
Abstract
Ankyloglossia is a failure of the tongue to release from the oral floor with reported consequences that include breastfeeding difficulties and speech impediments. Frenotomy is a commonly performed procedure for the treatment of ankyloglossia. Laser (light amplification by stimulated emission of radiation) is one of several mediums used to perform frenotomies. Although most frenotomies are uncomplicated, there remains a small possibility of complication, such as infection, pain, ductal injury, and hemorrhage, even in expert hands. Because frenotomies are most often performed in infants, postoperative hemorrhage is an important complication to look for as even small amount of bleed may prove fatal, due to low blood volume reserve. We report a case of delayed hemorrhage after laser frenotomy in a 6-week old infant displaying shock symptoms and required fluid resuscitation.
Introduction
Ankyloglossia is characterized as limited movement of the tongue due to congenital failure to release from the floor of the mouth.1,2 Ankyloglossia is commonly categorized as anterior and posterior; the classification depending on the location of a fibrous cord anterior or posterior to ventral tongue mucosa, respectively. 1 The consequences of ankyloglossia can include breastfeeding difficulties and speech impediments; although many patients with ankyloglossia may be asymptomatic and may not require intervention.1,3
Release of the tongue by frenotomy, otherwise termed frenectomy, is the preferred management option if surgery is indicated. 3 However, the timing or even the need for surgery is controversial. With the exponential increase in diagnosis in recent decades, with one reported increase of 834%, 1 it is paramount to weigh the clinical benefits and the risks of frenotomy.
Three categories of surgical approaches are utilized to achieve appropriate tongue release: cold steel, electrocautery, and laser (light amplification by stimulated emission of radiation). 4 Cold steel, usually scissors, is used to snip the frenulum, and hemostasis is achieved most often by simple pressure, silver nitrate, or gauze. 1 Sutures are rarely indicated. Electrocautery pen can be used to perform frenotomy in a similar manner. Laser is a novel technique that uses carbon dioxide, diode, yttrium aluminum garnet (YAG), or neodymium-doped-YAG that allows precision and immediate cauterization. 5
Although most frenotomies are uncomplicated, there are several case reports of complications. Some reported complications include infection, pain, salivary duct injury, and bleeding most typically in the immediate postoperative period.1,6 Herein, we report a case of a severe hemorrhage in an infant 7 days after an uncomplicated laser frenotomy requiring volume resuscitation.
Case
A 6-week-old healthy male weighing 4,710 g presented to an experienced community dentist with concerns of shallow latch, moderate but improving pain with breastfeeding, fussiness and spit-ups after feeds, and open mouth rest posture. The patient's mother was concerned that the baby's poor latch was contributing to swallowed air leading to increased reflux, and felt that the baby had a similar presentation to his older sibling, who had previously undergone release of his oral tethered tissue. On physical examination, the baby was observed to have a Kotlow class 2 moderate posterior tongue tie, with thick frenulum inserting at the anterior third of the tongue (Fig. 1A). The tongue was noted to be bowl shaped with minimal elevation on sucking. He also was diagnosed with a Kotlow 2 lip tie.
