
Abstract
Background:
The impact of COVID-19 vaccination on breastfeeding is unknown. The primary aim of this study was to determine whether vaccine-related side effects following COVID-19 vaccination were associated with an adverse impact on breastfeeding. Secondarily, we sought to determine perceived symptoms in breastfed children and maternal opinion about COVID-19 vaccination.
Materials and Methods:
We conducted a cross-sectional survey of breastfeeding mothers who underwent COVID-19 vaccination >2 days before the survey. Subjects were recruited through social media and websites. Data included sociodemographic information, vaccine history, maternal and child symptoms, and impact on lactation/breastfeeding. Bivariate statistics (chi-square, Wilcoxon rank sum, and t tests) and multivariable logistic regression models examined the association of vaccine side effects with lactation, symptoms in breastfed children, and maternal opinion on vaccination.
Results:
Analysis included 4,455 breastfeeding mothers. Maternal postvaccination symptoms were more common after the second dose (p < 0.001). Overall, 77 (1.7%) respondents reported a negative impact on breastfeeding postvaccination, and these mothers were more likely to have experienced fatigue, headache, muscle pain, injection site pain, chills, fever, or allergic reactions. After adjusting for confounding variables, higher odds of an adverse impact on lactation were associated with lower breastfeeding intensity, dose of vaccine, and child symptoms. Even among mothers who reported an adverse impact on breastfeeding, maternal opinion about vaccination and confidence in their decision to receive the COVID-19 vaccine were high.
Conclusions:
COVID-19 vaccination among breastfeeding mothers resulted in minimal disruption of lactation or adverse impact on the breastfed child. These findings may be considered in vaccination decision-making.
Introduction
Breastfeeding and pregnant women were excluded from recent trials evaluating novel COVID-19 vaccines. Meanwhile, in the United States and globally, women constitute the majority of the health workforce.1,2 With the U.S. Centers for Disease Control and Prevention (CDC) among those recommending health workers be included in the first phase of vaccine efforts, knowledge gaps related to COVID-19 vaccine safety in women of reproductive age are particularly glaring. Based on urgent ethical and clinical concerns in vaccinating this population, numerous health organizations have called for the inclusion of pregnant and lactating women in clinical trials.3–11
The theoretical risk of current COVID-19 vaccines adversely impacting lactation or breastfed children is quite low. However, breastfeeding mothers and their clinicians have minimal objective data to guide decisions on vaccine safety. Since the emergency use authorization of two messenger RNA (mRNA)-based COVID-19 vaccines in the United States in December 2020, COVID-19 vaccine recommendations for women who are breastfeeding have varied. Thus far, these recommendations have been based solely on expert opinion.
Citing a precautionary approach, the United Kingdom Medicines and Healthcare Products Regulatory Agency (MHRA) initially recommended that breastfeeding women be excluded from vaccination. 12 Yet, following widespread criticism from breastfeeding experts, clinicians, and other national health organizations, the MHRA reversed this original decision. 13 Currently, many regulatory agencies suggest mothers consider vaccination determined by weighing their risk of exposure to COVID-19, their personal health, and discussion with their health care provider.14–17
The initial lack of clear consistent guidelines coupled with the widespread and unprecedented publicity surrounding the development and rollout of the novel COVID-19 vaccines may adversely impact vaccine uptake among breastfeeding mothers. Awareness of the short-term outcomes related to postvaccine symptoms and the impact on breastfeeding and/or breastfed children may help guide decision-making in this special population. The primary aim of this study was to determine whether symptoms following COVID-19 vaccination were associated with an adverse impact on breastfeeding. Secondarily, we sought to determine perceived symptoms in breastfed children and maternal opinion about COVID-19 vaccination.
Materials and Methods
A cross-sectional study was conducted from January 8, 2021, to March 31, 2021. Data were collected through an online questionnaire. The survey was distributed online through the InfantRisk Center website, Facebook, and Twitter. Eligibility criteria were as follows: mothers currently breastfeeding or lactating, aged 18 years or above, and having received a COVID-19 vaccine more than 2 days before the survey. The Texas Tech University Health Sciences Center Institutional Review Board determined that this study was exempt from review. Response to the survey was completely voluntary and responding to the questions was considered consent.
