane Central Register of Controlled Trials) and reference lists of retrieved studies. Effect estimates were pooled using random-effects models.
Results:
In our school-based study, the association between breastfeeding and myopia was marginally nonsignificant after adjusting for potential confounders, including gender, body mass index, parental myopia, time for reading and writing after school, and time outdoors (odds ratio = 0.75, 95% confidence interval: 0.55–1.04, p = 0.09). In the meta-analysis of eight studies, no significant association was observed.
Conclusion:
Current evidence did not support that breastfeeding could reduce the risk of myopia in children and adolescents.
Introduction
Myopia is a significant global health concern, particularly in East Asians.1–3 The high prevalence of myopia poses a huge socioeconomic burden and high myopia can result in sight-threatening ocular complications such as cataract and glaucoma.4,5 Hence, identifying risk factors is crucial for the prevention of early onset myopia.
Breast milk is an infant's first food and a substantial early life exposure, which is supposed to reduce the risk of myopia.6–8 The long-chain polyunsaturated fatty acids (n-3 LCPUFAs) in breast milk are considered to be an important structural component of photoreceptors and cortical neuronal membranes, which are needed for rapid eye growth and neural development in early life.8,9 In addition, insulin-like growth factor-I (IGF-I) in breast milk promotes normal vascularization of the retina. 10 Low level of IGF-I may cause retinal traction and detachment, resulting in the absence of clear retinal image and eventually leading to myopia. 11 However, results regarding the relationship between breastfeeding and myopia from epidemiologic studies have been conflicting and inconclusive. Some studies found a protective effect of breastfeeding on myopia,6,7 whereas others reported nonsignificant findings.12–14
A comprehensive understanding of the relationship between breastfeeding and myopia may provide novel insights into the effective prevention strategy of myopia at an early stage of life. To address this gap, we first assessed the relationship between breastfeeding and myopia in a school-based study in rural China, where myopia has been reported to be increasingly prevalent in recent years. To make the evidence robust, we also conducted a systematic review and meta-analysis to examine the association of breastfeeding with myopia from available observational studies.
Materials and Methods
Methods of the school-based study
The Mojiang Myopia Progression Study is a school-based study on grade 7 students from 10 secondary schools in Mojiang located in the southwest part of China.15,16 A total of 2,346 (participation rate 93.5%) students including 1,213 (51.7%) boys and 1,133 (48.3%) girls completed the ophthalmic tests and questionnaire. Details of the study have been described in previous publications.16,17 The Mojiang Myopia Progression Study adhered to the tenets of the Declaration of Helsinki for research involving human subjects and was approved by the Institutional Review Board of Kunming Medical University.
Cycloplegic refraction of each eye was measured in all students using an autorefractor (RM-8000; Topcon Corp., Tokyo, Japan). Spherical equivalent (SE) was assessed bases on the standard formula (SE = sphere + [cylinder/2]). Myopia was defined as SE of less than −0.50 diopter (D). Axial length (AL) of the eye was measured with an IOL Master (Carl Zeiss Meditec AG, Jena, Germany). All the ophthalmic tests were performed by professional optometrists or trained technicians. With the help of parent(s), the students filled out the questionnaire to collect information regarding breastfeeding and myopia-related lifestyle factors. After completion of the questionnaires, the research assistants checked the questionnaires to ensure that all questions were properly answered.
We compared the baseline characteristics of the participants who have ever and never been breastfed, using chi-square tests for categorical variables and t-tests for quantitative variables. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to quantify the association between breastfeeding and three myopia-related outcomes, including myopia prevalence, SE, and AL. Owing to the high correlation of SEs (r = 0.90) and ALs (r = 0.98) between two eyes, we only analyzed right eye data in this article. In the first model, we only adjusted for gender. In the second model, we additionally adjusted for gender, body mass index (BMI), parental myopia, time for reading and writing after school, and time spent outdoors. Statistical tests were set with a significance level of 0.05. Statistical Package for Social Science version 20.0 was used for the analyses.
