
Abstract
Objective:
To compare (1) differences in mother's own milk (MOM) provision and enteral feeding outcomes, (2) differences in preterm formula and donor human milk (DHM) uses as bridges to exclusive MOM feedings at discharge, and (3) MOM and enteral feeding outcomes for racial/ethnic subgroups before and after the implementation of a hospital DHM feeding program.
Methods:
Retrospective data from 313 very low birth weight (VLBW; birth weight <1,500 g) infants born between January 2011 to December 2012 (pre-DHM, n = 157) and April 2013 to March 2015 (DHM, n = 156) were analyzed.
Results:
For this predominantly low-income and minority VLBW infant cohort, the percent of enteral fed hospitalization days was higher in the DHM group (pre-DHM 94% [88, 97] versus DHM 98% [95, 99], p < 0.001). Although MOM remained the predominant first enteral feeding type, significantly fewer DHM infants received MOM (pre-DHM 89% versus DHM 75%, p = 0.001). During days of life 1–14, a lower percentage of DHM infants received 100% MOM (pre-DHM 68% versus DHM 55%, p = 0.02). For the entire cohort, the risk for MOM discontinuation was significantly associated with maternal young age, multiparity, non-Hispanic Black race/ethnicity, and low income. Implementation of a DHM program did not predict duration of MOM feedings. However, non-Hispanic White infants had a longer duration of MOM feedings with DHM availability.
Conclusions:
Our findings highlight the importance of using precise dose and exposure period methodology to determine the impact of DHM on MOM provision. In addition, DHM availability may be associated with varying effects on MOM provision among racial/ethnic groups.
Introduction
When mother's own milk (MOM) is not available, pasteurized donor human milk (DHM) rather than preterm formula (PTF) is recommended for hospitalized very low birth weight (VLBW; birth weight <1,500 g), extremely premature (EP; ≤32 weeks of gestation) infants.1,2 DHM is not meant to replace MOM feedings in this vulnerable population, but rather to serve as a supplement when mothers are unable to provide an adequate volume of MOM. The distinction between supplementing and replacing is important because DHM is nutritionally inferior to MOM and does not confer comparable protection from complications of prematurity.3–5 Although DHM reduces necrotizing enterocolitis, it does not consistently reduce late-onset sepsis, bronchopulmonary dysplasia, or neurodevelopmental problems.2,3,6 Thus, understanding whether the availability of DHM reduces the provision of MOM (MOM provision) for VLBW EP infants in the neonatal intensive care unit (NICU), especially during critical postbirth exposure periods when MOM feedings have been linked with the reduction in specific morbidities, is crucial.7–9 Of equal importance and as yet unexamined is whether maternal race/ethnicity affects MOM provision after DHM introduction.
The majority of studies in this area have been retrospective comparisons of lactation outcomes for pre- and post-DHM introduction, and the most commonly used outcome variable has been breastfeeding rates at NICU discharge.5,10 Using these criteria, a systematic review addressing the impact of DHM availability on MOM provision revealed an increase in any but not exclusive breastfeeding rates at NICU discharge. 5 Although breastfeeding rates at NICU discharge are easily accessed and measured, they are not specific to whether DHM replaces MOM, and have been associated with multiple other modifiable and nonmodifiable variables such as maternal age, race/ethnicity, education, income, achievement of coming to volume, pumping behaviors, and duration of the NICU hospitalization. 11 Similarly, only two studies have reported results for different racial/ethnic groups as a part of subject characteristics.10,12 In one study, investigators reported a 10% increase in “any human milk” at NICU discharge after the introduction of DHM in California NICUs; however, the differential effects of DHM availability on racial/ethnic groups were not reported. 10
The purpose of this study was threefold. First, we sought to compare the differences in MOM provision and enteral feeding outcomes before and after the implementation of a DHM feeding program during critical periods in the NICU hospitalization when the infant is susceptible to morbidities, using precise feed volumes of MOM and DHM. Second, we compared the differences in the use of PTF and DHM as a bridge to the achievement of exclusive MOM feedings at NICU discharge. Third, we compared these MOM and enteral feeding outcomes for different racial/ethnic groups for the two time periods.