The primary outcome (impact on lactation) was ascertained by asking mothers whether they experienced any impact on breastfeeding or their ability to express breast milk postvaccination. This dichotomous outcome was explored separately (e.g., breastfeeding impact only or milk expression impact only) and combined (any impact on lactation), as indicated in the analyses. The questionnaire also collected data on sociodemographic factors, COVID-19 vaccine history, maternal and child symptoms following vaccination, and impact on maternal activities (including household duties, childcare duties, work-related duties, or other duties). The intensity of child's breast milk intake was ascertained by assessing the proportion of child fluid intake that was maternal milk. Breast milk intensity ranged from “breast milk only” to “some breast milk, mostly other liquids.” Five items assessed maternal opinions toward vaccination. These items examined the following concepts: risk of a new vaccine, confidence in the decision to receive the vaccination, and concern about vaccine side effects. All items were rated on a 5-point Likert scale, with a rating of 1 being strongly disagree and 5 being strongly agree. We limited comparisons by vaccine manufacturer to the Pfizer–BioNTech vaccine versus Moderna vaccine because very few respondents reported receiving AstraZeneca (two respondents) and Sputnik (one respondent) vaccinations. Responses were analyzed if complete demographic information, vaccine history, breastfeeding, and postvaccine symptom responses were available.
Descriptive statistics, unpaired two-tailed t tests (for parametric distributions), Wilcoxon rank sum (for nonparametric distributions), and chi-square or Fisher exact tests assessed the association between vaccine dose or impact on breastfeeding and covariables. Multivariable logistic regression was used to determine the association of postvaccination symptoms with vaccine dose and manufacture type and also to determine the association between adverse impacts on breastfeeding and maternal postvaccination symptoms. Variables that were significant in bivariate analyses were included in the multivariable logistic regression models, which were then reduced using backward elimination. Statistical tests were performed using Stata/IC 15.1 (College Station, TX). A two-sided p-value <0.05 was considered significant.
Results
In total, 5,944 responses were received. We excluded participants who failed to meet eligibility criteria (n = 613) or did not complete the survey (n = 876). The demographic characteristics of the 4,455 mothers included in the final analysis are described in Table 1. The majority of respondents received the Pfizer–BioNTech vaccine; were predominantly health care workers; and had a bachelor's degree or higher education. More than half provided only breast milk to their children (Table 1).
Demographic Characteristics of Survey Respondents Who Received the COVID-19 Vaccine While Breastfeeding, by Dose
Bold values are significant at p-value less than or equal to 0.05.
Statistical tests performed using chi-square tests or Fischer's exact tests (when cell size was <10) unless otherwise noted.
Nonpaired t test was used for parametric variables.
Other countries included Belgium (1), Denmark (8), Germany (2), Iceland (3), Ireland (1), Israel (8), Italy (2), Japan (1), Malta (1), Philippines (1), Qatar (1), Romania (3), Russian Federation (1), Singapore (1), Slovakia (1), Spain (2), Sweden (1), and the United Kingdom (17).
Test for trend was used for the statistical analysis.
SD, standard deviation.
Maternal symptoms
Several maternal postvaccination symptoms (allergic reactions, fever, chills, muscle pain, headache, fatigue, and injection site pain) were more common after the second dose (Fig. 1).