Meta-analysis on the association between breastfeeding and myopia
The meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (Supplementary Table S1). 18 A literature search was conducted to identify original studies assessing the association between breastfeeding and myopia among children and adolescents aged up to 18 years old. PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL) were used to search and identify relevant studies from their inception to March 9, 2019. We employed combined Medical Subject Headings (MeSH) and keyword search strategy based on the mentioned databases and included the following search terms: “myopia,” “refractive errors,” and “ametropia” in combination with “breast feeding,” “infant breastfed,” and “human milk.” Manual search was performed by scanning the bibliographies of relevant findings such as systematic review to ensure that all the potential studies were completed. No contact was made with the authors of original studies for additional information. No attempt was made to retrieve unpublished studies. Disagreements were resolved through consensus.
Selected articles needed to fulfill the following inclusion criteria: (1) infants who had been breastfed were compared with those who had never been breastfed, (2) the outcome was the presence of myopia in children aged 0 to 18 years, and (3) estimates of the association of having been breastfed with myopia were available in the published articles or could be derived. In addition, studies had been published in peer-reviewed journals in English. We excluded studies without a precise definition of myopia, animal studies, and did not fulfill all of these criteria.
Quality of the included studies was assessed using the Agency for Healthcare Research and Quality, 19 a tool developed to assess quality of studies for meta-analyses. It contains 11 items and each study was judged as “yes,” “no,” or “unclear.” Based on the precustomized criteria of inclusion and exclusion, the following information was independently extracted from each article using a purpose-built data collection excel form: study characteristics (last name of the first author, year of publication, and study location); characteristics of targeted individuals (number of participants, participant rates, and age range); and study methodology (definition of breastfeeding and myopia).
To evaluate the effect of breastfeeding on myopia, we calculated the ORs and 95% CIs from reported prevalence rates of myopia in different breastfeeding groups. Following results were revealed by forest plot that represented the effect of breastfeeding on myopia. Heterogeneity among studies was estimated using Cochran's Q test (significance level at p < 0.05) and I2 statistics. If I2 statistic values were <25%, which corresponds to a “low heterogeneity,” then fixed-effects model should be used for data analysis. When I2 statistic values reached up to 50%, then the random-effects model should be selected. Publication bias was appraised by the comparison funnel plot visually and was assessed by the Begg's and Egger's tests. The meta-analysis was performed using the Stata version 12 (Stata Corp, College Station, TX).
Results
Associations between breastfeeding and myopia in the school-based study
Table 1 shows the characteristics of participants who have ever and never been breastfed. Among the 2,346 students in the study, a total of 2,140 participants (91.2%) have ever been breastfed. The comparison of myopia-related variables between the two groups indicated that no statistically significant differences were observed in myopia-related lifestyle risk factors and outcomes (all p > 0.1).
Characteristics of Myopia-Related Variables of Participants Who Have Ever and Never Been Breastfed in the Mojiang Myopia Progression Study
BMI, body mass index; D, diopter; DBP, diastolic blood pressure; SBP, systolic blood pressure.
In gender-adjusted model, breastfeeding was associated with a decreasing prevalence of myopia and the association was of marginal significance (OR = 0.74, 95% CI: 0.54–1.00, p = 0.05) after adjusting for gender. However, the association was nonsignificant (OR = 0.75, 95% CI: 0.55–1.04, p = 0.09) after additionally adjusting for BMI, parental myopia, time for reading and writing after school, and time spent outdoors (Table 2). Similarly, no significant associations were observed between breastfeeding and SE (p = 0.22) or AL (p = 0.82) in the multiple linear regression models.
Associations of Breastfeeding with Three Myopia-Related Outcomes (the Presence of Myopia, Spherical Equivalent, and Axial Length) in the Mojiang Myopia Progression Study
Multivariate adjusted: adjusted for gender, body mass index, time for reading and writing after school, time spent outdoors, and parental myopia.
AL, axial length; CI, confidence interval; D, diopter; OR, odds ratio; SE, spherical equivalent.