Methods
Design
This retrospective comparison study leveraged datasets from two cohorts of infants, each corresponding to pre- and post-DHM availability. The pre-DHM availability (pre-DHM) dataset was extracted from a National Institutes of Health-funded prospective cohort study of MOM and health outcomes during a time that PTF was the only alternative to MOM feedings (January 2011 to December 2012). 7 After the completion of that study, DHM became routinely available for VLBW EP infants in the study NICU (April 2013). The post-DHM availability (DHM) dataset consisted of retrospective data from medical records of VLBW infants admitted to the same NICU during the 2 years after the introduction of DHM (April 2013 to March 2015). Both datasets contained detailed information about the type (e.g., MOM, PTF, and DHM) and daily volumes (mL) of all enteral feedings received during the NICU hospitalization. From the datasets, we calculated dose (amount) and exposure period (specific periods postbirth) for MOM, PTF, and DHM feedings as described in previous studies by this research team.7–9 Maternal and infant characteristics that may have influenced MOM provision were extracted from these datasets.
Sample
Inclusion criteria for both pre-DHM and DHM cohorts were identical: infant gestational age ≤32 weeks, birth weight <1,500 g, enteral feeding initiation before day of life (DOL) 14, and survival to at least DOL 14. Only one infant from a set of multiples was selected randomly for inclusion. Subjects were excluded if maternal race/ethnicity was described as “other” and if maternal insurance type was missing. Figure 1 provides the final sample for the pre-DHM and DHM groups. The Rush University Medical Center institutional review board approved this study.

Sample schematic. DHM, donor human milk; DOL, day of life; NICU, neonatal intensive care unit; VLBW, very low birth weight.
Setting
The study was conducted in a level III regional perinatal NICU that serves a predominantly minority, low-income population with nearly all VLBW EP infants receiving at least some MOM feedings. For both pre-DHM and DHM groups, all women received standard lactation care by NICU breastfeeding peer counselors, who are former NICU parents and represent the racial/ethnic composition of VLBW infants and their families. 13 Women initiated MOM provision with hospital-grade electric breast pumps and were able to rent a subsidized hospital-grade pumps for in-home use. In April 2013, DHM feedings were introduced for VLBW EP infants when MOM was not available. Women received both verbal and written information about MOM and DHM before providing written consent for DHM feedings. Infants of consenting mothers received DHM to supplement MOM as needed through to 34 weeks postmenstrual age, at which time they were transitioned to PTF. If a mother refused DHM and MOM was not available, the infant received PTF. There were no other changes in NICU enteral feeding or lactation practices during the study period.
Dependent measures
MOM provision
Multiple indicators of MOM provision were used, including rates of ever receiving MOM, PTF, and DHM; dose and exposure period of MOM feedings; the percentage of NICU days for any and exclusive MOM feedings; percentage of infants receiving exclusive human milk (EHM = MOM + DHM); percentage of NICU days for EHM feedings; and rates of MOM feeding at NICU discharge. NICU discharge-related variables were calculated using data from the entire 24-hour period preceding discharge. For all analyses, MOM provision was measured by the infant's receipt of MOM as documented in the medical record; maternal pumping data were not collected.
Rates of ever receiving MOM, PTF, and DHM were calculated for each infant using a categorical yes or no variable. Then, the frequency of infants receiving MOM, PTF, and DHM was calculated and expressed as a percentage for each group.
As performed in previous studies7–9 demonstrating the association between MOM and reductions in the risk of neonatal morbidities, the dose of MOM (MOM dose) was calculated as a percentage of total enteral feedings by summing the total volume (mL) of MOM received over a specific exposure period, dividing this sum by the volume of total enteral intake received during that same exposure period, then multiplying by 100 ({[mL MOM] ÷ [mL MOM + mL DHM + mL formula]} × 100). The exposure periods compared were DOL 1–14, DOL 15–28, and the entire NICU hospitalization. The percentage of each cohort receiving exclusive (100% MOM dose) during the NICU hospitalization was calculated. The duration of maternal lactation was defined as the last DOL that the infant received any MOM during infant hospitalization because pumping data were not available.
The percentages of NICU days for any and exclusive MOM feedings were calculated using only the NICU days during which the infant received enteral feedings (enteral feeding days [EFD]). Any MOM EFD was calculated by dividing the number of days that any MOM was received by the number of EFD  . The calculation for exclusive MOM EFD was similar
. The calculation for exclusive MOM EFD was similar  .