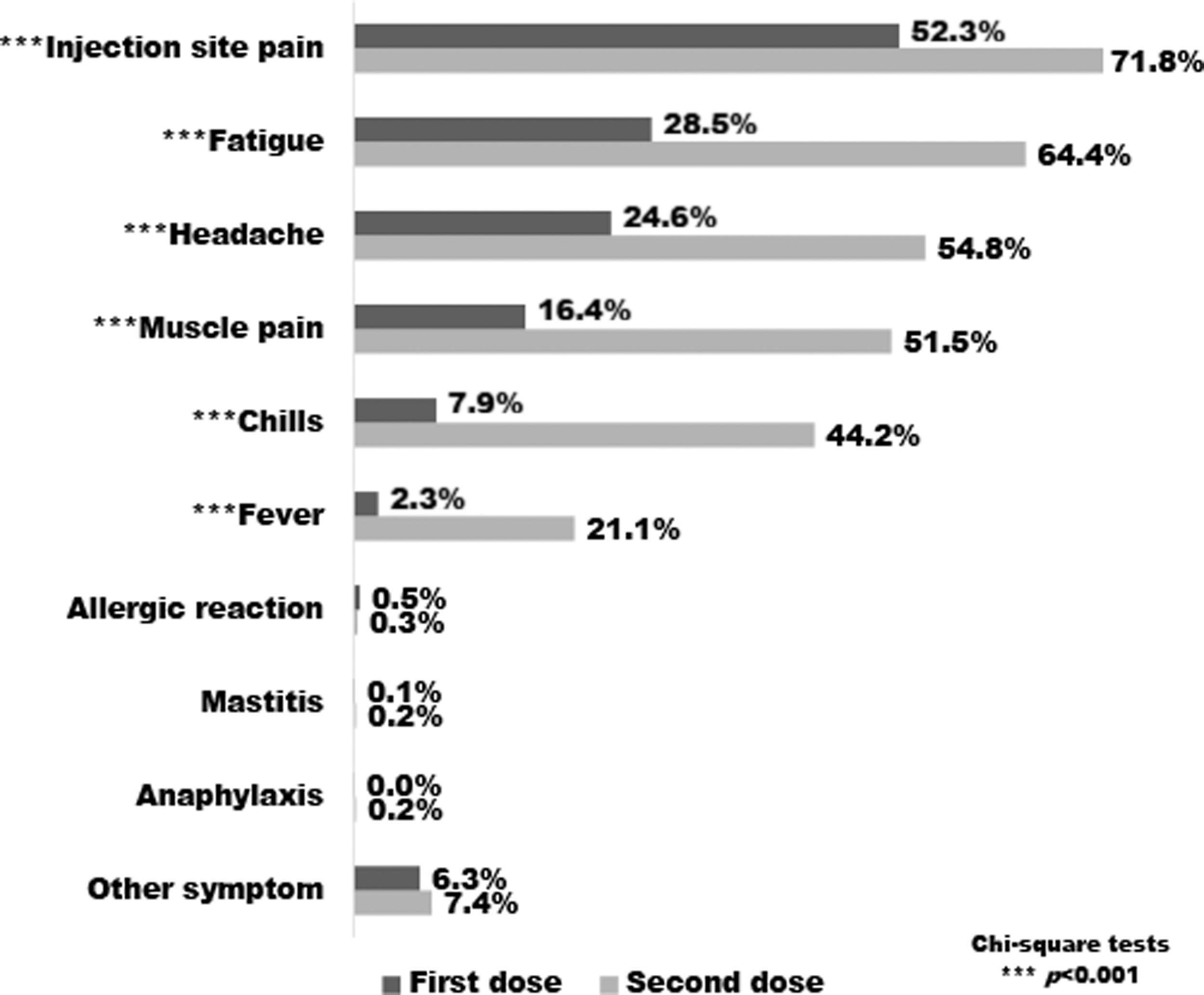
Percentage of mothers reporting side effects or symptoms following COVID-19 vaccination. Total number of mothers was 2,627 (one dose) and 1,828 (two doses); ***p < 0.001. Other side effects reported in three or more mothers included brain fog, axillary lymphadenopathy, arthralgia, rashes, clogged milk ducts, nausea, and dizziness.
The Moderna vaccine (compared with the Pfizer–BioNTech vaccine) was more commonly associated with fatigue (adjusted odds ratio [aOR] 1.8, 95% confidence interval [CI]: 1.5–2.0), headache (aOR 1.7, 95% CI: 1.5–2.0), muscle pain (aOR 1.7, 95% CI: 1.5–2.0), injection site pain (aOR 1.8, 95% CI: 1.6–2.1), chills (aOR 2.3, 95% CI: 2.2–3.3), fever (aOR 2.6, 95% CI: 2.1–3.3), and allergic reactions (aOR 8.1, 95% CI: 2.3–28.2), but not anaphylaxis (aOR 6.5, 95% CI: 0.6–66.0), when adjusting for dose number, intensity of breast milk intake, and health care worker status. Figure 2 displays the impact that vaccination had on mothers' daily activities.
