
Abstract
Background:
Vitamin D deficiency was associated with an increased risk of coronavirus disease 2019 (COVID-19) infection. Vitamin D deficient mothers are more likely to have infants with vitamin D deficiency, affecting their immunity and protection against infection. This study aimed at comparing the concentrations of vitamin D3 and T cell-related cytokines in milk between mothers with confirmed COVID-19 polymerase chain reaction (PCR) test, mothers with viral infections suggestive of COVID-19, and mothers without infection.
Materials and Methods:
Concentrations of vitamin D3 and T cell-related cytokines in milk samples were determined by ELISA from 10 mothers who had a positive COVID-19 PCR test, 10 mothers with viral symptoms suggestive of COVID-19, and 20 mothers without infection.
Results:
Vitamin D3 concentration in human milk was higher in women without infection than in women with viral symptoms or COVID-19 PCR. Interleukin-2 level in milk was higher in the no-infection group than the COVID-19 PCR group but it did not differ with the viral symptoms group. Vitamin D3 did not correlate with any cytokines in human milk. Prenatal vitamin intake did not affect the vitamin D3 in human milk. The percentage of milk from mothers with <20 ng/mL of vitamin D3 was 50% in the COVID-19 PCR group, 60% in the viral symptoms group, and 5% in the no-infection group.
Conclusions:
Vitamin D3 level in breast milk may influence maternal immunity against COVID-19 infection. A larger study is needed to evaluate the relationship between vitamin D3 concentration in breast milk, maternal immune response, and the incidence of COVID-19 infection in lactating mothers.
Introduction
Vitamin D is a steroid hormone synthesized in the skin when absorbing type B ultraviolet (UVB) sunlight or exogenous food sources and dietary supplements, including prenatal vitamins. Low serum 25-hydroxyvitamin D3 is associated with acute respiratory tract infections, including influenza1,2 and severe acute syndrome coronavirus 2 (SARS-CoV-2).3,4 Vitamin D deficiency increased the risk of coronavirus disease 2019 (COVID-19) infection and severity.3,5,6 Adequacy in vitamin D by supplementation and UVB exposure may reduce respiratory tract infections, especially in populations with vitamin D deficiency7,8 and in patients with antibody deficiency (IgA or IgG deficiency). 9 Vitamin D3 has an antiviral effect by obstructing viral replication and its anti-inflammatory and immunomodulatory properties. 10 Vitamin D3 may modulate immune function by affecting dendritic cells and T cells, which likely promote viral clearance and reduce inflammatory responses that induce symptoms. 11 Maternal vitamin D status determines the vitamin D levels of breastfeeding infants.12,13 Vitamin D deficient mothers are more likely to have infants with vitamin D deficiency, affecting their immunity and protection against infection. The impact of vitamin D3 concentration in milk from lactating women and their incidence of COVID-19 infection have not been investigated.
The CD4 T cell subsets, including T helper 1 (Th1), T helper 2 (Th2), T helper 17 (Th17), T-regulatory (Treg) cells, and T follicular helper (TFH), play a critical role in orchestrating adaptive immune responses during infectious disease. The Th1 cells predominantly produce interferon-γ (IFN-γ), interleukin-2 (IL-2), and tumor necrosis factor-beta (TNF-β)14,15 and help the entry of T cells into the sites of infection. 16 Mature cytotoxic T cells and naïve T cells can also produce IL-2.17–19 Th17 cells mainly secrete IL-17, whereas Th2 cells produce primarily IL-4.20,21 TFH cells principally secrete IL-4 to help B cells to mature into plasma cells and are essential to maintain homeostasis and antibody production. 22 The effect of vitamin D3 concentration on the levels of T cell-related cytokines in human milk remains unexplored.
We aimed at determining the concentration of vitamin D3 in breast milk and Th cell-related cytokines (IL-4, IL-17, IFN-γ, IL-2, and TNF-β) in human milk from mothers with a confirmed COVID-19 polymerase chain reaction (PCR) test, mothers with viral symptoms, and mothers without infection. Our hypothesis was that milk from mothers with COVID-19 infection has lower vitamin D3 and higher Th cytokine levels than milk from mothers without infection.