.
Enteral feeding initiation
The DOL of the first enteral feeding (DOL first feed) was extracted for each infant and the median value was calculated for each group. DOL first feed was then categorized dichotomously as either ≤DOL 3 or ≥DOL 4. The type of first enteral feeding (MOM, DHM, and PTF) was extracted and expressed as a percentage for each group. First enteral feeding type was also dichotomized as MOM or other (PTF and/or DHM).
Use of PTF and DHM
Variables included in this analysis were any PTF or DHM during DOL 1–28, use of PTF and DHM as a bridge to exclusive MOM at NICU discharge, PTF-ever, the first day of PTF feeding, DHM-ever, EHM during NICU hospitalization, and EHM enteral fed days. PTF and DHM as a bridge was calculated by first identifying infants who received exclusive MOM at NICU discharge and subsequently determining whether these infants also received either PTF or DHM during DOL 1–28. This variable was expressed as a percentage of the total number of infants who received exclusive MOM at NICU discharge. EHM days included only days that either exclusive MOM (pre-DHM group) or a combination of MOM and/or DHM (DHM group) and no PTF were received. The percentage of EHM days during NICU hospitalization was calculated as follows:  .
.
Maternal and infant characteristics
Maternal characteristics that may have influenced MOM provision included the following: maternal age; parity; race/ethnicity (non-Hispanic Black [NHB]; Hispanic [H]; and non-Hispanic White [NHW]); income status, defined as low income if receiving public insurance; and mode of delivery. Infant characteristics that may have influenced MOM provision, timing, and type of enteral feedings included gestational age (completed weeks), birth weight (g), length of hospitalization (days), sex, and multiple gestation.
Statistical analysis
Descriptive analysis revealed both normally and non-normally distributed data. Descriptive statistics included mean ± standard deviation, median [first and third quartile; Q1, Q3], and n (%). Continuous data were analyzed with t-test and Mann–Whitney U test for normal and non-normal distribution, respectively. Categorical data were analyzed using chi-square test and Fisher exact test, as appropriate.
Regression analysis was conducted to evaluate the interaction with race/ethnicity and DHM group on feeding outcomes. Logistic regression was used to test for the main effects and interaction of DHM availability and maternal race/ethnicity on feeding measures. Given the non-normal distributions for the continuous variables, the following variables were categorized into two mutually exclusive categories. The MOM dose was categorized (yes-no) as to whether the infant received ≥50% MOM feedings during the specific exposure period. MOM EFDs were categorized (yes-no) as to whether the infant received ≥50% EFDs of MOM and EHM during hospitalization.
Models of Cox proportional hazard were constructed using the entire dataset to analyze the risk of discontinuation of MOM before discharge (the last DOL the infant received any MOM) adjusting for maternal (age, parity, race/ethnicity, insurance, and delivery mode) and infant (age, sex, length of hospitalization, and first feed type) factors.12,14–16 Data were analyzed using SPSS for Windows Version 24 (SPSS, 2013, Armonk, NY). All statistical tests were two-tailed with p < 0.05 considered statistically significant.
Results
Of 356 VLBW infants admitted to the NICU during the study period, a total of 313 infants (pre-DHM = 157; DHM = 156) met inclusion criteria and were included in this analysis (Fig. 1). Maternal and infant characteristics for the two groups are detailed in Table 1. EFD were higher in the DHM group (pre-DHM 94% [88, 97] versus DHM 98% [95, 99], p < 0.001), but other between-group characteristics were similar.
Maternal and Infant Characteristics
Bold indicates significant p-value.
Data are give as mean ± SD, median [Q1, Q3] or frequency (%).
DHM, donor human milk; EFD, enteral feeding days; SD, standard deviation.
Table 2 shows that 97% of infants in both groups received MOM feedings, but the timing and type of initial enteral feedings differed. A greater percentage of DHM infants than pre-DHM infants received initial feedings by DOL 3 (pre-DHM 55% versus DHM 72%; p = 0.003). Although MOM remained the predominant first enteral feeding type, significantly fewer DHM infants received MOM for the first feeding (pre-DHM 89% versus DHM 75%; p = 0.001). Furthermore, during DOL 1–14 fewer infants in the DHM group received exclusive or 100% MOM (pre-DHM 68% versus DHM 55%; p = 0.02).
