
Abstract
Background:
Maternity care practices such as skin-to-skin care, rooming-in, and direct breastfeeding are recommended, but it is unclear if these practices increase the risk of clinically significant COVID-19 in newborns, and if disruption of these practices adversely affects breastfeeding.
Methods:
We performed a retrospective cohort study of 357 mothers and their infants <12 months who had confirmed or suspected COVID-19. Subjects came from an anonymous worldwide online survey between May 4 and September 30, 2020, who were recruited through social media, support groups, and health care providers. Using multivariable logistic regression, Fisher's exact test, and summary statistics, we assessed the association of skin-to-skin care, feeding, and rooming-in with SARS-CoV-2 outcomes, breastfeeding outcomes, and maternal distress.
Results:
Responses came from 31 countries. Among SARS-CoV-2+ mothers whose infection was ≤3 days of birth, 7.4% of their infants tested positive. We found a nonsignificant decrease in risk of hospitalization among neonates who roomed-in, directly breastfed, or experienced uninterrupted skin-to-skin care (p > 0.2 for each). Infants who did not directly breastfeed, experience skin-to-skin care, or who did not room-in within arms' reach, were significantly less likely to be exclusively breastfed in the first 3 months, adjusting for maternal symptoms (p ≤ 0.02 for each). Nearly 60% of mothers who experienced separation reported feeling “very distressed,” and 29% who tried to breastfeed were unable. Presence of maternal symptoms predicted infant transmission or symptoms (adjusted odds ratio = 4.50, 95% confidence interval = 1.52–13.26, p = 0.006).
Conclusion:
Disruption of evidence-based quality standards of maternity care is associated with harm and may be unnecessary.
Introduction
In March 2020, recommendations for the maternity care practices for mothers infected with SARS-CoV-2 and their infants were inconsistent. The standards of quality for maternity care practices that support breastfeeding serve as the framework for the Baby-Friendly Hospital designation. 1 Although as early as March 2020, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) had strongly recommended breastfeeding and skin-to-skin contact,2,3 recommendations from others varied.4–8 The risk of direct contact with newborns was unknown, and in some countries, infants were routinely separated from their mothers if the mothers had known or suspected infection.
Many countries issued guidance to separate or considering separating mothers from their newborns (Philippines, Malaysia, China, and initially the United States),4,7,9–11 sometimes while allowing expressed mothers' milk to be fed to the infant by an uninfected caregiver. 7 Other countries, particularly in Europe and Latin America, recommended maternity care practices during the pandemic that were consistent with WHO/UNICEF pandemic guidelines with respect to breastfeeding, skin-to-skin care, and rooming-in.5,6,12–17
Although there have been several commentaries on the importance of keeping mothers and infants together and supporting breastfeeding practices,18–21 there have been little published data on Baby-Friendly practices such as uninterrupted skin-to-skin contact, direct breastfeeding, or rooming-in with the infant within arms' reach during the pandemic, as related to viral transmission. We were specifically interested in testing the infant being within arms' reach, which allows for easier feeding and recognition of hunger cues, 1 as opposed to being in the same room but out of reach, for example, 2 m away.
Since launching our study, several studies have been published. One study estimated the negative effects of separation on breastfeeding both in-hospital and after discharge. 22 The American Academy of Pediatrics (AAP) perinatal COVID-19 registry published online data about the safety of rooming-in and direct breastfeeding in July and October, with >3,500 mother/infant dyads, but did not include specifics about infant distance from the mother. 23
In July and August 2020, data were published by 2 metropolitan New York hospitals that practiced rooming-in, skin-to-skin care, and direct breastfeeding, each with very different transmission rates (0% and 6.7%).24,25 Another study was published in October from one large academic medical center in New York which allowed rooming-in and direct breastfeeding. 26 In all three of these studies, safety measures, masks, and hand hygiene were practiced and no sites experienced COVID-19-related adverse outcomes in the newborns. A multicenter Spanish study where breastfeeding and skin-to-skin care was often allowed was published in September and showed no SARS-CoV-2 transmission to newborns. 27 In an October meta-analysis of 176 cases from 74 published articles of neonatal SARS-CoV-2 infection, mother–baby separation appeared to be beneficial. 28 Hospital-based studies may not capture the same kind of data as directly asking mothers themselves about their experiences.