Materials and Methods
Study design and participants
A screening survey was completed to recruit 10 lactating women who had a confirmed COVID-19 PCR test. Participants were asked to report when they had a positive COVID-19 PCR test and their symptoms. The time of COVID-19 positivity was between March 2020 and August 2020 during postpartum. The screening also identified 10 donors with viral symptoms suggestive of COVID-19 and 20 donors without infection during the COVID-19 pandemic. Mothers with viral symptoms suggestive of COVID-19 reported when they were sick and what symptoms they experienced but did not have a COVID-19 PCR test. Milk collection (n = 40) was collected between July 2020 and March 2021 for the three groups. The inclusion criteria were living in the United States, passing blood tests (women were screened before donating human milk and were negative for tests for HIV, Human T-cell lymphotropic virus (HTLV), hepatitis B or C, and syphilis, but these tests for infectious diseases did not include COVID-19 PCR test), and completing a health questionnaire (including prenatal vitamin intake) and a survey related to COVID-19 (Supplementary Table S1). Written consent to use milk for research was obtained from all participants. Milk collection was approved by the institutional review board (IRB00012424) of Medolac Laboratories. Mothers who used nicotine or other narcotics were excluded. Our recent study demonstrated that mothers with positive COVID-19 PCR and mothers with viral symptoms suggestive of COVID-19 had higher titers of human milk antibodies (IgA, IgM, and IgG) specific to SARS-CoV-2 receptor-binding domain than control women (prepandemic 2018). 23 The severity of COVID-19 or viral infections was mild, and these lactating women and their babies did not have severe problems that require hospitalization. The sample size was selected based on our previous studies of sample sizes.23,24 Based on the results, the sample size of lactating mothers for measuring vitamin D3 and cytokines could be comparable to that for determining the antibodies specific to SARS-CoV-2 and proved to be adequately powered.
Human milk collection
Human milk samples were collected at home with clean electric breast pumps into sterile plastic containers and stored immediately at −20°C in deep freezers. Donors labeled their milk collection by date of pumping. Human milk samples were frozen and transported in insulated boxes to Medolac Laboratories, where they were kept frozen and stored at −80°C until the ELISA measurements.
Vitamin D3 concentration
Human milk samples (2 mL) were rapidly thawed and centrifuged at 1,301 g for 20 minutes at 4°C. After removing the fat layer with cotton swabs,25–27 vitamin D3 concentrations were determined in undiluted supernatant samples by using an ELISA kit (Antibody Pair for Vitamin D3, MBS2099669; MyBioSource, Inc., San Diego, CA) and carried out as described by the manufacturer. ELISAs were recorded with a microplate reader (SpectraMax iD5; Molecular Devices, Sunnyvale, CA).
T cell cytokine concentrations
Human milk samples (2 mL) were rapidly thawed and centrifuged at 1,301 g for 20 minutes at 4°C. The concentrations of human IL-4 (Human IL-4 Duo Set ELISA, DY204-05), human IL-17 (Human IL-17 DuoSet ELISA, DY317-05), human IFN-γ (Human IFN-gamma DuoSet ELISA, DY285B-05), human IL-2 (Human IL-2 DuoSet ELISA, DY202-05), and human TNF-β (Human Lymphotoxin-alpha/TNF-β DuoSet ELISA, DY211-05) were measured in the supernatant milk samples undiluted. ELISAs were carried out as described by the manufacturer (R&D Systems, Inc., Minneapolis, MN).
Antibodies specific to SARS-CoV-2 RBD
The area under the curve (AUC) of SIgA/IgA, SIgM/IgM, and IgG specific to RBD-SARS-CoV-2 was determined by using ELISAs as described in our recent studies.23,24 Antibody titers were determined in mothers with confirmed COVID-19 PCR and mothers with viral symptoms suggestive of COVID-19.
Statistical analyses
Kruskal–Wallis test followed by Dunn's multiple-comparisons test was used to compare the measurements between COVID-19 PCR, viral symptoms, and no-infection groups by using GraphPad Prism (version 9). Mann–Whitney test was used to compare women taking prenatal vitamin and women without prenatal vitamin. Tukey's multiple-comparisons test was used to determine the effect of prenatal vitamin intake in women with viral symptom and women without infection groups (COVID-19 group was not tested, as all women were taking prenatal vitamins). The effect of seasons for milk collection (July to August for Summer versus November to February for Winter) was also determined by using Mann–Whitney test. Linear regressions were determined between vitamin D3 or cytokines and the elapsed time from infection to the milk collection in COVID-19 PCR and viral symptoms groups. Linear regressions were determined between maternal age or lactation time and the measurements in milk from all mothers. Linear regressions were evaluated between T cell-related cytokines and vitamin D3 concentrations in milk from all donors. Linear regressions were evaluated between antibody titers and vitamin D3 concentrations in milk from mothers with confirmed COVID-19 or mothers with viral symptoms.
Results
Maternal factors in lactating women during COVID-19 pandemic
The maternal demographic details of the participant groups are presented in Table 1. Postpartum time, infant gender, and maternal age were comparable between COVID-19 PCR, viral symptoms, and no-infection groups. Women who were taking prenatal vitamins during breastfeeding were higher in COVID-19 PCR (100%) than in viral symptoms (60%) and no-infection groups (70%). Mothers who had influenza vaccine were lower in COVID-19 PCR (20%) groups than in viral symptoms (70%) and no-infection groups (65%).
Demographic Description (Self-Reported) of Mothers with a Confirmed COVID-19 Polymerase Chain Reaction Test, Mothers with Viral Symptoms Suggestive of COVID-19, and Mothers Without Infection
Milk collection was performed after the viral symptoms.
