
Abstract
Background:
Oral application of mother's own milk (MOM) in very low birth weight (VLBW) neonates may provide an effective method of cleaning the oral cavity and influencing the immunocompetent cells there.
Methods:
A double-blind randomized controlled trial was conducted in a tertiary level neonatal unit on VLBW neonates; that is, neonates with birth weight <1,500 g, hospitalized within 72 hours of birth. The intervention was oral care with MOM. The primary objective was to observe the effect of oral care with MOM on late onset sepsis (LOS) and also on mortality, days to attain full enteral feed, necrotizing enterocolitis (NEC), exclusive breastfeeding rates at discharge, and total hospital stay (THS).
Results:
One hundred ten neonates were randomized to intervention and no-intervention group; 55 in each group. Neonates in the intervention group developed LOS in 9.1% versus 27.3% in no-intervention group (p = 0.013). Mortality was 9.1% versus 16.4% (p = 0.252); days to attain full enteral feeds were 6.94 ± 2.34 versus7.4 ± 2.31 days (p = 0.306); exclusive BF rates at discharge were 83% versus 75% (p = 0.449); THS was 30.72 ± 8.72 versus 33.5 ± 8.7 days (p = 0.267) in the two groups, respectively. There was no effect on NEC.
Conclusion:
Oral care of VLBW neonates with MOM reduces LOS and mortality.
Introduction
Sepsis is the second most frequent cause of death in neonates. 1 Approximately 25% of the neonates admitted to our neonatal unit are very low birth weight (VLBW), and they account for 25% of total deaths, with sepsis as a significant offender. Late onset sepsis (LOS), that is, sepsis developing after 72 hours of birth, is common in neonatal units, and research regarding preventive strategies is rampant. The oral cavity harbors potentially pathogenic bacteria that can cause systemic infection. 2 Oral care of sick and ventilated adults in the intensive care units with chlorhexidine decreases the incidence of invasive infection; however due to safety issues with chlorhexidine, this cannot be replicated in VLBW neonates.3,4 The oral cavity has a mucosal immune system comprising immunocompetent cells. Saliva is known to have antimicrobial proteins and peptides (APPs) that destroy bacteria and enhance mucosal immune system. It is stipulated that mother's own milk (MOM) also has APPs, which further stimulate neonatal APP production. 5 Secretory immunoglobulin A in MOM inhibits adhesion of bacteria to respiratory and gut mucosa. 6 In addition, MOM contains oligosaccharides that inhibit adhesion of bacteria to the surface receptors in the oral mucosa and cytokines, which may synergistically stimulate immune competent cells in the oral cavity and gut.7–9 When neonates are not fed orally, only the gut is exposed to MOM. Therefore, oral care using MOM may complement the benefits of breast milk feedings delivered through a feeding tube. Rodriguez et al. 10 described the theoretical immunological perspectives of oral care with colostrum in extremely low birth weight (ELBW) neonates and in a pilot study in 2010 determining its safety and feasibility. 5 Using MOM for oral care in neonates is an attractive option to reduce morbidity and mortality. It is also possible that oral care using MOM is a step in the transition to achieving breastfeeding success in infants with complex surgical anomalies. 11 Previous research regarding MOM oral care has shown mixed results and is limited by small sample sizes, inclusion of only ELBW neonates, that is, neonates with birth weight <1,000 g, and limiting oral care for the first few days after delivery. Therefore, we have planned a randomized controlled trial to determine the effect of MOM oral care, continuing up to the time the neonates are fed orally, on the incidence of LOS and also mortality, days to attain full enteral feeds, necrotizing enterocolitis (NEC), exclusive breastfeeding rates at discharge, and total hospital stay (THS).
Methods
This was a prospective, double-blind, parallel randomized controlled trial conducted in level III NICU on preterm VLBW neonates admitted within 72 hours of birth. Informed consent was obtained from either of the parents, and ethical approval was obtained from institutional ethics committee. The neonates for whom MOM was not available, in whom there was contraindication to feeding MOM, who were anticipated to be discharged within 14 days of enrollment, who had prior exposure of oral cavity to MOM, with major congenital anomaly, and whose parents did not give consent were excluded for the study. The primary objective of the study was to find the effect of oral care with MOM on LOS. Secondary objectives were to observe the effect on mortality, days to attain full enteral feed, NEC, exclusive breastfeeding rates, and THS.