In March of 2020, we sought to examine whether rooming-in within arms' reach, direct breastfeeding, and uninterrupted skin-to-skin care were inferior to separation with regard to viral transmission and/or clinically significant COVID-19, and whether breastfeeding might protect infants against hospitalization for COVID-19. We also wanted to examine the effects of separation on the mother.
Materials and Methods
In this document, “COVID-19” refers to infection with SARS-CoV-2, which can be asymptomatic. “Confirmed COVID-19” means laboratory confirmation of infection, that is, “SARS-CoV-2+.” “Suspected COVID-19” indicates infection was suspected or likely because of the history, symptoms, and/or other tests, but no test for SARS-CoV-2 was performed, or infection was suspected even if a test did not show SARS-CoV-2.
We conducted a retrospective cohort study comprising of a one-time online survey of mothers with laboratory-confirmed or clinically suspected COVID-19. It included questions about their maternity care experiences, their and their infant's symptoms, their and their infant's SARS-CoV-2 test results, and their feeding history. Mothers were excluded if they were <18 years, if they were not the female birth mother, if the infant was not over 1 month old when the mother completed the survey, or <12 months old at the time of the infection, and neither the mother nor the infant had confirmed or suspected COVID-19.
The survey was terminated if the respondent did not meet screening criteria. We required the mother to wait until her infant was at least 1 month old to complete the survey so that we could learn the eventual outcomes of her birth experiences. We limited the survey to cisgender biological mothers so that there would not be known biological or hormonal reasons for breastfeeding problems (see online Supplementary Appendix SA1). At the time of our study launch, the countries with the highest prevalence of COVID-19 included the United States, Italy, and Spain.
The survey was eventually conducted in 10 languages (see Survey text online). English, Spanish, and French versions launched initially on May 4, 2020. Chinese and Japanese versions were added in early May. Residents of European countries were excluded until July 1, at which time Italian and German versions were added. Brazilian Portuguese was added shortly thereafter. Hindi and peninsular Arabic were added in August. The study was closed on September 30, 2020, guided by the desire to provide evidence to support clinical practice at a time when the evidence was scarce.
Respondents were told that their responses were anonymous. To more easily meet the requirements of the General Data Protection Regulation necessary for distribution in European countries, IP addresses were not collected and European respondents were informed of this fact in their consent question. Survey settings allowed a respondent to retake the survey, as several conditions made it necessary for mothers who were initially screened out to retake the survey later (e.g., infant age <1 month, or country of residence). However, this added the potential for duplicate responses.
Retrospectively, we evaluated every response and excluded those that had a high likelihood of being nongenuine, were duplications, or had responses not relevant to mother–infant transmission (Fig. 1 and Supplementary Appendix SA1). These criteria included responses in which the infant and maternal infections were separated by more than 1 month, responses in which the infant infection preceded the maternal infection, responses with rapid sequential timestamps in the same language together with inconsistent answers (e.g., a mother who said COVID-19 was not suspected at delivery but also said her doctor or midwife suspected it at delivery), and those for whom the language of the response was very incongruous with the stated country of residence. For example, we deleted a respondent who answered in Japanese as a resident of Malawi (see online Supplementary Appendix SA1). We erred on deleting suspicious survey respondents at the risk of deleting some genuine ones.