Women were diagnosed with COVID-19 PCR test with a nasal swab (positive RNA SARS-CoV-2).
Symptoms reported by COVID-19 PCR groups were headaches, loss of taste and smell, fatigue, fever, nasal congestion, cough, severe upper respiratory infection, and body aches. Milk collection was performed after COVID-19 infection.
Symptoms reported by mothers with viral symptom suggestive of COVID-19 were headaches, fever, cough, nasal congestion, sore throat, mild runny nose, productive cough, laryngitis, rhinorrhea, body aches, and chills.
Data are mean ± SD, min, and max.
COVID-19, coronavirus disease 2019; NA, not applicable; PCR, polymerase chain reaction; SARS-CoV-2, severe acute syndrome coronavirus 2.
Between 50% and 60% of milk samples were collected during winter in the three groups. The elapsed time from the infection (SARS-CoV-2 or other viruses) was comparable between COVID-19 PCR and viral symptoms groups. The incidence of COVID-19 in lactating mothers [No. of women with +COVID-19 PCR test (n = 10)]/[No. of women in the population of our screening survey (n = 200)] was 5%.
Lower vitamin D3 levels in human milk from mothers with COVID-19
To determine the effect of vitamin D3 in human milk on the incidence of COVID-19 in lactating mothers, we measured the concentration of vitamin D3 in human milk. Vitamin D3 concentration in human milk was 2.8- and 3.4-fold higher in women without infection than in women with viral symptoms (p = 0.002) and COVID-19 PCR groups, respectively (p = 0.016, Fig. 1a), but it did not differ between viral symptoms and COVID-19 PCR (p > 0.99). The vitamin D3 was comparable between mothers taking prenatal vitamins and those without prenatal vitamins (p = 0.58, Fig. 2a). When comparing mothers with and without prenatal vitamins, vitamin D3 was lower in the viral symptoms group than in mothers with no infection (p = 0.004, Fig. 2b). Still, prenatal vitamin did not affect vitamin D3 in each separated group. The vitamin D3 in milk collected during summer (July–August) was 1.8-fold higher than in milk collected during winter (November–February) in all mothers (p = 0.024, Fig. 2c).
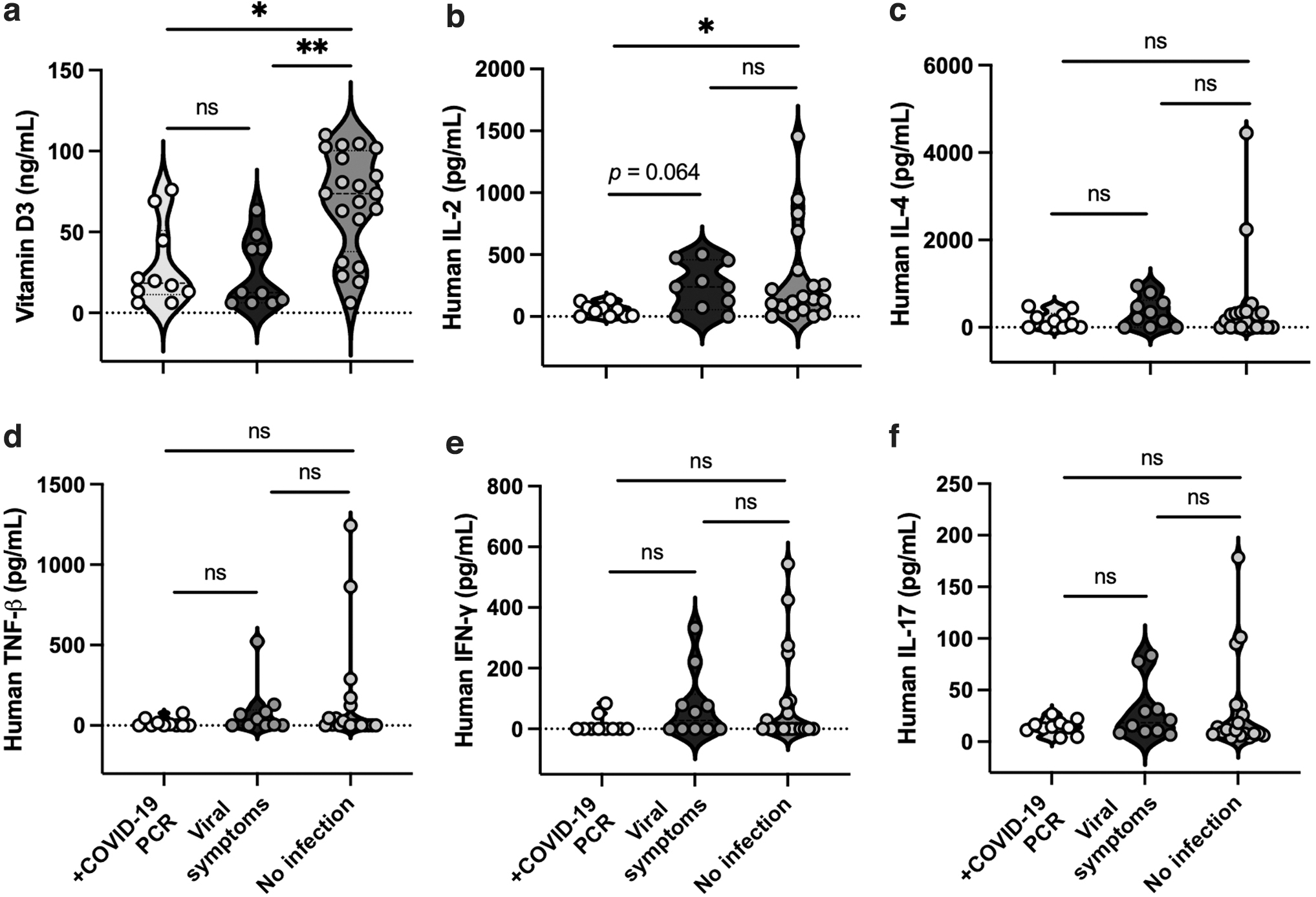
Effect of COVID-19 infections on the concentrations of vitamin D3 and T cell-related cytokines in human milk. Concentrations of
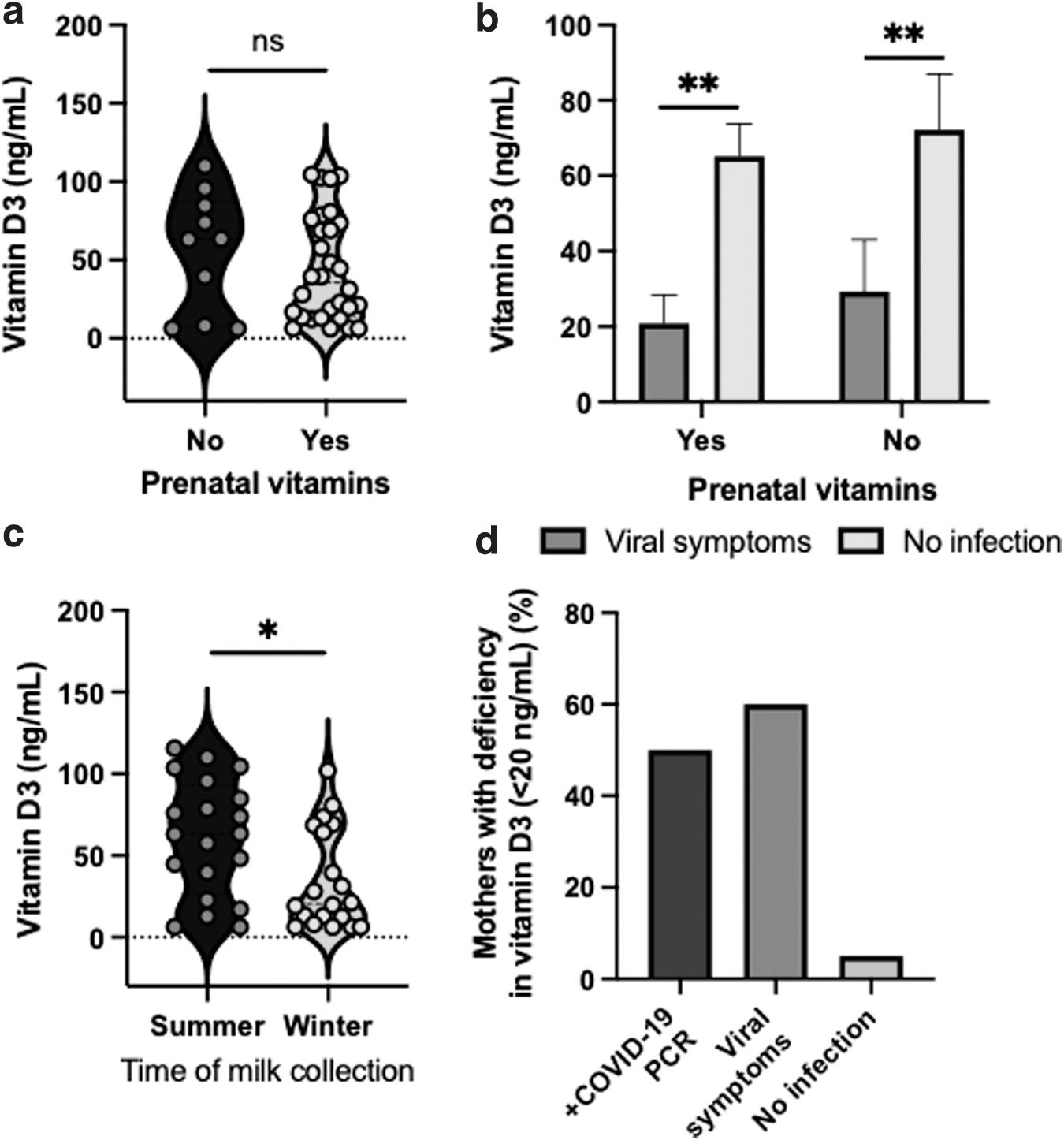
Effect of prenatal vitamin intake, season of milk collection, and viral infection on the vitamin D3 concentrations in human milk.