The trial was registered in Clinical Trial Registry in India (Registration no. CTRI/2018/01/01326. Assessment of eligibility was performed by the Senior Resident on duty, and randomization was done by the senior nurse on duty. Enrolled neonates were randomized into two groups using computer-generated random numbers. Group A was intervention group who received oral care with MOM, and group B was no-intervention group who received a sham procedure for oral care. Allocation concealment was performed by sequentially numbered opaque sealed envelopes created by the statistician. The senior nurse in the unit was responsible for opening the envelopes for group assignment.
Both parents and investigators were blinded to group assignment. To administer the intervention, the nurse placed a screen around the infant's bed, and administered either oral application of MOM or a sham procedure using an empty syringe and no swabbing.
Baseline demographics including birth weight, sex, gestational age, type of delivery, place of delivery, birth asphyxia (APGAR SCORE <6 at 5 minutes), diagnosis on admission, history of antenatal steroids, and maternal antibiotic use were collected from the medical records. Neonates were managed according to the unit protocols.
Oral care procedure
For neonates in group A, oral care was performed aseptically by the senior nurse on duty by instilling 0.1 mL of MOM (0.05 mL on each side) followed by swabbing with sterile ear bud. For group B, a sham procedure of the oral cavity using an empty syringe and no swabbing was performed. The procedure was repeated every 8 hours until the infant began taking MOM by spoon/breast. Adverse effects of the procedure were noted. Neonates in both groups were fed according to standard guidelines for feeding VLBW neonates (starting fluids at 80 mL/kg/day for neonates with birth weights of <1,500 g with usual daily increment of 15–20 mL/kg/day, so that by the end of first week 150 mL/kg/day is reached). During hospitalization, all neonates were monitored for the clinical signs suggestive of sepsis, followed by relevant investigations, including sepsis screen, blood culture, lumbar puncture, chest radiograph as indicated.
Primary outcome
Occurrence of LOS among both the groups.
The National Neonatal Perinatal Database, 2002–2003 definitions were used to define sepsis, meningitis, and pneumonia as mentioned in Appendix Table A1. 12
Secondary outcome
Mortality rate, days to attain full enteral feed, NEC, exclusive breastfeeding rates at discharge, and THS were compared between the two groups.
Sample size
The sample size was calculated using the following formula:
13
where c = 7.9 for 80% power, P1 and P2 are the proportion estimates. Thus for this study, considering P1 = 0.25 and P2 = 0.5 (19) for an 80% power, and 5% two sided level of significance, sample size per group was 55. Hence, 55 subjects were required to be enrolled in each group. Expecting a dropout rate of 30–40%, 84 neonates were enrolled in each group.
Statistical analysis
For the statistical analysis, SPSS 16.0 software was used. Quantitative variables were compared using unpaired t-test/Mann–Whitney U test (for continuous variables). Qualitative variables were compared using chi-square test/Fisher's exact test as appropriate. Neonates who died or left the study within 14 days of enrollment were not included in the analysis. Per protocol analysis was done.
Results
As shown in Figure 1, during the study period, 2,298 neonates were admitted to NICU, of which 489 were VLBW. The first 258 were consecutively assessed for eligibility. Ninety neonates were excluded (neonates for whom MOM was not available [33], contraindication to feeding MOM [7], prior exposure of oral cavity to MOM [25], with major congenital anomaly [5], and whose parents did not give consent [20]). Finally, 168 neonates were enrolled and randomized to one of the two groups with 84 in each group. There were 58 dropouts (30 left against medical advice, 17 expired within 14 days of enrollment, and 11 parents withdrew their neonates before study completion). So both groups comprised of 55 neonates who completed the study.