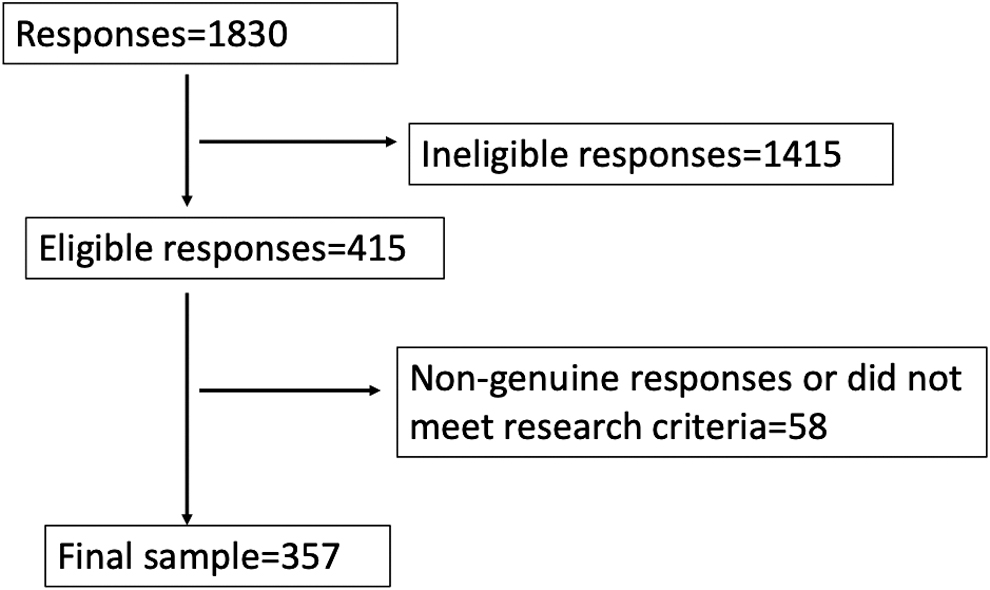
Enrollment diagram.
Mothers were recruited through social media platforms, particularly those of mothers' groups and breastfeeding support organizations, such as La Leche League (United States and worldwide), US Baby Cafés, Amamanta (Spain), and the Italian Breastfeeding Movement; through local offices of the U.S. Supplemental Nutritional Program for Women Infants and Children (WIC); through health care providers who knew of mothers who had had COVID-19, including lactation specialists, midwives, and physicians, including members of the Academy of Breastfeeding Medicine; and by word of mouth. There was no compensation for participation.
Our initial primary outcomes were assessment of infant SARS-CoV-2 infection and severity in neonates by exposure to rooming-in, direct breastfeeding, and skin-to-skin care from mothers with confirmed and/or suspected COVID-19. Secondary outcomes included assessment of SARS-CoV-2 infection and severity among infants 1 month old or older after exposure to mothers with confirmed or suspected COVID-19, as predicted by the exposure to exclusive breastfeeding. Secondary outcomes also included assessing the average duration of self-reported separation from mothers and neonates owing to COVID-19, and whether such separation caused maternal distress or impacted her ability to breastfeed.
Sample size and statistical analysis
Estimations of sample size before recruitment were challenging as there were no known estimates of effect size of maternity care practices and breastfeeding on infant transmission or hospitalization. We estimated a sample size of 324 would be sufficient to detect a 7% difference in any of our three primary outcomes at an alpha of 0.05 and power of 0.8. Statistical analysis was performed using Stata version 16 and SAS version 9.4.
For all outcomes examining infant illness, outcome was a dichotomous variable using the combined outcome of testing positive or having symptomatic infection versus no infection. We estimated breastfeeding outcomes from the question “How would you describe your baby's diet in the first 3 months of life?” The respondent could pick from 4 possible choices ranging from exclusive breastfeeding/human milk feeding to feeding exclusively with infant formula. Although all mothers answered this question and the questions about maternity practices, we adjusted for maternal symptoms using only those mothers who reported infection in the first 3 months of their infant's life to match the predictor of infant diet in the first 3 months of life. In the analysis, exclusive breastfeeding and direct breastfeeding were handled as dichotomous variables. Skin-to-skin care, maternal symptoms, infant diet, and rooming-in were handled as ordinal/indicator variables, except when collapsed into dichotomous variables when appropriate (e.g., for logistic regression outcomes or Fisher's exact testing). Direct breastfeeding and hospitalization were handled as dichotomous variables. Outcomes were analyzed using multivariable logistic regression, except for certain analyses with small sample sizes, where we used Fisher's exact test. Severity of maternal illness was considered a confounder for maternity practices on infant illness, and infant diet was a potential confounder in examining effect of maternal symptoms on infant illness. Sensitivity analyses were also performed.
The study was deemed exempt by the Institutional Review Boards (or their equivalents) of Harvard University, Cooper University Health Care, the National Institute of Health of Italy, the Ministry of Health of Spain, Hospital Sofia Feldman in Belo Horizonte, Brazil, and complied with the General Data Protection Regulation. The study was unfunded.