To determine whether vitamin D3 is influenced by the elapsed time from the infection (COVID-19 PCR group) or viral symptoms group, linear regressions were used between these measurements in the two groups of lactating women with different elapsed times. Vitamin D3 was not affected by the elapsed time from infection to milk collection in mothers with viral symptoms (p = 0.29) and with a confirmed COVID-19 PCR (p = 0.19). The postpartum time (p = 0.14) and maternal age (p = 0.90) did not correlate with vitamin D3 in milk from all mothers. Vitamin D3 did not correlate with any cytokines in human milk. The infant gender did not affect the vitamin D3 (p = 0.12).
Deficiency in vitamin D3 (<20 ng/mL) in milk was higher in the COVID-19 PCR (50%) and viral symptoms (60%) groups than in milk from mothers without infection (5%) (Fig. 2d).
Effect of COVID-19 infection on the levels of T cell-related cytokines in human milk
To determine whether T cell-related cytokines are influenced by COVID-19 infection, we determined the concentration of IL-2, IL-4, TNF-β, IFN-γ, and IL-7 in human milk. Human IL-2 level in human milk was higher in mothers without infection than in mothers with a confirmed COVID-19 PCR (p = 0.038, Fig. 1b), but it did not differ between the viral symptoms and no-infection groups. Human IL-2 level tended to be lower in the COVID-19 PCR group than in the viral symptoms group (p = 0.064, Fig. 1b). Human IL-4, TNF-β, IFN-γ, and IL-7 were comparable between COVID-19 PCR, viral symptoms, and no-infection groups (Fig. 1c–f). The human IL-2, IL-4, and IL-17 levels decreased with increasing elapsed time from infection to milk collection in mothers with viral symptoms (p < 0.05, Fig. 3a–c), but no correlation was observed in the COVID-19 PCR group. The human TNF-β level tended to decrease with increasing elapsed time from viral symptoms (Fig. 3d) or COVID-19 PCR test (Fig. 3e) to milk collection in both groups. Postpartum time and maternal age did not correlate with the concentrations of T cell cytokines in human milk. The infant gender did not affect the T cell-related cytokines.
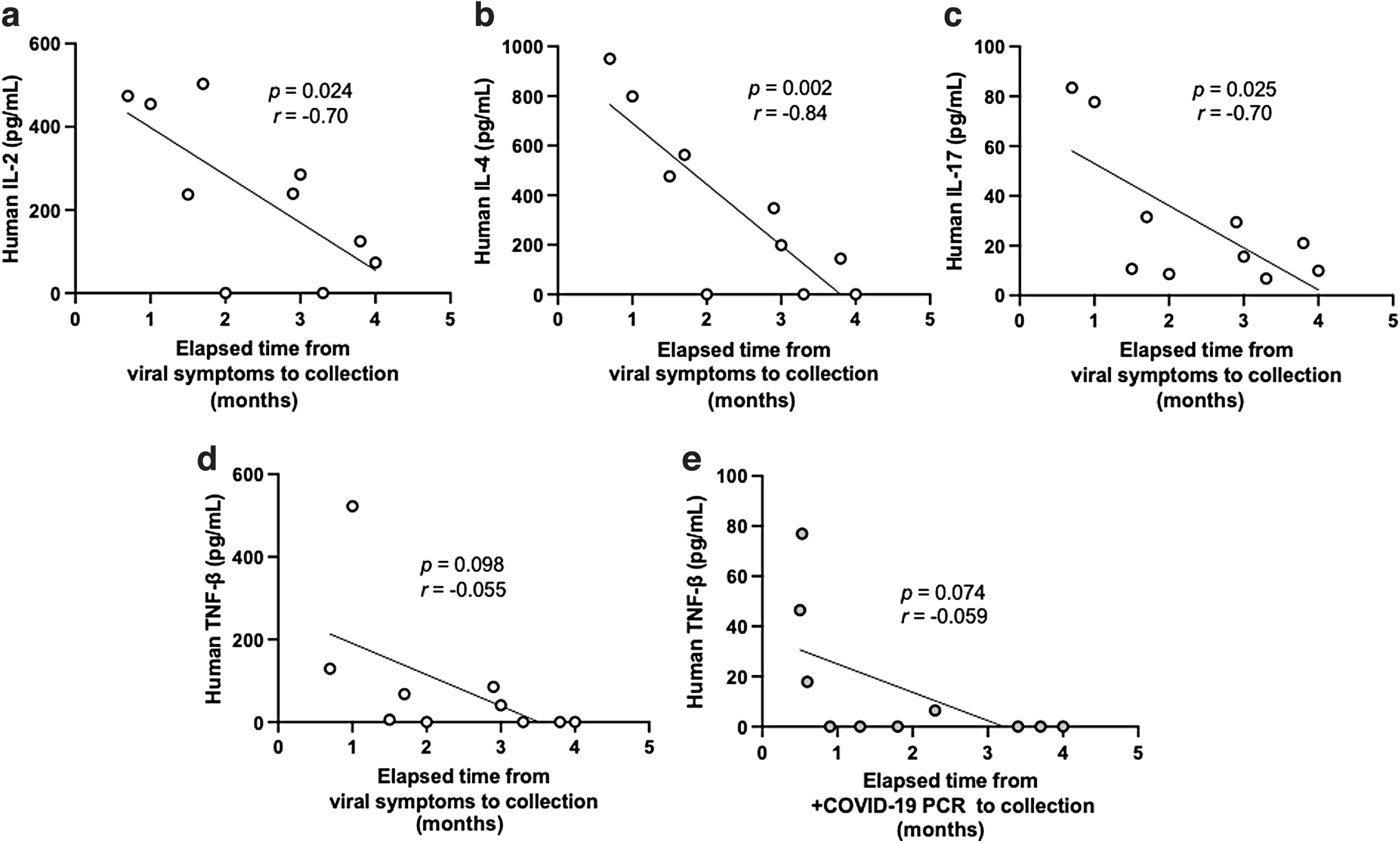