Meta-analysis on the association between breastfeeding and myopia
Search results and eligible studies
We identified 22 published articles through three databases and reference lists of relevant studies (nine from PubMed, nine from EMBASE, three from CENTRAL, and one identified through other sources). Nine records were removed for duplicates, and four records were excluded through an initial screening of titles and/or abstracts. The remaining nine full-text articles were assessed, of which four records were further excluded according to our inclusion criterion. Five individual studies (four cross-sectional studies and one birth cohort study), which provided effect estimates on the association between breastfeeding and myopia, were finally considered eligible for inclusion in the meta-analysis6,7,12–14 (Fig. 1). Of the four excluded studies, two studies were reported in language other than English, one failed to report myopia as the outcome, 20 and the other investigated “significant refractive error” (including both myopia and hyperopia) as the outcome. 21 Besides the included five studies, we also included the Mojiang Myopia Progression Study to the meta-analysis. The U.K. birth cohort studies 12 were three independent studies and were treated as different studies in the meta-analysis. Ultimately, eight studies met the criteria for meta-analysis.
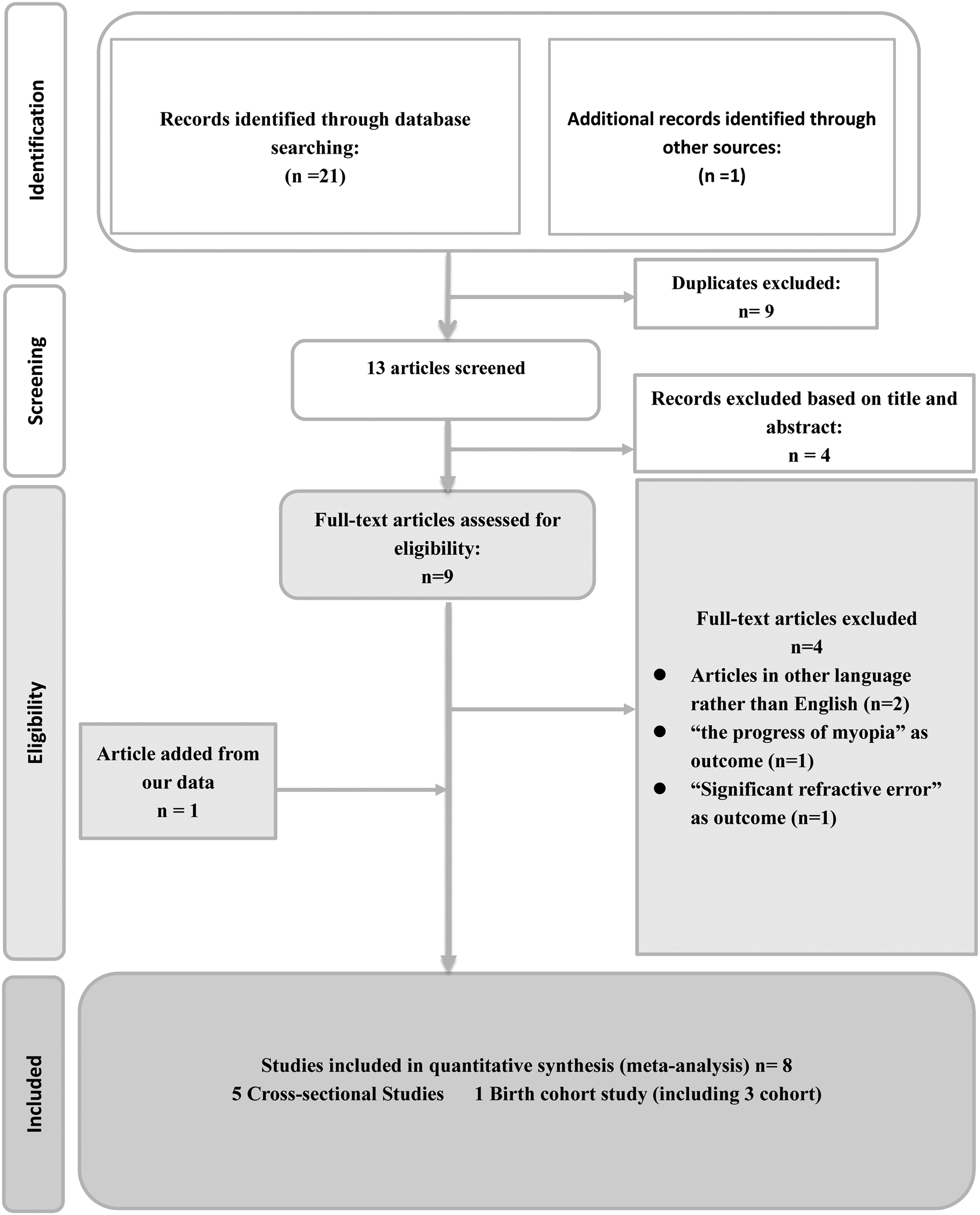
Flow diagram of the selection of eligible studies.