Results
A total of 1,830 responses were obtained, of which 415 met eligibility criteria. Among the 1,415 ineligible responses, almost all fulfilled one or more of the following criteria (in order): (1) neither mother nor baby had confirmed or suspected COVID-19, (2) respondent did not finish the survey, (3) infant was either >12 months or <1 month (Fig. 1 and Supplementary Appendix SA1). Of those remaining, 58 were deleted because they met criteria for having a high likelihood for being not genuine, being duplications, or their responses indicated situations irrelevant to mother–infant transmission (Supplementary Appendix SA1). A total of 357 responses remained for analysis (Fig. 1, and summarized in Tables 1–3). Included respondents came from 31 countries, mostly from the United States, Europe, and Latin America (Table 1). Despite significant outreach, no eligible responses were obtained from China, Japan, or India. The respondents overwhelmingly breastfed their infants, with <2% of all respondents answering that they only used infant formula during their infant's first 3 months (Table 3). Just over 1/3 (36.1%) of the total sample of 357 were mothers who reported a confirmed or suspected infection when their infant was a neonate (≤30 days old) (Table 1).
Maternal and Infant Characteristics (All Mothers Had Infants)
Because mothers of neonates completed the survey at least 1 month after giving birth, they would have known test results if a test was carried out. Thus, if they answered “suspected COVID” in the survey, they likely were not tested or infection was suspected even if a test did not show SARS-CoV-2. In the beginning of the pandemic, testing was not readily available in many locations.
ICU, intensive care unit.
Differences in Maternity Practices Between Neonates Affected by Possible COVID-19 and Older Infants Whose Births Were Not Directly Affected by COVID-19
We asked all mothers about their maternity care practices. The table depicts maternity practices among neonates directly affected by possible maternal infection, compared with those of older infants whose births were not directly affected by possible maternal infection.
CI, confidence interval.
Diet of the Infants
n/a, not applicable.
In six cases, only the infant had confirmed or suspected COVID-19, and not the mother. Of these six cases, four had a positive test. All such infants were at least 1 month old, and five were from the United States or Europe. There were 11 hospitalized infants, only 6 of whom were SARS-CoV-2+. Of the 11, 2 required mechanical ventilation, both of whom were neonates, and one of whom was not SARS-CoV-2+ but whose mother tested positive (and resided in a high-income country). There were two other hospitalized neonates who did not require mechanical ventilation, only one of whom was SARS-CoV-2+. The seven remaining hospitalized infants included two of the six infants whose mother did not have COVID-19. Only one of these two infants was SARS-CoV-2+, calling the diagnosis into question. Among the 11 hospitalized infants, 4 were from the United States, 4 were from South America, and 3 were from Europe. None of the 11 infants were reported to have underlying medical problems, including prematurity. Given that only 6 of the 11 hospitalized had positive tests, including only 1 of the ventilated infants, it is unclear how many of the 11 infants actually had COVID-19 and if so, if that was the reason for hospitalization and/or mechanical ventilation.
Primary outcomes
We found no statistically significant increase in the odds of the combined outcome of an infant becoming SARS-CoV-2+ or getting symptoms when we compared neonates who were skin-to-skin uninterrupted for ≥1 hour with those who were taken from their mothers in the first hour, adjusting for maternal symptoms (Table 4, Table S1 and Supplementary Appendix SA1). Sensitivity analysis showed similar results (Table S1).
Summary of Outcomes
aOR, adjusted odds ratio; CI, confidence interval; n/a, not applicable; OR, odds ratio; SARS-CoV-2+, tested positive for SARS-CoV-2.
We found no statistically significant increase in the odds of the combined outcome of an infant becoming SARS-CoV-2+ or getting symptoms when we compared neonates who were rooming-in at arms' reach with those kept in a separate room, adjusting for maternal symptoms. An additional sensitivity analysis showed similar results (Table 4 and Supplementary Appendix SA1).
We also found no significant increase in the risk of the combined outcome of an infant becoming SARS-CoV-2+ or getting symptoms, when we compared direct breastfeeding with feeding human milk by other means. We found no increased odds of this combined outcome compared with feeding any type of milk by other means, adjusting for maternal symptoms.
