
Abstract
Background:
Research on how storage and transport of expressed human milk in a tropical country affect the milk bacterial count is limited.
Materials and Methods:
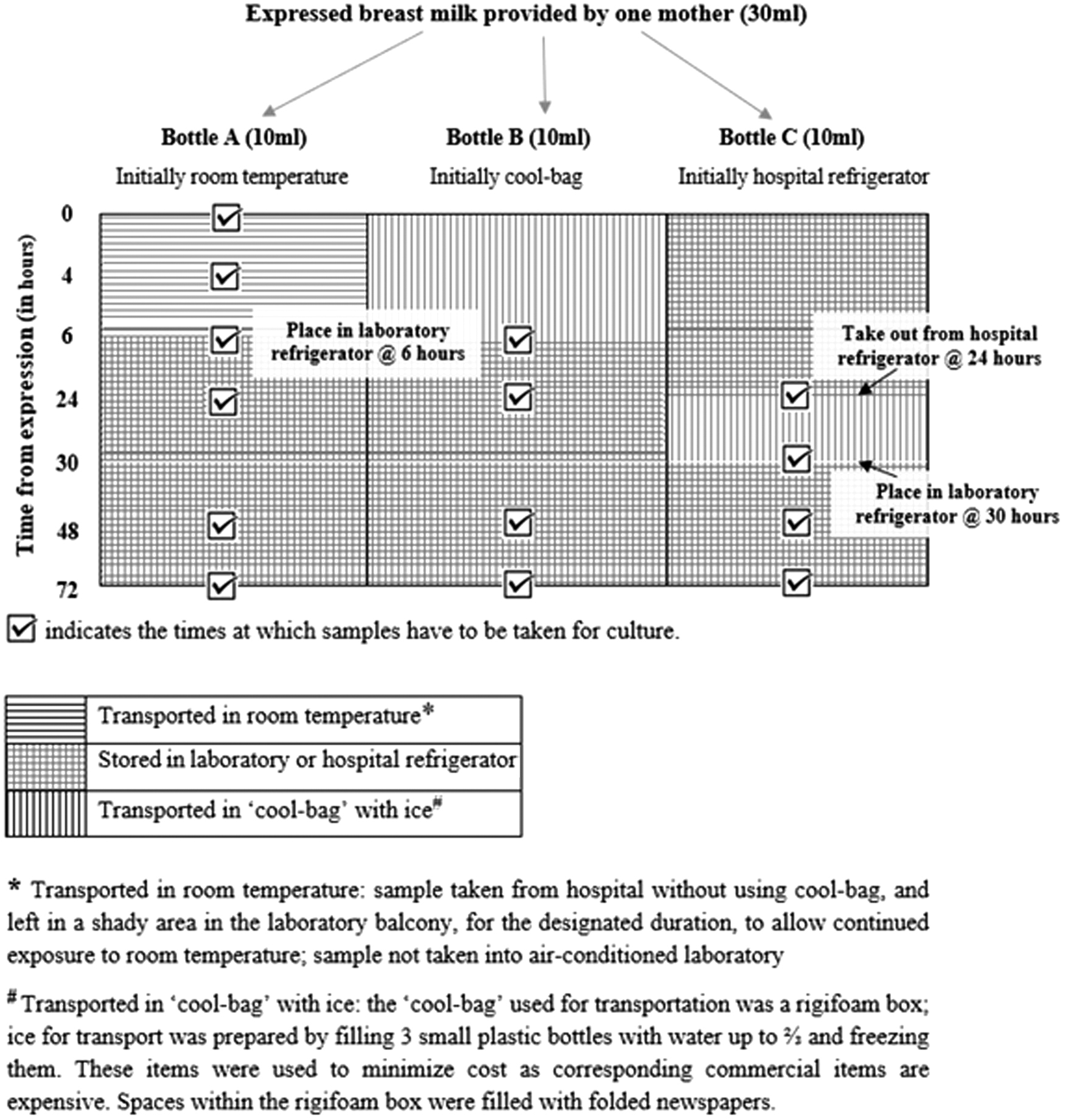
A cross-sectional descriptive study of 50 mothers of infants in a Sri Lankan tertiary neonatal unit was performed. Expressed mother's milk was divided into three bottles and kept under varied environmental conditions to simulate different storage and transport methods. Initial bacterial culture of milk was performed <30 minutes after expression, with further cultures at predetermined times. Bottles A and B were stored at room temperature and in a cool bag for the first 6 hours, respectively, and then refrigerated; and bottle C was refrigerated for 24 hours, transported in a cool bag for 6 hours, and rerefrigerated until 72 hours. Total colony counts >105 colony-forming units (CFU)/mL of viable microorganisms or >104 CFU/mL of either Enterobacteriaceae or Staphylococcus aureus were considered positive.