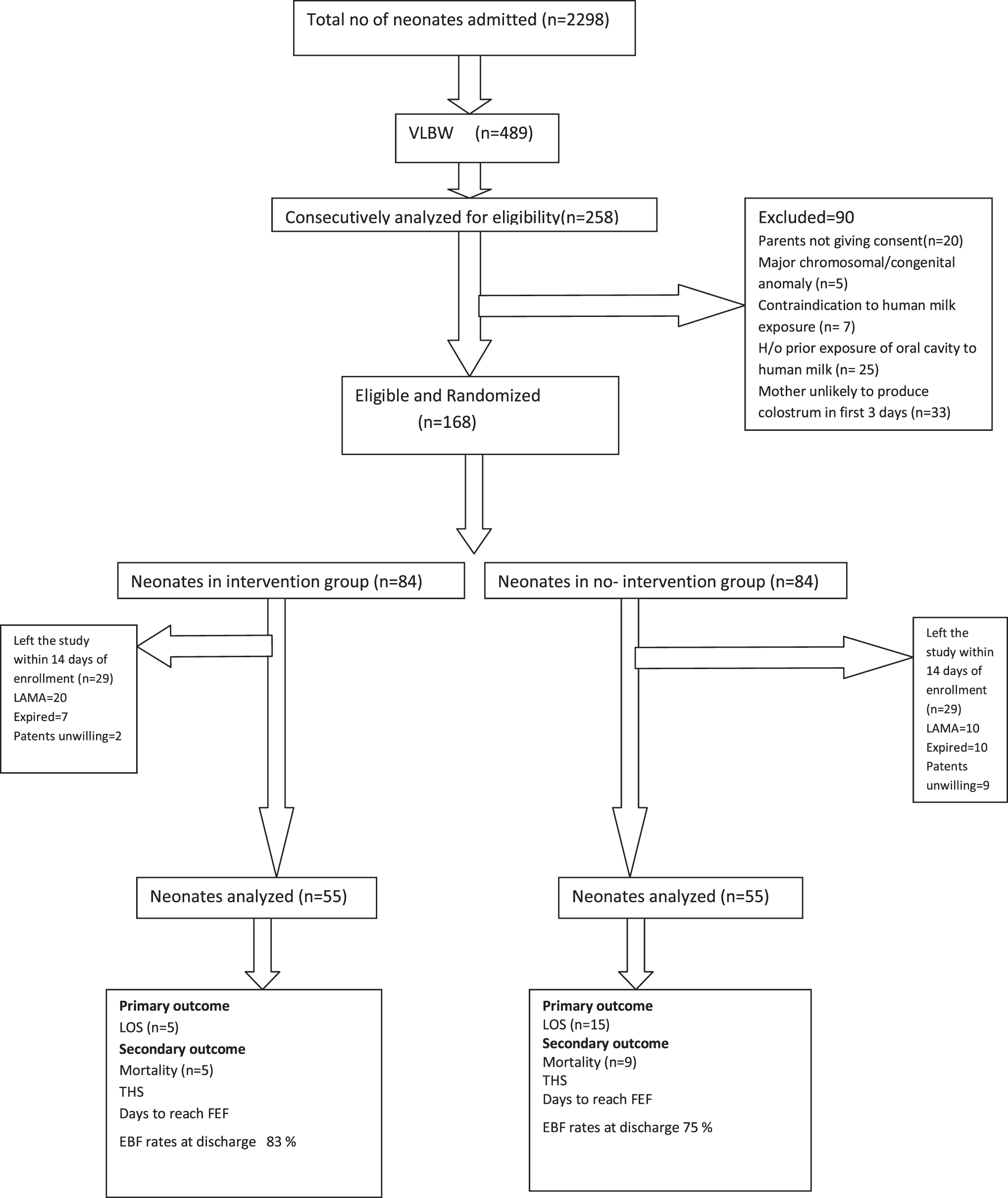
Flow diagram of the study.
Table 1 displays the baseline characteristics of enrolled neonates, which were similar between two groups. The mean number of days the intervention was administered was 7.91 ± 3.03 days. There were no adverse events during the procedure except for transient hypoxia in one neonate.
Baseline Characteristics of Study Neonates
AGA, appropriate for gestational age; EOS, early onset sepsis; LSCS, lower segment cesarean section; MAS, meconium aspiration syndrome; NVD, normal vaginal delivery; RDS, respiratory distress syndrome; SGA, small for gestational age.