The eight studies in the meta-analysis included 29,849 individuals, among whom 14,182 (47.51%) had ever been breastfed. Supplementary Table S2 summarizes the main characteristics of the included studies. The quality assessment results of the included studies are shown in Supplementary Figure S1. History of breastfeeding in infancy was ascertained by questionnaires in all studies. Prevalence of breastfeeding in these studies ranged from 22.00% to 91.22% (Table 3). Refractive error was assessed objectively using cycloplegic autorefraction in four studies.6,7,14 Myopia was defined as SE of less than −0.5 D in five studies. In the U.K. birth cohort studies, myopia was defined as an unaided vision of 6/12 or worse. Prevalence of myopia in these studies ranged from 4.26% to 65.37% (Table 3).
Random-Effects Meta-Analysis Investigating the Effect of Breastfeeding on Prevalence of Myopia
1970 BCS, British Cohort Study; CI, confidence interval; 1958 NCDS, National Child Development Study; 1946 NSHD, Medical Research Council National Survey of Health and Development; OR, odds ratio.
Table 3 provides the pooled estimates of the association between breastfeeding and myopia. Random-effects meta-analysis yielded a pooled OR showing no association between breastfeeding and myopia (OR: 0.93, 95% CI: 0.78–1.10, I2 = 60.8%, pheterogeneity = 0.01). Only one study explored the association between durations of breastfeeding and the risk of myopia and found that the association was nonsignificant. 7 Although there were some signs of asymmetry in the funnel plot, the Egger's (p = 0.27) and Begg's (p = 0.19) tests showed no publication bias (Supplementary Fig. S2). Sensitivity analyses showed that all single-study-omitted estimates were within the 95% CIs of their respective overall pooled estimate (Supplementary Fig. S3).
Discussion
The Mojiang Myopia Progression Study together with the meta-analysis of eight studies did not observe significant association between breastfeeding and myopia. Thus, current evidence did not support that breastfeeding could reduce the risk of myopia in children and adolescents.
The results of the Mojiang Myopia Progression Study showed no significant relationship between breastfeeding and myopia, which were inconsistent with the findings of previous studies on Chinese populations.6,7 Such discrepancy may be explained by differences in LCPUFAs exposure, especially docosahexaenoic acid (DHA). In the last trimester of pregnancy, DHA accumulates rapidly in neural cortex tissues 22 and retinal membrane synapses. 23 Exposure to different concentrations of DHA during pregnancy may have different influence on fetal eye development.24,25 Besides, breast milk is a major source of DHA for infants, and DHA concentrations differ substantially relying on maternal diet.26,27 Previous studies have demonstrated regional differences in distribution of DHA across China.28,29
The meta-analysis also indicated that breastfeeding is unrelated to the risk of myopia. The heterogeneity in this meta-analysis may be explained, in part, by the differences in sample sizes, study regions, levels of social-economic status, and definitions of breastfeeding and myopia. In addition, several cases should be noted. First, most included studies in this analysis were performed in East Asia, which features a high prevalence of myopia. Lack of data from Western countries may result in the absence of associations between breastfeeding and myopia in developed countries. Second, overall findings were based on observational epidemiologic studies, and they may lack sufficient power to determine any relationship. Third, breastfeeding data were based only on maternal recall, which may lead to recall bias. But, recall bias might hardly cause effect on the validity of data in the studies included in our work, as parents were unaware of the hypothesis and breastfeeding questions were mixed with unrelated queries.
In conclusion, current evidence did not support that breastfeeding could reduce the risk of myopia and this issue warrants further clarifications.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.