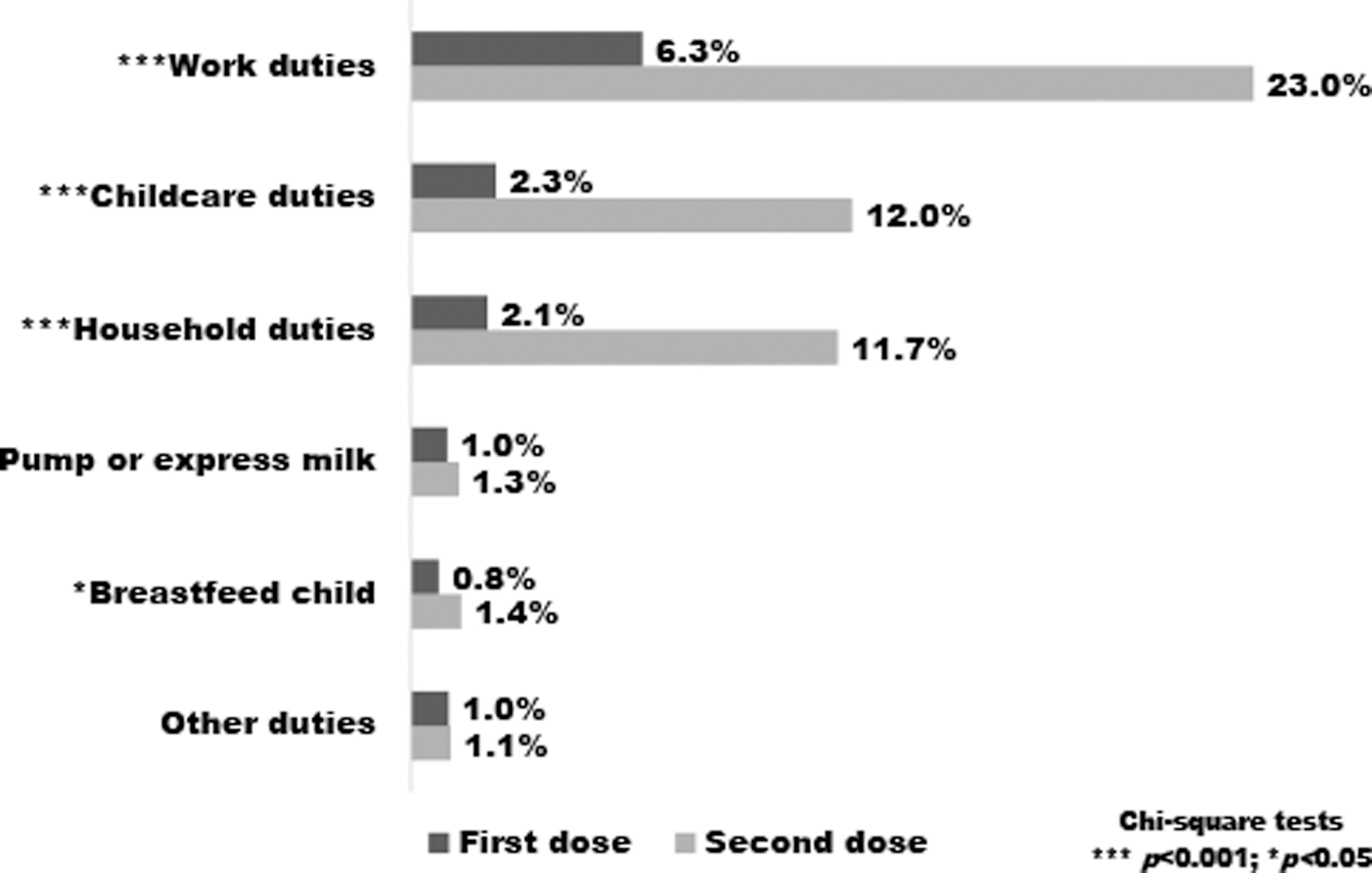
Percentage of mothers reporting an adverse impact on function following COVID-19 vaccination. Total number of mothers was 2,627 (one dose) and 1,828 (two doses); ***p < 0.001 and *p < 0.05. Other impacts described by three or more mothers included sleep alterations and disruptions or discomfort with their exercise routine.
Impact on breastfeeding
Overall, 77 (1.7%) mothers reported any adverse impact on breastfeeding following their vaccination: impacted direct breastfeeding only (n = 27, 0.6%), impacted milk expression only (n = 32, 0.7%), or impacted both direct breastfeeding and milk expression (n = 18, 0.4%). When asked about changes in milk production following vaccination, 90.1% (n = 3,898) respondents reported no change, while 3.9% (n = 168) reported an increase and 6.0% (n = 258) reported a decrease in milk production.