We found a nonsignificant decreased risk in neonatal hospitalization for each of the three exposures. Of note, the study was underpowered for neonatal outcomes to make a definite conclusion that these three Baby-Friendly practices were noninferior to the alternatives tested.
Secondary outcomes
We did not find a statistically significant protective effect of exclusive breastfeeding in the first 3 months of life on the combined outcome of contracting SARS-CoV-2 infection or getting symptomatic disease on infants >1 month of age, adjusting for maternal symptoms (Table 4).
“Separation due to COVID-19” was reported in 36 mothers of neonates (27.9%). A large proportion of these mothers (58%) reported feeling “very upset or distressed” because of the separation, with 78% reporting at least moderate distress. Nearly one third of separated mothers (29%) were unable to breastfeed once reunited, despite trying. Average length of separation was 6–7 days.
Additional outcomes
Our study had a low proportion of mothers reporting that they were asymptomatic in the perinatal period (≤3 days of age), 34%, and a very low proportion, 9%, in the postneonatal period (1–12 months of age). The rate of positive tests in the perinatal period was 7.4% among infants with SARS-CoV-2+ mothers (Table 1). A high proportion of infants were reported to have symptoms and positive SARS-CoV-2 tests. We thus examined if symptomatic mothers were more likely to transmit the virus and found that infants of any age of symptomatic SARS-CoV-2+ mothers had 4.50 times the odds of the combined outcome of becoming SARS-CoV-2+ or getting COVID-19 symptoms compared with mothers who had no symptoms, adjusting for infant diet in the first 3 months of life (95% confidence interval: 1.52–13.29, p = 0.006), but no significant increased odds when stratified by infant age (Table 4).
We examined additional effects by looking at disruption of Baby-Friendly practices on breastfeeding outcomes (Table 4). The adjusted odds of exclusive breastfeeding at 3 months was markedly lower if infants were kept in a separate room compared with arms' reach (0.26, p = 0.001) or who were taken from their mother at birth compared to being held skin-to-skin for at least an hour at birth (0.38, p < 0.017). In addition, infants who did not experience direct breastfeeding had lower odds of exclusive breastfeeding in first 3 months (0.17, p < 0.001), compared with any milk not fed directly.
Discussion
Our study is unique in including participants from 31 countries, in having maternal viewpoints, and in using a unique dataset of subjects. Our study captures maternity care practices in the detail not routinely available in medical records or registries. Lack of rooming-in because of COVID-19 has previously shown to decrease the likelihood of breastfeeding. 22 However, ours is one of the few studies to contribute safety data on the clinically relevant risks of infection with rooming-in at arms' reach, uninterrupted skin-to-skin contact for >1 hour, and direct breastfeeding, at least for predominately breastfed infants.
Our findings contradict those reported in a recent systematic review suggesting that “separation” (not defined) is beneficial. 28 To our knowledge, it is also the first study to show the harms of deprivation of skin-to-skin contact and deprivation of direct breastfeeding in the setting of COVID-19. Furthermore, our data show that removing an infant from the mother after birth, keeping an infant in a separate room, and preventing direct breastfeeding, markedly undermine exclusive breastfeeding later in infancy.
Our findings have implications for infant health and survival. Undermining exclusive breastfeeding puts infants at risk of other infections, hospitalization for other lower respiratory tract infections, and increased infant mortality.29,30 Delayed breastfeeding initiation increases the risk of infant mortality. 31 Skin-to-skin contact is important for thermoregulation of the newborn, glucose homeostasis, bonding, and breastfeeding. 32
Although our data did not show an association with breastfeeding and protection from SARS-CoV-2 in infants over 1 month old, this finding may be because we had very few infants in our sample who were not at least partially breastfed. The very high proportion of breastfed infants in our sample reflects the fact that we largely distributed the survey through breastfeeding networks. Because few infants with COVID-19 get severely ill, a large sample is required to assess the risk of such rare events.