Enteral Feedings
Bold indicates significant p-value.
EHM = MOM + DHM.
Data are given as mean ± SD, median [Q1, Q3] or frequency (%).
MOM versus DHM + PTF.
DHM, donor human milk; DOL, day of life; EFD, enteral feeding days; EHM, exclusive human milk; MOM, mother's own milk; NICU, neonatal intensive care unit; PTF, preterm formula; SD, standard deviation.
The use of PTF and DHM as supplements to MOM differed significantly for the groups, as given in Table 2 and Figure 2. In the pre-DHM group, a greater proportion of infants received PTF-ever (pre-DHM 82% versus DHM 69%, p = 0.008). PTF was introduced significantly earlier after birth (19 versus 44 days, respectively, p < 0.001) in the pre-DHM group. Similarly, EHM feedings for the entire hospitalization were less prevalent in the pre-DHM group (18% versus 32%, respectively, p = 0.008). Neither the percentages of infants receiving supplements to MOM in DOL 1–28 nor the use of supplements as a bridge to exclusive MOM at NICU discharge were different between the groups. Tests for interactions between pre-DHM and DHM groups by maternal race/ethnicity on feeding outcomes were not significant (Table 3).
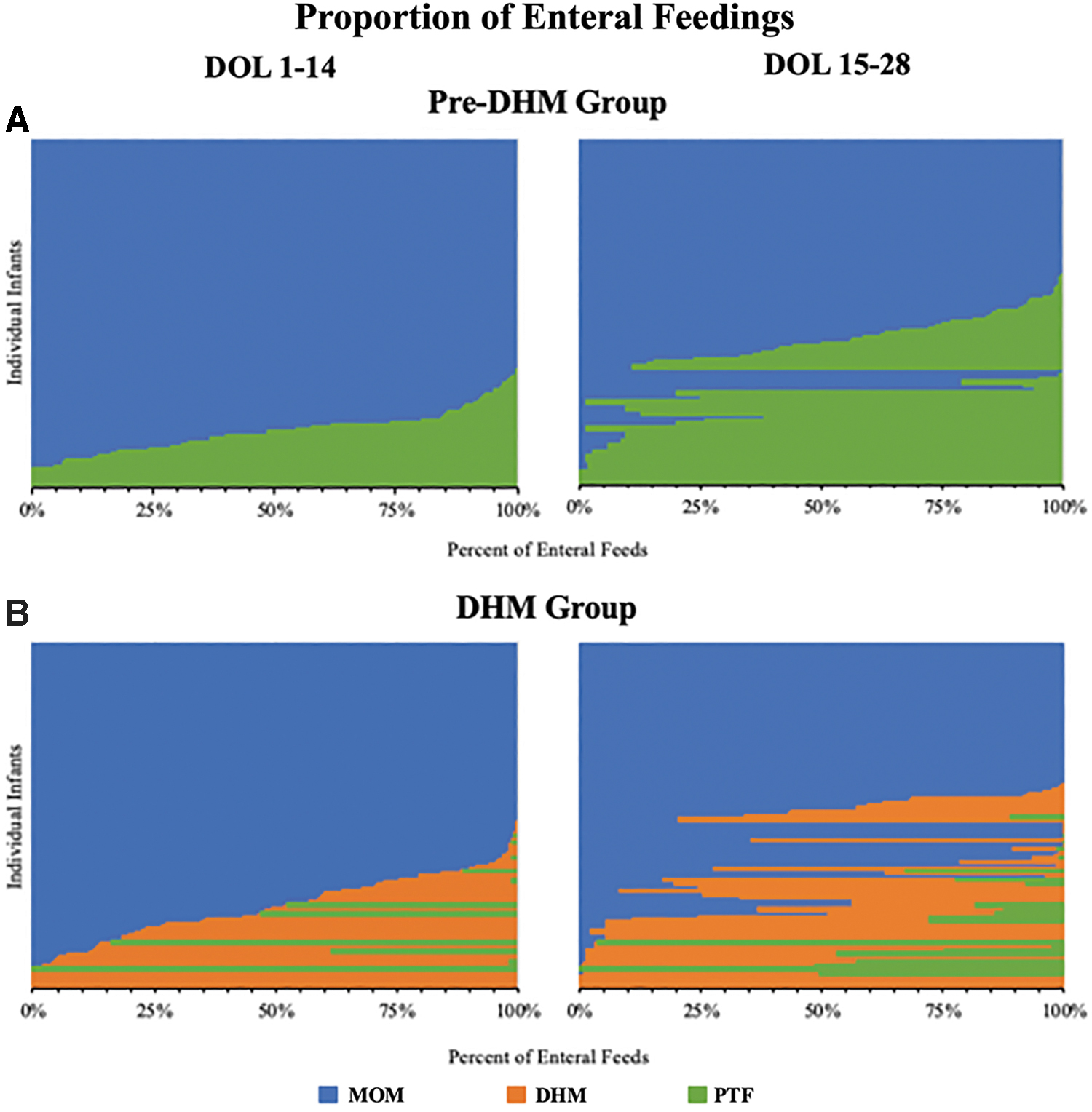
Proportion of enteral feeding types during DOL 1–14 and DOL 15–28 by cohort. Each horizontal bar denotes an infant's proportion of enteral feeding by exposure period.