Linear regression analysis between the concentrations of T cell-related cytokines and the elapsed time from infection to milk collection. Concentrations of
Human IL-2 level was positively correlated with IL-17 (Fig. 4a), IL-4 (Fig. 4b), and TNF-b (Fig. 4c) in human milk. Human IL-4 level was elevated with the increase of TNF-β (Fig. 4d) and IL-17 (Fig. 4e), whereas IL-17 was positively correlated with TNF-β (Fig. 4f).
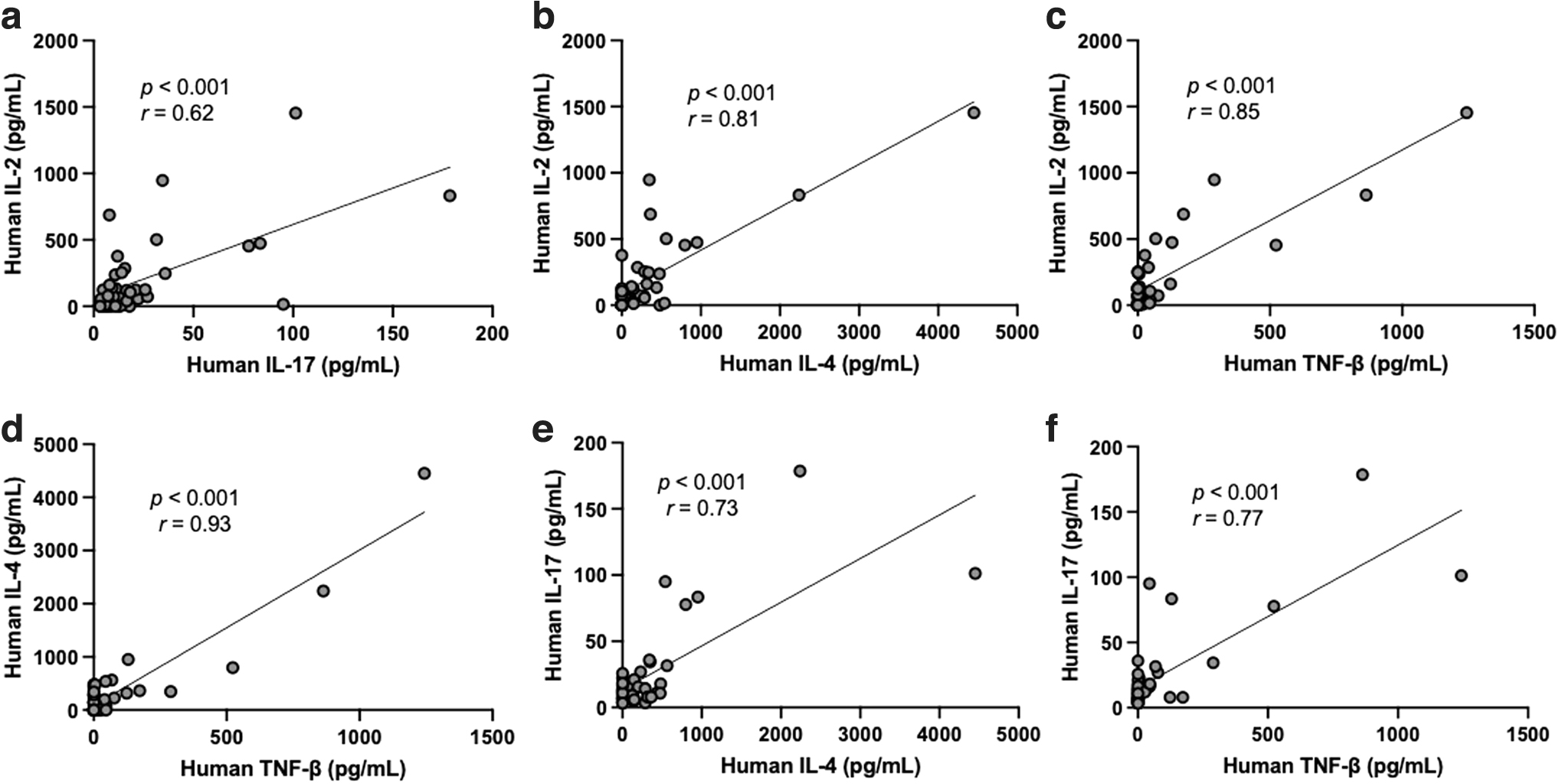
Linear regression analysis between the concentrations of T cell-related cytokines in human milk. Concentrations of
SARS-CoV-2-specific antibody titers and vitamin D3
No correlation was detected between antibodies (SIgA/IgA, SIgM/IgM, and IgG) specific to SARS-CoV-2 RBD and vitamin D3 concentrations in milk from mothers with a confirmed PCR or from mothers with viral symptoms (p > 0.10).
Discussion
Lactating women with adequate vitamin D in human milk are ingesting food with vitamin D, taking vitamin supplements, or getting body UVB exposure.12,28 Circulating vitamin D is transferred into human milk but circulating 25-hydroxyvitamin D does not.13,29 The parent compound cholecalciferol (vitamin D3) is the major vitamin D metabolite that crosses from maternal serum into human milk. 13 The active vitamin D3 [1,25(OH)D3] can bind to the vitamin D receptor, which potentially regulates the expression of genes involved in innate and adaptive immunity. 30 Whether vitamin D3 in human milk influences the incidence of maternal COVID-19 infection remains unknown.
For the first time, we demonstrated that vitamin D3 concentrations in human milk were higher in mothers without infection than in mothers with a confirmed COVID-19 PCR test and mothers with previous viral infections. This result suggests that a lower level in mother's milk, which reflects a lower vitamin D level in maternal blood, may increase the risk of COVID-19 and viral infections in lactating mothers. No previous study has examined the effect of vitamin D in human milk on the incidence of COVID-19 infection. A retrospective cohort study reported that deficient vitamin D status was associated with increased COVID-19 