In bivariate analyses, there was a significant association between any adverse impact on breastfeeding and vaccine dose (1.3% first dose versus 2.3% second dose, p = 0.015), but not vaccine type (1.4% Pfizer versus 2.3% Moderna, p = 0.059).
After adjusting for confounding variables, an adverse impact on lactation was more common with receipt of a second dose, report of symptoms in the child, and the intensity of breast milk intake (Table 2).
Multivariable Odds of Adverse Impacts on Breastfeeding in Mothers Post-COVID-19 Vaccination
Bold values are significant at p-value less than or equal to 0.05.
— Indicates insufficient data.
Symptoms reported by respondents following maternal COVID-19 vaccination.
Child symptoms
Overall, 303 (7.1%) respondents reported one or more symptoms in their child following maternal vaccination. The intensity of breast milk intake was not associated with a higher rate of perceived postvaccine symptoms in the breastfed child (breast milk only 7.6%, mostly breast milk 7.1%, half breast milk 5.8%, and some breast milk 5.7%, p = 0.305). Mothers who received their second dose (compared with the first dose group) were more likely to perceive increased fussiness (2.8% versus 13.9%, p < 0.05) in their breastfed children (Fig. 3). In the bivariate analysis, perceived symptoms in the breastfed children were associated with an adverse impact on breastfeeding (6.8% versus 23.4%, p < 0.001). In the fully adjusted logistic regression model, reports of postmaternal vaccination symptoms in the breastfed child were associated with 4.0 times greater odds of any adverse breastfeeding effects (95% CI: 2.3–7.0).
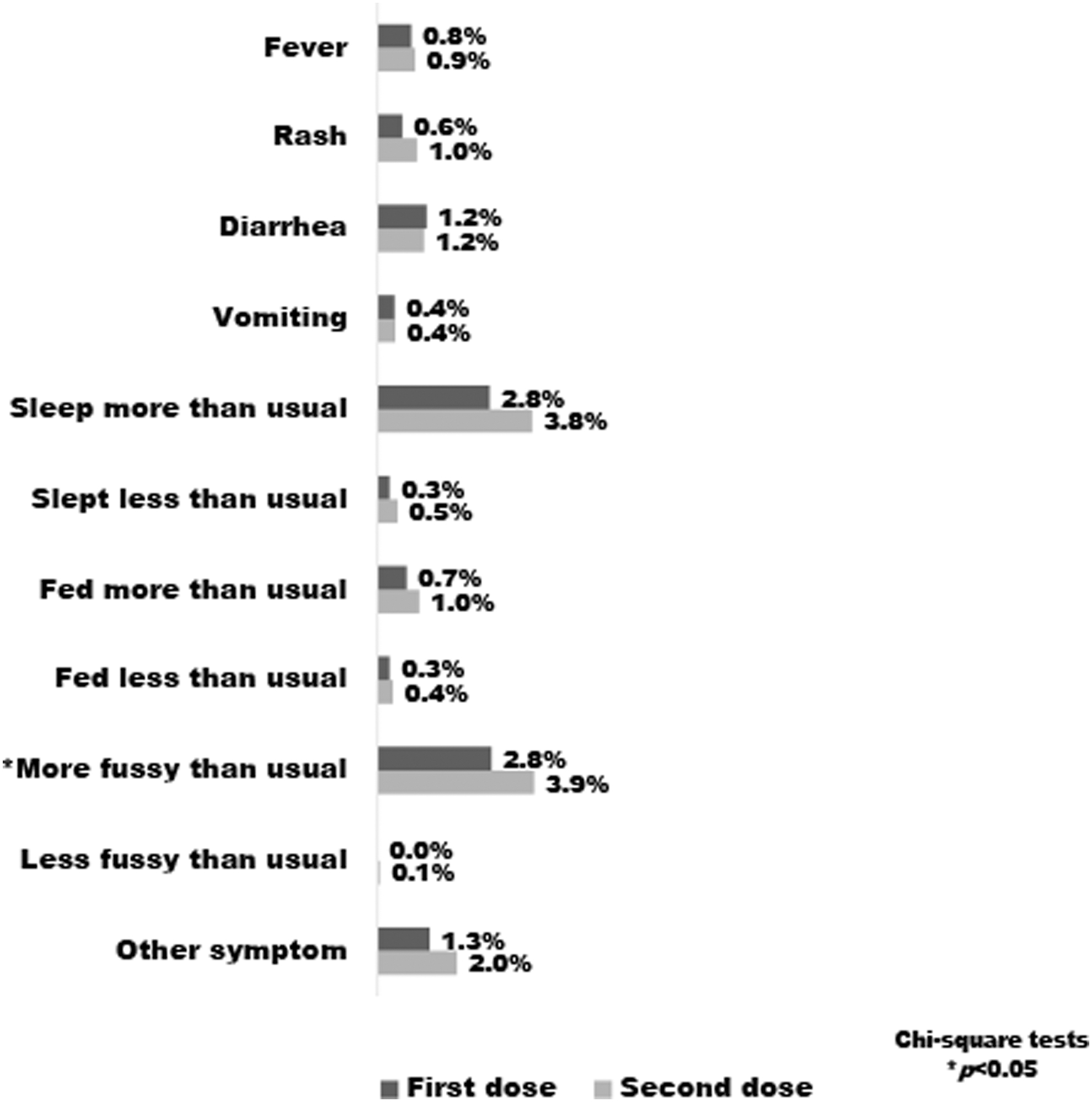