Results:
Initial culture was positive in 30% (15/50) of samples; majority, 87% (13/15), of these were S. aureus. For bottle A, 26% (13/50), 36% (18/50), 34% (17/50), and 26% (13/50) of samples were positive at 4, 6, 24, and 72 hours, respectively. For bottle B, positive cultures were found in 26% (13/50) and 17% (8/47) of samples at 24 and 72 hours, respectively. For bottle C, results were similar to bottle B.
Conclusions:
Transportation of expressed mother's milk for 6 hours in a tropical climate using a low-cost cool bag, with refrigeration at other times, maintained acceptable bacterial counts for up to 72 hours after expression. Hygienic practices at collection are extremely important as most samples with significant bacterial growth were positive on initial culture.
Introduction
Mothers' milk feeding, either as direct breastfeeding or expressed milk, is the best method of providing nutrition to a newborn infant as it has numerous advantages for both the infant and mother. 1 Some infants born prematurely or those who are sick need to spend several weeks in a neonatal unit. In most western countries such as the United States, United Kingdom, and Australia, once a mother is discharged from the hospital after the birth of her infant, she has to bring her expressed milk from home or other accommodation outside the hospital as facilities for families to stay in the hospital 24/7 are not common.2,3 Our study in Melbourne, Australia, showed the importance of using cooler containers for transporting refrigerated mother's milk even for a short duration from the home to the hospital and the need for diligent monitoring of milk storage and transport conditions to ensure that milk remains at a low temperature. 4
In contrast, the current practice in most Sri Lankan neonatal units (based on corresponding author's personal experience as a pediatric/neonatal doctor in Sri Lankan hospitals for 15 years) is for mothers to spend the entire time that their newborn infants are in the neonatal unit as inpatients themselves at the same hospital, but in a different ward or room from the infant. One reason mothers need (or are usually expected) to remain in the hospital is to provide the infant with fresh expressed milk for every feed. Storage and transport of expressed mother's milk are not standard care in Sri Lanka. In Sri Lankan public hospitals, most mothers express their milk by hand into sterilized metal cups.