risk. 6 Martineau et al. 7 also found that vitamin D supplementation (daily or weekly) protected against acute respiratory tract infection, including coronaviruses. This protective effect was more pronounced in individuals with vitamin D deficiency, although those with higher baseline 25-hydroxyvitamin D concentrations also benefited. These authors speculated that vitamin D might support the immune responses to respiratory pathogens. 7 A randomized and double-blind intervention study reported that supplementation with vitamin D3 might reduce infectious symptoms among patients with antibody deficiency or frequent respiratory infections. 9
The vitamin D3 concentration of 8 ng/mL in human milk corresponds to 320 IU/L (1 μg = 40 IU) and ∼400 IU/L in infant formula. 13 These authors reported that the average of human milk vitamin D3 was 5–60 ng/mL in vitamin D supplemented mothers across 28 days. We found that the average of vitamin D3 in human milk from all 40 mothers was 48 ng/mL. The antirachitic activity of human milk is mainly influenced by the vitamin D3 concentration and minimally influenced by 25-hydroxyvitamin D, 13 as previous studies observed that 25-hydroxyvitamin D concentration was below 1 ng/mL.31,32 Approximately 20% of maternal vitamin D is transferred from mother's milk to the infant. 33 A concentration >30 ng/mL of total circulating 25-hydroxyvitamin D in maternal serum is considered adequate, whereas <20 ng/mL is considered deficient.34,35 Vitamin deficiency was also defined by the serum 25-hydroxyvitamin D3 < 20 ng/mL or 1,25-dihydroxyvitamin D3 < 18 ng/mL before testing COVID-19. 6 In this study, the percentage of milk from mothers with <20 ng/mL of vitamin D3 was 50% in COVID-19 PCR test, 60% in viral symptoms, and 5% in the no-infection groups. Vitamin D3 deficiency was higher in the COVID-19 PCR and viral symptoms groups than in the no-infection group. Mothers with Vitamin D deficiency are more likely to have infants with vitamin D deficiency.12,13 Whether infants deficient in vitamin D3 are less protected against viral infections than infants with adequate vitamin D3 remains to be investigated.