We noted a higher rate of symptomatic mothers than has been reported in some other studies,23,24 likely because of self-selection. Our proportion of symptomatic SARS-CoV-2+ mothers in the perinatal period, 62%, is much higher than the 23% reported by the AAP in their registry as of October 3, 2020, 23 but similar to that seen in the Italian Obstetric Surveillance System, 72% on admission, 33 and in one New York hospital system (Presbyterian), 74%, 25 nearly half of whose mothers had their symptoms >2 weeks before delivery. Our rate of SARS-CoV-2+ infants in the first 3 days of life, 7.4%, is higher than the AAP reported rate of 1.7%, 23 the United Kingdom Obstetric Surveillance System, 5%, 34 in the Spanish data, 5.2%, 27 and that seen in the worldwide review of infants of over 660 pregnant women with COVID-19, 4%, 35 but it is consistent with that seen in the Italian data, 6.1%, 33 and in another New York hospital (Elmhurst), 6.7%. 24
Although it may appear that our neonatal hospitalization rate is high compared with that reported in the literature (5.6 per 10,000 livebirths in the United Kingdom), 36 we do not have a true numerator, so that even if all 4 hospitalized neonates in our study were American (instead of from 31 countries), our hospitalization rate would be 0.01 per 10,000.
Some studies have shown low infant positivity rates, including the SET-NET data (2.6%), 37 and the Presbyterian data (0%). 25 However, significant proportions of these mothers were no longer contagious at the time of delivery (64% and 34%, respectively). This may explain low infant positivity rates seen in other studies, especially those involving pregnancy registries.
Given international participation, our study is more generalizable than those from a single site or region. We have been able to collect a sizeable amount of data despite COVID-19 cases being relatively few in all series. Nonetheless, given that hospitalization is a rare outcome, very few studies, even those with pooled data, have sufficient power to detect significant effects from any intervention.
An association between symptomatology and contagion has not been previously well described in the literature, and our study adds to the epidemiologic evidence that people with symptoms may indeed be more contagious. This appears to be driven by the greater, but nonsignificant, effect of transmission we found among older infants compared with neonates. Sample sizes in the two individual age categories were likely too small to show effects by themselves, but the combined sample of all infants was significant. However, neonates may indeed be less susceptible to transmission. Recent evidence shows that neonates are not colonized with viruses until later months of life, and breastfed infants are colonized with far fewer viruses. 38 The vast majority of our symptomatic infants had “mild” symptoms. The issue of most clinical concern is not mere transmission but serious complications such as hospitalization, and we showed a nonsignificant decrease in risk, not an increase in risk.
Our study is one of the few to examine mothers' experiences of separation, and the harm that this practice can bring both to the success of breastfeeding and to mothers' emotional health, 22 already at risk during the pandemic. 39 Our finding that 29% of separated mothers who intended to breastfeed were unable to do so is consistent with other reported literature from the pandemic. 22
As the northern hemisphere enters influenza season, it is worth noting the risks we identified when considering the management of birthing mothers with influenza-like illness. Unlike WHO, 40 CDC currently recommends separation for influenza, 41 but other measures may suffice, given the harms of separation.
More research is needed on how best to protect infants of symptomatic mothers from severe disease while supporting breastfeeding. In the meantime, we must emphasize meticulous attention to respiratory and hand hygiene for symptomatic mothers, both in the hospital and at home.
Our study is limited by neonatal sample size that did not allow for detection of noninferiority in neonatal outcomes by exposures of interest. The exceptionally low reported hospitalization rate in the literature 36 indicates it may be nearly impossible to demonstrate a clinical benefit from disrupting Baby-Friendly practices. We were also limited by our lack of ability to verify responses with IP addresses, which would have allowed us to verify the global location of a respondent and better confirm genuine responses and eliminate duplicate responses. However, the complex algorithm of the survey response options made it more likely that only genuine respondents would give consistent answers, allowing detection of responses that were not genuine.
Because of self-selection, patients were subject to selection and recall bias, which may have skewed data toward reporting sicker outcomes. We also were limited by lack of access to infant records to verify why infants were hospitalized or mechanically ventilated to confirm COVID-19 diagnoses, and we suspect that some of the hospitalized infants may not have actually had COVID-19. Like most studies, we did not study variables such as hand hygiene, mask use, and use of enclosed cribs.