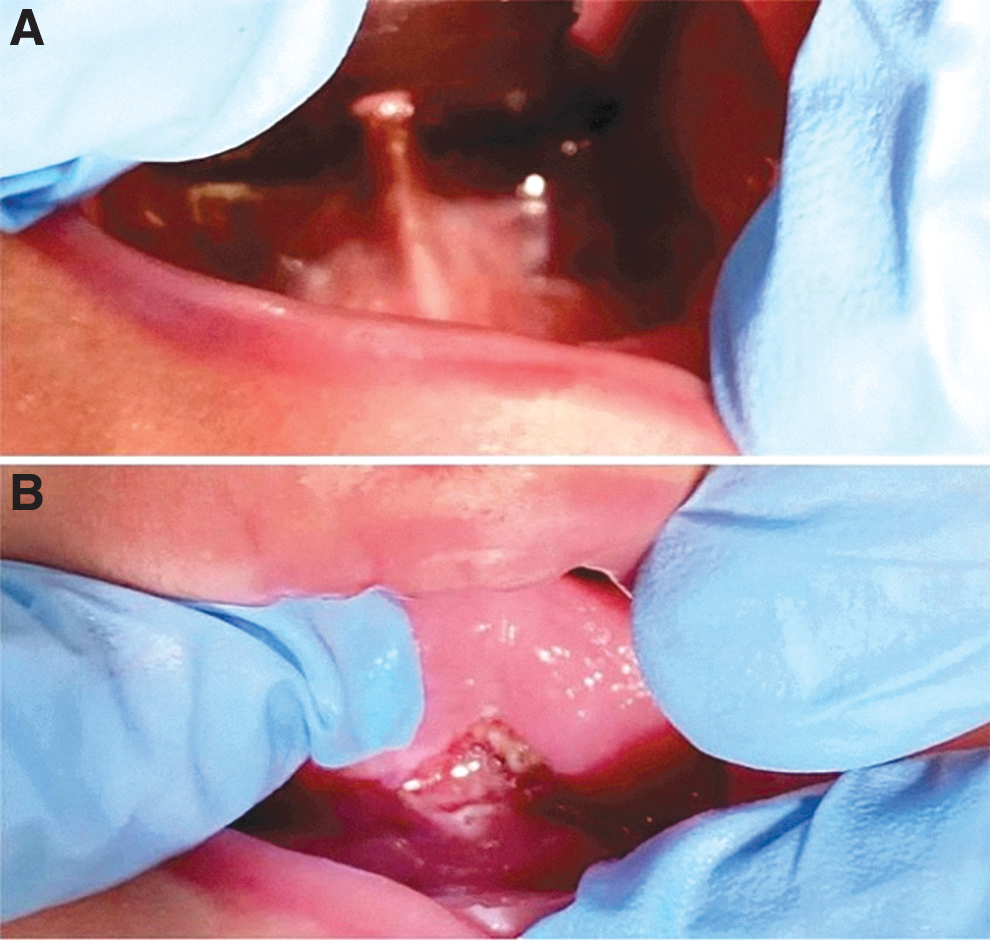
In
The attending dentist recommended release of both lip and tongue tie. A PicassoLite 810 nm diode laser was used with the following settings: 1.6 W, continuous wave, and 1 minute per site. No anesthesia was administered. The tongue tie was released until a diamond-shaped wound with no palpable tethering was achieved (Fig. 1B). Care was taken to avoid lingual artery, vein, and nerve as well as sublingual caruncle, duct, and gland. The procedure was uncomplicated perioperatively. Immediately postoperatively, the patient was encouraged to breastfeed, and mother noticed improvement in comfort, with more tongue elevation and organized suck observed by the dentistry team. The patient's mother was counseled to perform regular postoperative stretching exercises (stretching and active wound management protocol: lifting the tongue and elevating the upper lip six times daily for 3 to 4 weeks postoperatively, beginning the day of the procedure) and feed ad lib, as per the usual postoperative protocol for all frenotomies performed by this attending dentist. The patient was encouraged to continue to work with a lactation consultant in addition to performing these exercises, and follow-up at 1 week postoperatively.
On postoperative day (POD) 2, the mother noticed blood tinged sputum without active bleeding. On POD 5, the mother noted blood stains on patient's bed and shirt with blood clots in the mouth. The patient was immediately brought to the emergency department.
At admission, the patient was alert, responsive but agitated. The blood pressure at admission was 50/35 and the heart rate was 217. Other vital signs were within normal range. The patient appeared pale. His initial hemoglobin was 117 g/L, with a normal white blood cell count and a normal hematocrit. International normalized ratio and partial thromboplastin time were both within normal limits. Venous blood gas initially showed low pH of 7.2 with a critically elevated lactate at 7.2 mmoL/L.
The blood pressure below 5th percentile for age, marked tachycardia, pallor, and critically high lactate levels indicated hypovolemic shock. The emergency staff estimated ∼50mL of blood loss and decided to initiate crystalloid fluid resuscitation. Subsequently, the pH normalized to 7.36 and lactate improved to 1.8.
A 2.5 cm blood clot was found in the inferior aspect of the tongue with no active bleeding. Suctioning of the clot revealed a 1.5 cm raw surgical site extending from the lingual frenulum to the left floor of the mouth, which was the presumed site of bleeding (Fig. 2). There was no damage to Wharton's duct.
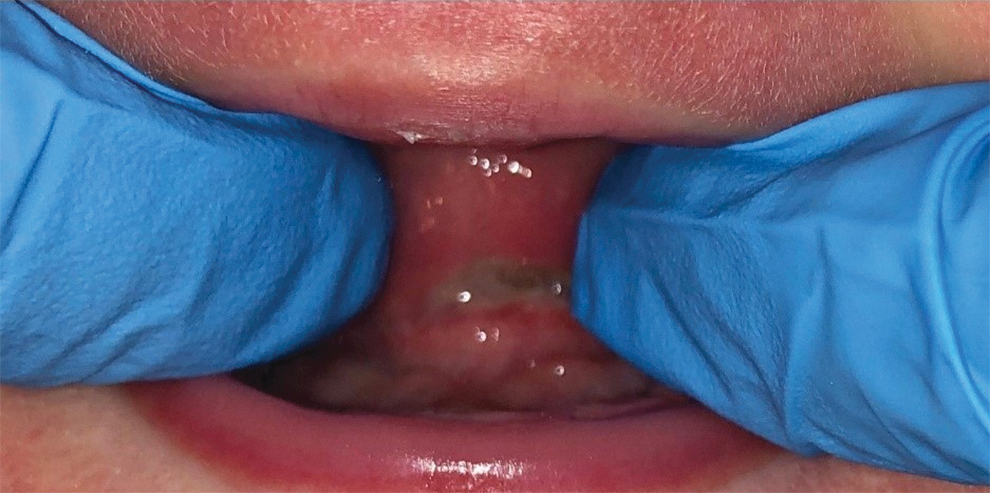
At POD 6, a 1.5 cm surgical site is shown extending from the lingual frenulum to the left floor of the mouth. POD, postoperative day.