Human IL-2 level in human milk was higher in the no-infection group than in the COVID-19 PCR group. IL-2 tended to be higher in mothers with previous viral symptoms than COVID-19-recovered mothers. IL-2 is the major inducer of Th1 cells and is essential for mediating anti-viral defense and adaptive immunity.36,37 CD4+ and CD8+ cells released IL-2, IL-4, and IFN-γ during the mice's influenza-immune response. 38 Our results suggest that human milk IL-2 level was affected by the presence and type of maternal infection. Bryan et al. 39 also observed a similar range of IL-2 concentration in human milk. They speculated that the transfer of IL-2 from the mother's milk to the infants might stimulate T cells' growth and development and assist their deficit in this cytokine. More studies are needed to identify the role of IL-2 during neonatal development and the prevention of viral infection.
IL-2, IL-4, IL-17, and TNF-β levels decreased with increasing elapsed time from viral symptoms to milk collection. This observation could be due to the release of cytokines to the site of infection (respiratory mucosa). Cytokines that enter the circulation from infected mucosa are subject to massive dilution or rapid clearance. 40 Therefore, the lack of difference in IL-4, IL-17, IFN-γ, and TNF-β between infection and non-infection groups may be associated with the elapsed time between the infection and milk collection cytokines and may vanish after a few months of the immune response activation.
We observed that prenatal vitamin intake did not affect vitamin D3 concentration in human milk. Vitamin D supplementation is recommended to maintain a blood level of vitamin D above 30 ng/mL for lactating women and the pediatric population. 35 Prenatal vitamins generally contain 400 IU of vitamin D. Hollis and Wagner 12 reported that with limited sun exposure, an intake of 400 IU per day vitamin D would supply little vitamin D to nursing infants in human milk. Vitamin D intake regression model as 400 IU per day intake would increase maternal circulation by only 2.8 ng/mL after 5 months of supplementation. 41 Therefore, the prenatal vitamin intake of 400 IU did not increase the vitamin D3 concentration in human milk.
Vitamin D3 in human milk collected in summer (July–August) was higher than in milk collected in winter (November–February). This result is in accordance with Oberhelman et al., 13 who found that baseline serum vitamin D3 and 25-hydroxyvitamin D were 2.5- and 1.1-fold greater in mothers enrolled in April to July than those enrolled in January to March. Vitamin D produced after skin exposure to UVB sunlight provides ∼90% of vitamin D in nonsupplemented populations and is influenced by season, time of day, skin pigmentation, sunscreen use, and age. 42 Maternal age did not affect the vitamin D concentration in human milk, likely due to the small range (from 23 to 40 years old). Oberhelman et al. 13 also observed no correlation between baseline 25-hydroxyvitamin D concentrations and maternal age.
A limitation of this study is the unavailable information on the ethnic of the mothers (Caucasian, African American, or Hispanic) who donated their milk. The vitamin D2 was not determined in this study, as vitamin D2 is inferior to vitamin D3 at maintaining circulating 25(OH)D levels in humans. 43 We did not differentiate the concentration of 1,25(OH)2D3 and 25(OH)D3 in human milk but only total vitamin D3. Another limitation was the small sample size for this study. A larger cohort is needed to establish a positive correlation between vitamin D3 levels and reduction of COVID-19 infection. Moreover, vitamin D3 was not measured in different samples from the same mothers across times (pre-infection or +COVID-PCR test, peri-infection, and post-infection). We did not have milk samples from mothers who had donated milk without COVID-19 who later developed symptoms or +PCR test. However, these types of milk samples should be collected for future investigations.
Conclusion
These findings are potentially significant and support that adequate vitamin D3 level in human milk may influence COVID-19 infection in lactating women. However, a larger study is needed to confirm the relationship between human milk vitamin D3 and the reduction of incidence of COVID-19 disease. Adequate vitamin D3 status in breastfeeding women could provide a novel strategy to decrease the risk of SARS-CoV-2 infection. Whether adequate level of milk vitamin D3 enhances the immunity of breastfed neonates against COVID-19 remains to be investigated.
Footnotes
Authors' Contributions
V.D.M. conceptualized and designed the study, carried out the statistical analysis, drafted the article, and approved the final article as submitted. V.D.M. has primary responsibility for the final content. V.D.M. and S.L. carried out ELISA analyses. E.M. provided funding. S.L. and E.M. critically revised the article and approved the final article as submitted.
Acknowledgments
The authors thank all the study participants for their valuable contributions.
Disclosure Statement
V.D.M., S.L., and E.M. are employees at Medolac Laboratories A Public Benefit Corporation.
Funding Information
The authors (V.D.M., S.L., and E.M.) disclosed receipt of the financial support from Medolac Laboratories A Public Benefit Corporation for the conduct of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.