Like many studies, our study had a very high proportion of breastfed infants; this may limit its generalizability to nonbreastfed infants. Generalizability may be limited because we did not use random sampling. We were also unable to survey mothers without internet access, so we may have undersampled lower income populations, resulting in fewer sicker subjects. Oversampling of breastfeeding subjects in high-income countries may also have undersampled sicker or more vulnerable subjects. We did not specifically ask about bedsharing or sleep practices, which is an issue particularly for older infants, and in some countries where bedsharing may be practiced in delivery settings. We did not capture finer timeframes of infant feeding outcomes, which could be a topic of future research. In addition, we would have liked broader participation from Asia and Africa.
Future research is needed with a larger sample of nonbreastfed infants to further delineate the risks of COVID-19 in such infants, and risks of symptomatic mothers stratified by infant age.
Conclusion
Our research contributes to the emerging evidence that skin-to-skin care, rooming-in within arms' reach, and direct breastfeeding may be safe for mothers infected with SARS-CoV-2. Breastfeeding is associated with a decreased risk of hospitalization for lower respiratory tract infection.42,43 Similar respiratory pathogens are not spread through human milk. Thus, policies to separate mothers and infants could potentially result in increased risk of adverse outcomes for mother and child, 29 including infant respiratory infections, such as SARS-CoV-2 and influenza, particularly if exposed later during infancy. The harms of all forms of separation associated with harms to breastfeeding and maternal stress should prompt medical authorities to question the underlying assumptions of risks and benefits behind any policy decisions that include forms of separation of mothers and infants.
Footnotes
Acknowledgments
The authors extend their heartfelt thanks to the participating mothers. The authors thank the following people: Fouzia AlHreashy, MD; Talita Balaminut, RN, PhD; Kimarie Bugg, DNP, RN, MPH, IBCLC; Judy Canahuati; Jie Chang, BSN, MBBS, MMed; Mariana Colmenares Castaño, MD, IBCLC; Jeannette T. Crenshaw, DNP, RN; Leah DeShay, BA, IBCLC; Yashika Joshi; Laura Haiek, MD; Rukhsana Haider, MD, PhD; Debbi Heffern; Juliette Hertzhaft-LeRoy, MD, DO, MSc, IBCLC; Annabelle Mackensie, MA (Cantab), IBCLC; Francesca Marchetti, RN, BMid, PhD; RuthAnna Mather, BS; Lissette Moreno, BA; Erika Nehlsen, IBCLC, EFNB; Midori Nishimura, MD, IBCLC; Sara Oberg, MD, MPH, PhD; Jennifer Pintiliano, MD; Sili Recio, BA; Elien Ruow, MD, FABM; Lourdes Santaballa, MS, IBCLC; Francesca Zambri, BSc Mid, PhD; Yushi Zhang, BS.
Data Sharing Statement
Deidentified individual participant data are not publicly available because of institutional restrictions.
Authors' Contributions
M.C.B. conceptualized and designed the study, carried out initial and subsequent analyses, helped with data collection, drafted the initial version of the article, performed data analysis, and reviewed and revised the article.
L.F.-W. conceptualized and designed the study, carried out subsequent analyses, and reviewed and revised the article.
V.V. conceptualized and designed the study, helped with data collection, performed translation of survey and recruitment material, reviewed and revised the article.
A.G. and E.M.C. contributed to study design, helped with data collection, performed translation of survey and recruitment material, reviewed and revised the article.
N.B.B., M.-T.H.-A., L.J., and E.D.D. helped with data collection, and reviewed and revised the article. M.-T.H.-A. also performed translation of survey consent material.
J.G. carried out final data analysis and critically reviewed the article.
All authors approved the final version of the article as submitted and agree to be accountable for all aspects of the work.
Disclosure Statement
No authors have financial conflicts of interest to disclose.
L.F.-W. works as a consultant and physician lead for Communities and Hospitals Advancing Maternity Practices (CHAMPS) at Boston Medical Center in Boston, MA, and consultant to National Institute for Children's Health Quality. M.C.B. and L.F.-W. serve in unpaid positions on the Board of the Academy of Breastfeeding Medicine. E.M.C. works for the Italian National Committee for UNICEF as the Baby-Friendly Coordinator.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.