The site was cauterized with silver nitrate and the patient was admitted for 24 hours of monitoring. Clindamycin PO for 5 days was initiated prophylactically in case infection had contributed to the postoperative bleed. No further interventions were required, and the patient had no further bleeding. On subsequent follow-up with the attending dentist at POD 8, the surgical site appeared within normal limits with formation of granulation tissue. At POD 14, the patient had complete healing of his surgical site and there had been no further bleeding

At POD 14, the surgical site is completely healed with no further bleeding.
Discussion
Laser frenotomy is a relatively novel treatment for ankyloglossia. 5 Compared with conventional scalpel surgeries, laser is advertised to be more precise and less traumatic. 7 Some of the reported reasons for using laser in oral surgeries are heat-induced hemostasis, reduced anesthetic use, enhanced precision, eliminated need for sutures, and faster recovery time. 8 There is a paucity of complications reported of the laser frenotomy in the literature, limited to cases of delayed healing, and inadvertent laser heat-induced thermal necrosis. 9 There are also reported risks of thermal injury related to the use of laser, including damage to surrounding tissue. Immediately beneath the ventral tongue fascia lie lingual nerve branches that provide sensory and motor functions to the frenulum, and the anterior tongue. As such, the dissipating heat of the laser can inadvertently injure this integral structure. 2 Other theoretical damages associated with laser are eye damages such as aqueous flare, cataract formation or retinal damage, plume formation by laser vapor, and inherent fire hazard. 5 To our knowledge, however, this is the first reported case of hemorrhage after laser frenotomy.
This case is also unique in that bleeding was delayed in nature. There is only one similar case currently in the literature. Tracy et al. report a case of delayed bleeding after cold steel anterior frenotomy in a 4-year-old male, despite intraoperative hemostasis. 10 An arterial bleed was noted at POD 10 in this patient, with tachycardia and hemoglobin dropped to 78g/L and cauterization was required for control.
Our report of delayed hemorrhage postfrenotomy follows similar time course as secondary (or delayed) post-tonsillectomy hemorrhage, and we postulate the mechanism of bleeding may be similar. After tonsillectomy, a fibrin clot coats the tonsillar fossa and separates at around POD 7. 11 This leaves a thin new stroma and exposes the vascular bed, thus increasing the risk for hemorrhage. This seems a likely mechanism for the bleeding observed in our patient, given the wound appearance and the time course. Other common reasons for secondary hemorrhage after tonsillectomy are infection, non-steroidal anti-inflammatory use, undiagnosed bleeding disorder, and solid food trauma, none of which were suspected in this patient. 12 His postoperative exercises may have been contributory, although these are routinely offered to patients after many frenotomies, without reports of bleeding. He was treated prophylactically for infection, and he did not have overt signs and symptoms suggestive of infection.
Frenotomies are performed mainly in the pediatric population, especially very young neonates with difficulty breastfeeding. Newborns have limited blood volume reserve and develop shock symptoms rapidly. 13 As such, minimal bleeding can prove catastrophic. Pediatric hemorrhage is classified into four severities of increasing percentage of estimated blood volume (EBV) loss. 14 The total EBV in pediatric patients is estimated to be 75–80 mL/kg, which in our patient of 4.710 kg would be ∼375 mL.13,15 The estimated 50 mL of blood loss would represent ∼15% of blood loss and indicates Class 2 hemorrhage with compensation by the aforementioned early shock signs and symptoms. In children, especially infants, even compensated shock may progress rapidly into uncompensated shock within minutes if not treated promptly, resulting in severe hypotension and cardiac arrest. 15 In our case, hypotension and critically high lactate were grave signs that necessitated immediate fluid resuscitation and close monitoring.
Conclusion
Frenotomies are typically presented as a benign procedure without risk of complication; however, ours and other cases suggest that patients should be counseled about the real, although rare, risk of serious complication. The authors suggest careful patient selection to limit unnecessary risk, and advocate that frenotomies should be performed by experienced providers if they are deemed necessary. A shared decision-making approach should always be employed before surgical management of ankyloglossia.
Footnotes
Authors' Contributions
All authors have contributed to the interpretation of the clinical findings, literature search, drafting, and revising of the article. All authors have approved the final article and agree to the conditions outlined on the authorship agreement form.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.