Percentage of mothers reporting symptoms in their breastfed children following COVID-19 vaccination. Total number of mothers was 2,627 (one dose) and 1,828 (two doses); *p < 0.05. Other perceived symptoms in the children reported by three or more mothers included runny nose and flushing of cheeks.
Maternal opinion
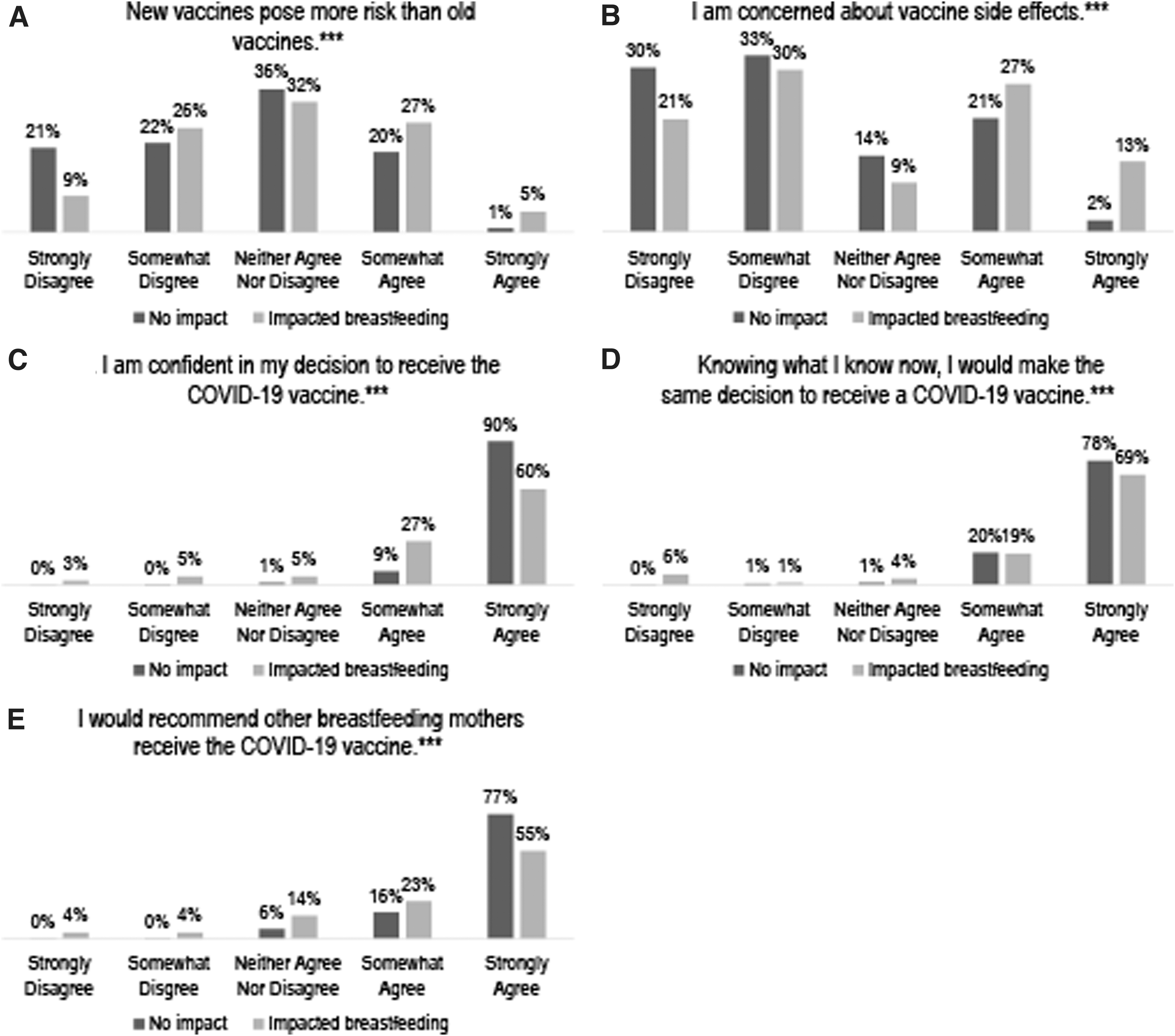
Overall, 77.3% (n = 3,278) of respondents strongly agreed that they were confident in their decision to receive the COVID-19 vaccine, while 0.2% (n = 10) strongly disagreed. Additionally, 89.4% (n = 3,793) strongly agreed that they would make the same decision again, while 0.2% (n = 10) strongly disagreed.
Mothers who experienced no adverse impact on breastfeeding (n = 4,166) were compared with mothers who reported an adverse impact on lactation (n = 77). Those who endorsed an adverse impact on lactation reported lower levels of agreement when asked about (1) confidence in undergoing vaccination, (2) recommending the vaccine to other breastfeeding mothers, and (3) making the same decision again (Fig. 4). Mothers who experienced an adverse impact on lactation were also more likely to report concerns about risks of new vaccines or serious adverse effects (Fig. 4).
Discussion
This study is unique, in that it is the first large survey of breastfeeding mothers who have received one or more doses of a COVID-19 vaccine. In addition to ascertaining the frequency of common postvaccination symptoms in mothers, this study provides clinically relevant information on how vaccine side effects might impact the breastfeeding relationship between the mother and child. Because breastfeeding is a dyadic behavior, this study contributes important information on perceived symptoms in the breastfed child following maternal COVID-19 vaccination.