Selected Enteral Feedings by Maternal Race/Ethnicity
EHM = MOM + DHM.
DHM, donor human milk; DOL, day of life; EFD, enteral feeding days; MOM, mother's own milk; NICU, neonatal intensive care unit; PTF, preterm formula.
A Cox proportional hazard model revealed no differences between pre-DHM and DHM groups (hazard ratio = 0.77 [0.55, 1.07], p = 0.12) for the time until discontinuation of MOM feedings after controlling for covariates (Table 4). The hazard of MOM discontinuation overall was significantly higher with younger maternal age, multiparity, NHB race/ethnicity, and low income. The hazard of MOM discontinuation was lower when the first enteral feeding type consisted of MOM. In a subsequent model we added a term for the interaction between DHM availability and race/ethnicity. Although the interaction was not statistically significant (p = 0.148), there was a pattern for NHW infants to have longer duration of any MOM feedings after the introduction of DHM (pre-DHM median 37 [Q1, Q3, 22.5, 68.8] versus DHM 68.5 [41.0, 103.8] DOL), whereas NHB (37 [19.0, 62.0] versus 35.5 [22.0, 53.3] DOL) and Hispanic (55.0 [40.0, 83.0] versus 39.0 [23.0, 74.0] DOL) infants had no change in MOM duration (Fig. 3).
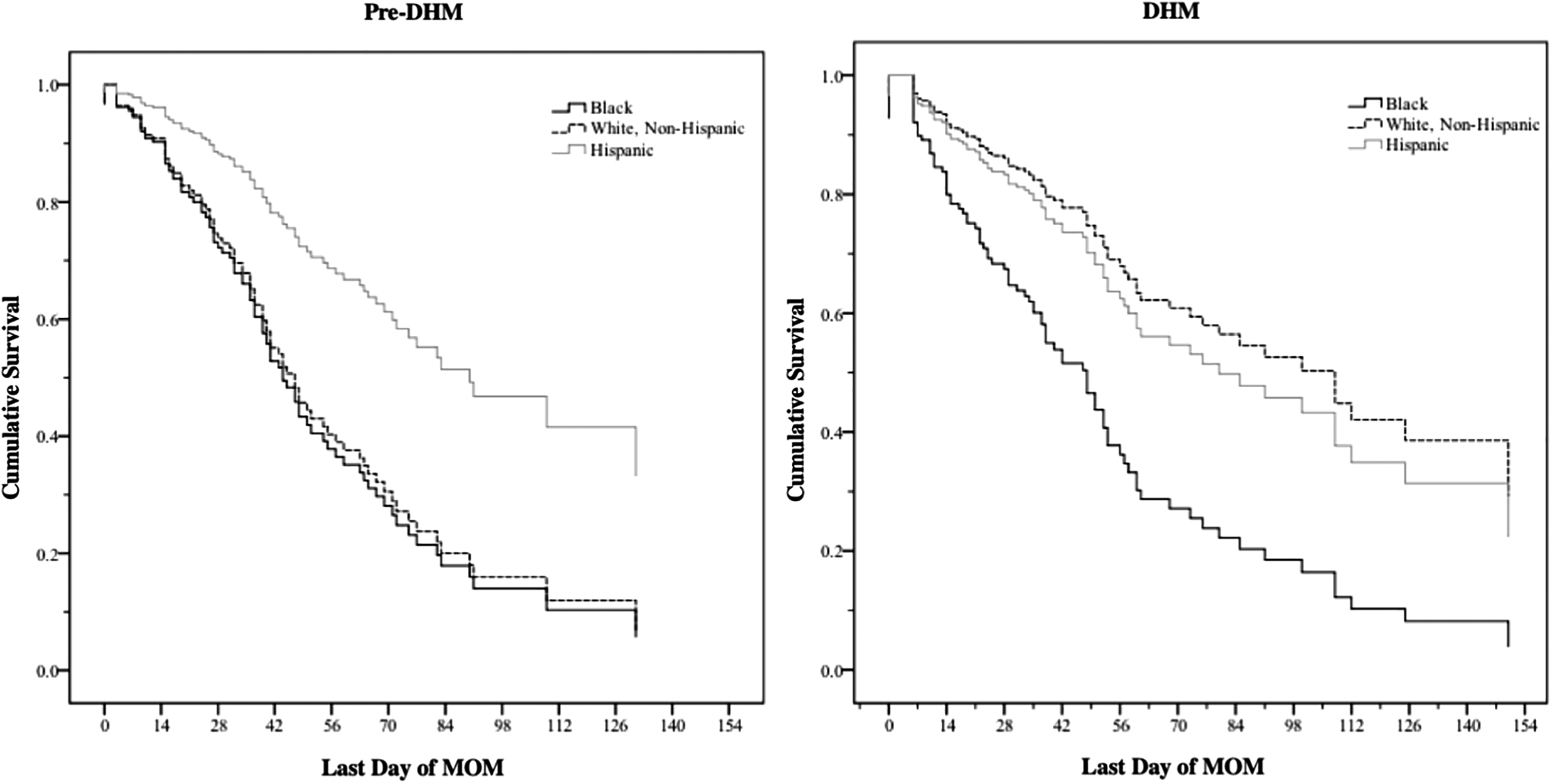
Adjusted cumulative survival of MOM feedings for infants in pre-DHM and DHM groups by maternal race/ethnicity. DHM, donor human milk; MOM, mother's own milk.
Hazard Ratio for Discontinuation of Mother Own Milk Feedings
Bold indicates significant p-value.
CI, confidence interval; DHM, donor human milk; HR, hazard ratio; LL, lower limits; MOM, mother's own milk; UP, upper limits.
Discussion
In this retrospective study from a single NICU serving a predominantly low-income and minority population, the maternal and infant characteristics and initiation rates for MOM feedings were similar between pre- and post-DHM cohorts. Our results reveal that the introduction of DHM was associated with a reduction in receipt of exclusive MOM feedings during DOL 1–14, but was not associated with a decrease in MOM provision over the first month or the NICU hospitalization. Compared with the pre-DHM group, the DHM group demonstrated earlier initiation of enteral feedings, later introduction of PTF, less use of any PTF, and more exclusive HM feeding days during the NICU hospitalization. Although feeding group did not predict the duration of MOM provision for the groups as a whole, infants of NHW and Hispanic mothers had a longer duration of MOM feedings compared with infants of NHB mothers. Other covariates that predicted a shortened duration of MOM provision included not receiving MOM as the first enteral feeding, younger maternal age, primiparity, and low income.