Study context
This article describes bacterial growth in human milk samples stored and transported under different conditions in Sri Lanka, an island situated within the tropics where the mean annual temperature varies between 27°C in coastal lowlands and 16°C in central highlands. 5 Ragama, where this study was conducted, is situated in the coastal lowlands. The average temperature is 30–32°C, with a maximum of 38.4°C recorded in the past 40 years. 6
Bacteriological safety of expressed mother's milk
A 2019 review analyzing 242 studies from 38 countries identified the presence of a total of 820 species in human milk microbiota, with Staphylococcus aureus and Streptococcus agalactiae being the most common bacteria. 7 Minimizing the possibility of expressed human milk containing pathogenic bacteria is extremely important for neonatal units. A hazard analysis approach to handling expressed human milk in a neonatal unit in Belgium identified critical control points that can be optimized to ensure infant safety: hand hygiene, cleaning/disinfection of breast pump equipment, need to refrigerate or freeze the expressed milk within 1 hour, transportation in an isothermal bag to the hospital, maintenance of the home refrigerator or freezer, and steps for ensuring correct identification of a milk sample to be given to a particular infant. 8
Previous literature on this topic was searched with the aim of identifying studies that looked at bacterial growth in mother's milk, expressed under a range of conditions and stored under different temperatures for varied periods, to determine the safety (using cutoff values for bacterial counts) of feeding the milk to hospitalized infants. Studies or study components that looked at the bacteriology of donor milk in milk banks or those where storage of the expressed milk was only in a freezer were not included. All original articles similar to ours, which were identified by searching PubMed using the terms “expressed breast milk,” “expressed human milk,” “storage time,” and “bacteria,” are included in Table 1. Relevant original articles cited by those identified on the PubMed search and mentioned as being similar when accessing these identified articles were also included (last update September 10, 2020).
Safe Storage Duration/Microbiology of Expressed Mother's Milk Based on Storage Temperature
CFU, colony-forming units; NM, not mentioned; SC, significant contamination.
In addition to the previous search terms on PubMed, the terms of “hygienic practices,” “home vs. hospital,” and “manual vs. pump” were used to identify articles that have assessed the effects of different places and techniques of expression and hygienic practices on bacterial counts of milk. These articles are summarized in Table 2. Studies on storage or transport of human milk have not been conducted in Sri Lanka previously.
Effects of Hygienic Practices, Place, and Method of Expressing Mother's Milk on Suitability for Administration to Hospitalized Newborn Infants
CFU, colony-forming units; NM, not mentioned.
Recommendations from human milk banks and their relevance
Human milk banks across the globe have set standards on acceptable limits of bacterial content in expressed human milk that is donated for infants of other mothers, for example, the Human Milk Banking Association of North America, PREM Bank (Perron Rotary Express Milk Bank) in Perth, Australia, and Mercy Hospital Breastmilk Bank, in Melbourne, Australia.30–33 There are guidelines published by the National Institute for Health and Care Excellence (NICE), United Kingdom too. 34 Guidelines prepared for temperate climates have limited applicability in tropical countries such as Sri Lanka.
Furthermore, there are no standards for what is considered an acceptable level of bacterial content when a particular infant is fed freshly expressed human milk from its own mother. Even in developed countries, when a mother is providing expressed milk for her own infant in a neonatal unit, the milk is not tested microbiologically before administration. We therefore decided to use values that were most lenient, as given by NICE, United Kingdom, as the cutoffs for this study: that is, a count of >105 colony-forming units (CFU)/mL for total viable microorganisms or >104 CFU/mL for Enterobacteriaceae or S. aureus as a significant growth, which constituted a positive sample. 34
Study rationale
Fresh human milk for each feed is the optimal nutrition that can be provided to infants in a neonatal unit. 35 However, if social and other circumstances make it necessary for a mother to be at home and bring in milk expressed at home for her newborn in the hospital, it is important to understand the best way that this can be done.
Therefore, the objective of this study was to explore the bacterial content in expressed human milk transported and stored using different methods, under Sri Lankan environmental conditions, and to identify which methods and duration measures would maintain bacterial count levels within acceptable limits over 72 hours from the time of expression.
Materials and Methods
Design
A descriptive exploratory study was conducted at the University Neonatal Unit of Colombo North Teaching Hospital, Ragama, Sri Lanka, and the Faculty of Medicine, University of Kelaniya, Ragama. As it would be unethical to change current practice and send mothers home before the infant's discharge from hospital for the sake of a study, simulated conditions were used.
Eligibility
Women whose infants were currently receiving care as inpatients at the above neonatal unit, who had already been trained in standard hygienic practices for human milk expression, and who were able to express 30 mL of milk within 30 minutes were included in the study. Those women whose milk supply was inadequate to provide 30 mL of expressed human milk without compromising the amount available for her infant were excluded. Women taking antibiotics within the previous 48 hours were also excluded along with women who had nipple damage or nipple/breast infection or a skin condition.