Breastfeeding mothers who received the COVID-19 vaccination reported similar side effects as clinical trial participants.18–20 In addition, side effects such as injection site pain, fatigue, headache, muscle pain, chills, and fever were more common among participants who had received a second dose. Allergic reactions were less common among those who had received a second dose, which is likely because an allergic reaction to the first dose might result in a contraindication to receiving subsequent doses depending on the severity.
We did not find any literature that directly examined whether maternal symptoms following vaccination impacted breastfeeding outcomes. Although few respondents (1.7%) reported any adverse impact on direct breastfeeding or breast milk expression, we found that an adverse impact was more common among mothers who reported vaccine side effects such as fever, fatigue, headache, muscle pain, injection site pain, chills, and allergic reactions. A few plausible mechanisms by which maternal symptoms may adversely impact lactation exist. Previous studies have found that maternal illness may be associated with earlier breastfeeding cessation. 21 Maternal fever, which increases the metabolic demand and insensible water losses, could have a detrimental impact on breastfeeding by reducing the total body water available for milk production. Fatigue, especially when protracted, may also have a detrimental impact on milk supply. 22 However, since vaccine-related symptoms are typically much less in severity and duration than actual medical illness, this may explain why very few mothers in this study experienced an adverse impact on direct breastfeeding or milk expression.
It is important to note that we received far fewer responses from women who received a second dose of the Moderna vaccine. This is likely due to the fact that the Pfizer–BioNTech vaccine was the first to receive Emergency Use Authorization (EUA) in the United States.