A potential concern is that some women may have equated DHM with MOM despite clear, written messaging highlighting the superiority of MOM over DHM and the availability of intensive NICU lactation support. Given the similar rates of MOM provision after the first 2 weeks, this is less likely to have occurred in our study. The lack of effect between DHM availability and the duration of MOM provision in our study is consistent with that of others, except for Parker et al., 17 who reported higher rates of MOM provision at NICU discharge after the implementation of a DHM program. Our use of precise dose and exposure period methodology adds to the extant literature by providing essential, specific detail about the timing and the extent to which DHM replaced both MOM and PTF throughout the NICU hospitalization. We speculate that the overall lack of effect of DHM on MOM provision in our study may be related to our already high rates of MOM provision. Although fewer of the DHM than pre-DHM infants received exclusive MOM during the first 14 days of life, this appears to be related to the earlier introduction of enteral feedings with DHM rather than waiting for MOM. Parker et al. 18 used a similar methodology to examine the change in MOM provision in EP infants over three consecutive periods: pre-DHM, first year after DHM availability, and second year after DHM availability. Although Parker et al. 18 found that less MOM was consumed during the first 28 DOL after DHM availability, they did not report extensive feeding outcomes. In contrast, Parker et al. 17 reported higher rates of any MOM at DOL 7 after the introduction of DM and attributed this to messaging by the nursing staff about the importance of MOM.
The availability of DHM resulted in many differences in enteral feeding outcomes, including earlier enteral feeding initiation and a decreased rate of MOM as the first enteral feeding for the DHM group. Butler et al., 19 Marinelli et al., 20 and Tshamala et al. 21 also reported earlier initiation of enteral feedings with DHM availability. Our work and others suggest that the earlier introduction of enteral feeds reflects the consensus that DHM is safer to feed early postbirth than is PTF. 3 Because prolonged nil per os status impedes intestinal epithelial cell growth and colonization of the intestine and contributes to gut dysbiosis, DHM serves as a safe strategy for earlier enteral feed initiation when MOM is unavailable. 3
Our findings that the DHM group had a lower rate of PTF-ever, a higher rate of EHM throughout the NICU hospitalization, and a higher percentage of EHM enteral fed days when compared with the pre-DHM group suggest that DHM may have replaced PTF as a supplement to MOM. Although Delfosse et al. 22 were the first investigators to describe the use of DHM as a bridge to the initiation of MOM feedings, their study did not compare pre-DHM and DHM cohorts nor did it measure feeding outcome at the time of discharge. In contrast, we defined bridge to mean any feedings other than MOM during the early postbirth period in infants who were receiving exclusive MOM at NICU discharge. This approach accounted for the fact that many mothers experience delayed secretory activation and their infants need a temporary supplement, or bridge, to exclusive MOM feedings. 23 Although we found no difference between the groups concerning the use of supplements as a bridge, we found the type of supplement was different.
We found no significant interactions between DHM group and maternal race/ethnicity. However, a closer look at these data suggest a concerning pattern that may be clinically relevant. Particularly noteworthy are the favorable differences in feeding outcomes that are statistically different for the DHM cohort as a whole (Table 2), but may not be equitably shared by NHB infants (Table 3). Specifically, these favorable patterns include the reduced use of PTF-ever and, concomitantly, higher rates of EHM during NICU hospitalization (e.g., avoidance of PTF) in NHW and Hispanic infants (44% of the total sample) but not NHB infants in the DHM cohort. Figure 3 suggests that DHM availability coincided with the longer duration of MOM provision only in NHW mothers, or 22% of the total cohort. As our center is located in an urban setting, generalizability may be limited in less racially/ethnically diverse NICUs. Research in other settings such as rural, affluent, low-income, and predominantly NHW populations may provide additional valuable information about the effect of DHM availability on MOM provision and other feeding outcomes. These patterns underscore the importance of including subgroup analyses in quality improvement initiatives to target clinical interventions appropriately.
Our study has several strengths and limitations. First, the large size for this single-site study includes a racially/ethnically diverse sample representative of hospitalized VLBW infants. The precision of the MOM dose and exposure period data pinpoints the effect of DHM availability at different time points from initial enteral feedings through to NICU discharge for subgroups of infants based on maternal race/ethnicity. Limitations of our study include the retrospective design and the single NICU setting with a high MOM initiation rate that may limit generalizability. In addition, similar to previous researchers, we used infant receipt of MOM as a proxy for maternal pumped milk volume.10,17,18,20–22,24–29
DHM availability was associated with reduced early MOM dose feedings but not with a change in the overall rate or exclusivity of MOM feedings at discharge in an NICU. Our findings highlight the importance of using precise dose and exposure period methodology to determine the impact of DHM on MOM provision and the importance of reporting outcomes for maternal race/ethnicity subgroups.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was partially supported by NIH R01 NR010009.