Sample size and recruitment
The number of mothers who provided expressed human milk samples for similar previous studies ranged from 12 to 63 individuals.11,12,14,18,19 A bacteriology study of human milk expressed at home and hospital showed that a significant number of pathogenic organisms were identified by 4 hours when milk was kept at 25°C in 11% of those samples expressed at home. Therefore, using the calculation N = 4 × Zα 2 × p (1 − p)/w 2 (Zα = confidence level, w = width of confidence interval, and p = prestudy estimate of the proportion to be measured), the sample size required to show the percentage of milk samples that were positive as a reflection of what it would be in a similar larger population, with a confidence level of 95% and confidence interval of ±10%, was 37. 36 We planned to recruit 50 mothers to allow for issues such as laboratory staffing and equipment malfunction. Each mother's expressed milk was bacteriologically tested 14 times under 3 storage/transport protocols. A research assistant not involved in clinical care recruited the participants. Consecutive convenience sampling was used. 37
Flow of samples and microbiological testing
Mothers expressed their milk in the neonatal unit, simulating home conditions, and the microbiological testing was done at the Department of Microbiology, Faculty of Medicine, University of Kelaniya (located within 10 minutes walking distance from the hospital). The 30 mL of milk provided by each participant was divided equally into 3 bottles, A, B and C, which were each placed inside a Ziploc bag along with a data logger thermometer. The bottles remained in this bag for 72 hours of monitoring, commencing from completion of milk expression, except when samples were being obtained for culture. The protocols for the three scenarios were prepared to simulate expressed milk brought in to the hospital within 6 hours (A and B) or the following day after being stored at home for 24 hours (C) and used in the unit until 72 hours from time of expression (Fig. 1). Immediate transport of required bottles ensured that initial culture was done within 30 minutes.
Sample flowchart.
Simulation of home conditions
Mothers followed standard advice already provided regarding hand hygiene and breast preparation for milk expression. The containers used for collection and storage of expressed milk were glass feeding bottles sterilized in the neonatal unit using boiling water on a stove. The staff kitchen refrigerator was used for storage before transportation (for bottle C) rather than the well-controlled medicine/vaccine refrigerator of the neonatal unit. In the laboratory, milk was stored in their sample refrigerator, which simulated a potential future milk refrigerator in the neonatal unit. When placing samples in the refrigerator, the door compartment was avoided.
Microbiological testing
Samples were inoculated onto sheep blood agar and MacConkey agar plates with a standard 1 μL wire loop at specified intervals. The plates were read for growth of microorganisms after overnight incubation at 37°C in the incubator. The total aerobic bacterial colony count (total viable organisms) and the colony counts for each of the organisms in a particular sample were calculated manually by counting the CFU and interpreted as CFU/mL. Identification of organisms was done by the colony morphology, gram stain, and routine biochemical tests such as the catalase test, staphylase test, coagulase test, oxidase test, streptococcal grouping by agglutination test, indole test, and inoculation into KIA (Kligler iron agar).
Details of data collection tools
Demographic, pregnancy, and birthing details of the mother were obtained by face-to-face interview at recruitment.
Temperature assessment instruments
Refrigerator thermometers (CaterChef brand digital fridge/freezer thermometer) in the staff refrigerator of the neonatal unit and laboratory refrigerator were used to maintain daily temperature logs throughout the study period.
Temperature was recorded every 5 minutes using the Tinytag Transit 2 temperature data logger TG-4080 in Ziploc bags next to the milk bottles. The recordings were downloaded to the computer after 72 hours.
Data analysis
Analysis was conducted using SPSS, version 16.0, and descriptive statistics (means and proportions, etc.) presented.