Generally, routine vaccination is not contraindicated during lactation with notable exceptions of yellow fever and smallpox vaccines, which are both live-attenuated vaccines. 23 In concordance, we found that a higher intensity of breast milk feeding was not associated with more symptoms in the breastfed child. This supports the theoretical knowledge that mRNA-based vaccines would not be transmitted to the child through maternal milk and thus should not cause direct symptoms in the child. After controlling for confounders, we found that an increasing intensity of breast milk feeding was protective against an adverse impact on lactation. This could be because respondents who were exclusively breastfeeding may have had a more robust milk supply and/or may have been more resilient to the temporary effects of vaccination side effects. Conversely, mothers whose children had more symptoms at the time of maternal vaccination were more likely to report an adverse impact on lactation. This could be because breastfeeding routines may be altered during times of child illness.
Based on our findings, breastfeeding mothers who choose COVID-19 vaccination might expect to have more postvaccine symptoms with a second dose. Such symptoms may be more common with the Moderna vaccine compared with the Pfizer–BioNTech vaccine; however, adverse impact on lactation did not differ by vaccine type. Mothers who experience pain-related symptoms (such as headache, injection site pain, and body aches) or fever/chills may choose to treat their symptoms with antipyretics and/or anti-inflammatory medications such as ibuprofen or acetaminophen, which could reduce the severity or duration of such symptoms and minimize effects on breastfeeding. Additionally, mothers whose children are partially weaned onto other liquids might benefit from proactive measures such as ensuring adequate breastfeeding or breast milk expression frequency, hydration, and adequate postvaccine symptom management. Given the frequency with which vaccination impacted maternal household-, childcare-, and work-related activities, breastfeeding mothers may also undergo vaccination when additional help or support is available for these tasks.
As a mother discusses with her health care providers the possibility of receiving the COVID-19 vaccine while breastfeeding, it is important to consider her personal level of unavoidable exposure to COVID-19 and her individualized risk of severe COVID-19 symptoms if she became infected, as well as concerns around breastfeeding. Based on our findings, it seems that the vaccine is likely to have minimal detrimental effects on breastfeeding despite the potentially inconvenient and unpleasant short-term side effects. In the setting of a COVID-19 infection, symptoms of fatigue, headache, muscle pain, chills, and fever are likely to be more severe and longer in duration.24,25 Since these symptoms are the same as the adverse effects from the vaccine, which were associated with negative impacts on breastfeeding, the adverse effects may not be clinically relevant to most women at high risk for contracting the virus. This theory may serve as an additional impetus for the vaccine rather than against it. Furthermore, severe symptoms from an infection that may result in hospitalization are extremely likely to have a substantial negative impact on breastfeeding.24–26
Strengths of this study include the large numbers of survey respondents who received (first or second) doses of the two vaccines available at the time in the United States to power analyses of comparisons. Given that responses were received from all U.S. states and Puerto Rico and internationally, our study is more generalizable than one from a single region. This study also reports on some maternal views related to vaccination, which help further describe the attitudes of mothers in this sample.
This study is limited by the use of a self-selected sample comprising predominantly health care workers. These respondents were among the first eligible to receive the vaccine, were mostly highly educated, were of white race, and had received the Pfizer–BioNTech vaccine (especially the second dose group), which limits generalizability. Almost all respondents received either the Pfizer–BioNTech or Moderna vaccine and both use mRNA technology to elicit an immune response. Our findings may not be applicable to vaccines with other mechanisms of action, such as the live Oxford–AstraZeneca and Johnson & Johnson adenovirus-mediated vaccines, which were not yet widely available in the United States at the time of these analyses.
Conclusions
Breastfeeding mothers contemplating COVID-19 vaccination may have unique concerns such as an adverse impact on their infant or a negative impact on their ability to breastfeed or express milk. Our findings suggest that the vaccine resulted in minimal disruption of lactation or adverse impact on the breastfed child. While awaiting more definitive results from prospective randomized studies of COVID-19 vaccination in lactating mothers, our findings may help guide the clinical decision-making of breastfeeding mothers and their clinicians.
Footnotes
Authors' Contributions
S.M.L-J. conceptualized the manuscript, created the data collection instruments, performed the analyses, and drafted the manuscript. C.D.G. and K.K. conceptualized the manuscript, created the data collection instruments, and reviewed and revised the manuscript. T.W.H. conceptualized the manuscript, provided feedback on analyses, and critically reviewed the manuscript for important intellectual content.
Disclosure Statement
All the authors have no financial conflicts of interest to disclose.
Funding Information
No funding was provided for this article.