Ancillary study
To test mother's milk that was actually expressed at home and transported to the hospital, we conducted a second smaller study 2 months after the main study. We recruited 11 consecutive eligible and consenting women, who had not participated in the main study, at the time of their infants' discharge from hospital. The eligibility criteria were the family could travel from the home to hospital within 1 hour, the infant would be receiving expressed mother's milk at home, and they would be attending the follow-up clinic within 2 weeks of discharge. Information provision and consent were similar to the main study. Mothers boiled the collection bottles at home before use and were asked to follow written instructions for collection and storage of the three bottles of milk—A, B, and C. Ziploc bags and data loggers were used as in the main study. The only difference in the flow of samples from the main study was that milk in bottle C was collected the day before coming to the hospital and it remained in the participant's home refrigerator for 24 hours. The mothers brought all three bottles to the hospital clinic in the specified containers. The bottles were immediately taken to the laboratory. Telephone reminders were provided to participants.
Ethical considerations and approval
Ethical approval was obtained from the Ethics Review Committee of the Faculty of Medicine, University of Kelaniya, Ragama, Sri Lanka (P/237/09/2017), and the Human Research Ethics Committee of the College of Science, Health and Engineering, La Trobe University (Melbourne, Australia).
Results
Demographic characteristics
All eligible mothers were approached during the study period (February to August 2018) except for approximately 12 weeks when laboratory staff were intermittently engaged in union action and recruitment was paused. All those approached consented to participate (n = 51), but one baby's condition deteriorated overnight after a woman consented, so this woman was withdrawn, leaving 50 women. Demographic and birthing details are available in Table 3.
Mother's Characteristics (N = 50)
SD, standard deviation.
Microbiology
Main study: in bottle A, three samples (6%) did not have any growth even after 72 hours, while 30% (15/50) of samples were positive initially. Of the 28% (13/47) of samples that were positive at 48 and 72 hours, 85% (11/13) were positive from time of collection. The organism found in 87% (13/15) of samples that were positive on initial culture was S. aureus. In bottles B and C, the number of positive samples gradually went down over time with refrigeration. Further details are available in (a) in Table 4.
Microbiological Results
Culture missed: performance of culture inadvertently missed by laboratory staff.
X, no culture as per the study protocol.
Ancillary study (milk brought from home): (b) in Table 4 provides the percentages of samples with positive bacterial counts at various time points under different conditions. Initial culture was positive in 54% (6/11) of samples, with four of the positive samples having significant growth of S. aureus and two of Escherichia coli.
Temperature
Temperature results were obtained by perusing data logger recordings and refrigerator temperature logs. Expressed milk was collected in the hospital at room temperature that ranged from 23°C to 28°C with a mean of 25.9°C. During the 6 hours that bottle A was at room temperature, the maximum temperatures to which each sample was exposed over 6 hours ranged from 26°C to 30.6°C, with a mean temperature of 27.5°C for recordings made at 6 hours. The temperature recorded by the data loggers, when in the laboratory refrigerator, ranged from 0.5°C to 6.2°C. The mean refrigerator temperature was 4.1°C at 24 hours.
Discussion
The most prominent finding from this study was that the majority of milk samples with positive bacterial counts showed growth at initial culture soon after collection. Therefore, it was not storage and transport that were the main contributors to bacterial growth in expressed human milk, but rather bacteria already present in the milk or introduced during expression/collection. Human milk contains a wide range of microbiota.7,38 Strict versus standard hygienic practices have not shown a difference in milk bacterial counts. 28 Education and reminders about hygienic practices have consistently resulted in lower bacterial counts in milk in other studies.23,26,29 The evidence regarding use of pumps versus hand expression and bacterial counts is equivocal.22,24 In Sri Lanka, most mothers expressing milk for hospitalized infants do so by hand. Higher contamination in milk expressed at home rather than the hospital has been noted in several studies.24,27,28 Our ancillary study showed a similar trend. This raises the possibility of lower adherence to hygienic practices at home where mothers have many other commitments and distractions. Therefore, if Sri Lankan mothers are to be allowed to express milk at home for hospitalized infants, the importance of adhering to recommended hygienic practices needs to be stressed.
There was a rise in bacterial counts (statistically nonsignificant, probably due to the small sample size) from 4 to 6 hours when milk was kept at room temperature. This rise in bacterial counts suggests that 6 hours may be too long—under Sri Lankan environmental conditions of our study (26–30.6°C)—for mother's milk to be kept at room temperature if it is to be stored further in the refrigerator and administered later to infants in the neonatal unit. Previous studies recommend 4 hours or less as a safe storage duration when room temperature is 27–32°C, 12 30–38°C, 15 25°C, 14 or 24°C 19 and 8–9 hours with temperatures of 15–27°C 15 or 30°C. 18 The Human Milk Banking Association of North America and the World Health Organization recommend 4 hours at room temperature.35,39
Milk samples that were in the cool bag for the 6 hours of simulated transport did not show an increase in the number of samples with significant bacterial counts, which implies that if expressed mother's milk is to be transported in Sri Lanka, it should be done using a cool bag that would maintain bacterial counts at static levels. Expressed human milk that was stored and transported to simulate conditions where mothers would store milk expressed at home for over 1 day in the home refrigerator and travel with it to the hospital the next day, with the milk in a cooler container, also had shown acceptable bacterial counts for the process of storage and transport. In the two sets of milk samples that were always stored in the refrigerator and transported only using a cool bag, the number of samples with significant bacterial counts dropped by 72 hours to about half of the number that had significant counts at the time of collection. Human milk that has not been pasteurized is biologically active and has numerous antipathogenic properties that could have contributed, along with refrigeration, to the drop in number of positive samples. 10 This was an encouraging result for those mothers wishing to travel from home to the hospital. Several authors have reported that bacteriology of expressed mother's milk has remained stable during refrigeration for up to 96 hours,16,17 120 hours,10,35 and 6 days, 19 while other studies have monitored the milk for shorter refrigeration periods, 24 hours11,15 and 48 hours, 9 and deemed these periods as safe.
Implications
Our findings suggest that 4 hours appears to be a safe duration at room temperature for expressed human milk for hospitalized infants in Sri Lanka. Bacteriology of milk samples stored and transported using economical methods for 72 hours suggests that mothers who wish to travel from home can safely bring milk expressed and stored at home to the hospital. The importance of adhering to recommended hygienic practices at home needs to be stressed to such mothers as most samples that had significant bacterial counts had these from the time of collection.
Long-term surveillance of infection-related conditions, for example, necrotizing enterocolitis, should be in place if the current practice of providing only fresh expressed mother's milk to infants in the neonatal unit is changed to allow mothers to bring stored mother's milk to the hospital to monitor safety of this new practice on infants' health.
Limitations
This study has a small sample size and was conducted in a single center: a larger sample size under real, rather than simulated, conditions could enable firmer conclusions and should be replicated in other Sri Lankan centers to make generalized recommendations for the entire country.
Conclusions
In this simulation study, it was found that mother's own milk, which was expressed for later use by infants in neonatal units, could be transported in an economical cool bag for up to 6 hours and kept refrigerated for the remainder of 72 hours from the time of expression in a tropical climate without compromising microbiological safety.
Footnotes
Authors' Contributions
Authors of this article contributed substantially to the concept of the study and data collection, analysis, or interpretation. All contributed to drafting and revising the article and provided final approval.
Acknowledgments
The authors wish to acknowledge the contribution made by mothers of infants in the neonatal unit who willingly participated in the study.
Disclosure Statement
All authors have no conflicts of interest to declare.
Funding Information
This study was funded by a research grant from the University of Kelaniya, Sri Lanka.