Table 2 shows the incidence of sepsis and mortality, days to attain full enteral feeds, NEC, exclusive breastfeeding rates at discharge, and THS among the two groups.
Outcome Measures Among the Neonates of the Two Groups
The bold represents statistical significance.
EBF, exclusive breastfeeding rates; FEF, full enteral feeds; LOS, late onset sepsis; NEC, necrotizing enterocolitis; THS, total hospital stay.
Discussion
In our study, the overall incidence of LOS was 18.2%. The incidence of clinical LOS in intervention group was significantly lower than that found in no-intervention group. We also found less culture proven sepsis in the intervention group. This difference can possibly be attributed to the numerous APPs, oligosaccharides, and cytokines present in MOM, which may decrease infection by modulating mucosal and systemic inflammatory responses. These results are similar to those of Lee et al. 14 who found oral care with colostrum group was associated with less clinical sepsis, but there was no difference in culture proven sepsis. On the contrary, some researchers found no statistically significant decrease in the incidence of sepsis in neonates who received oral colostrum priming.15–17 Some studies have reported inconclusive results. 18 The Cochrane review published in 2018 found no difference in sepsis, NEC, and other morbidities by oropharyngeal colostrum (OCP), and stated that more randomized controlled trial (RCTs) are needed in this field. 19
In our study the duration of THS was lesser in intervention group versus no-intervention group. Although this was statistically not significant. This was also reported in other studies where intervention group had significantly shorter THS.18,19 In our study the overall incidence of NEC was 1.8%. There was no difference in incidence of NEC in two groups. This incidence was low because the sickest of preterm babies may not have lived beyond 14 days after being randomized (therefore excluded) or may not have been a part of the study due to non-availability of MOM. This was in line with other studies.15,16,20 However Lee et al. found that the colostrum group had lesser incidence of NEC (Bell stage 2) 25% versus 17%, though not statistically significant (p = 0.72). 14
In our study, mortality was almost half in intervention group 9.1% versus no-intervention group 16.4% (p = 0.252). This was expected although all baseline characteristics and the morbidity profiles of neonates in both the groups were similar; LOS was significantly less in intervention group. This was in line with some research studies.14,17
We found that full enteral feeds were attained earlier in the intervention group, but the difference was not significant. This was similar to the observation of some studies.14-,15,20 On the contrary, Abd-Elgawad et al. found that the intervention group reached full feeds significantly earlier.
In our study, there was no significant difference in THS in the two groups. This was unlike some studies where a significant reduction by 16 days in the median length of hospitalization was found in the intervention group. 16 Lee et al. 14 and Seigel 20 et al. did not find a statistically significant difference in the length of stay but did report some interesting trends from which our study differed in the frequency and duration (8 vs. 5 hourly and 8 vs. 5 days) of oral care protocol. Recently, Abd-Elgawad et al. too found the intervention group to have a shorter THS. 17
Exclusive breastfeeding rate at discharge was more in intervention group (83% vs. 75%), but the difference was not significant (p = 0.449) in our study. The reason for this is unclear as in both the groups the mothers were blinded and equally motivated. Unlike our study, Synder et al. found that there was a significant association between OCP application and receiving breast milk as the majority of feed at 6 weeks of age. 15
None of the babies in our study, not even the most premature and ELBW, developed any problem during the procedure of application of MOM in the oral cavity except transient hypoxemia. Our findings are similar to many other studies.5,15,20,21
The strengths of our study are that it is a double-blind RCT with a robust methodology. We included VLBW late preterm neonates too, which make up a substantial part of VLBW babies in developing countries like ours. Other researchers have worked primarily on <28–32 week gestation neonates. Since the no-intervention group also received sham oral care, those mothers were also enthusiastic to express milk for their neonates. Finally, the neonates were from a single center, thus limiting the treatment center variability.
The major weakness of our study is a dropout rate of 35%. This happened primarily because of neonates dying within 14 days of enrollment, leaving against medical advice due to financial constraints, or parents withdrawing from the study as mothers could not continue supplying MOM for oral care. Maybe the presence of dedicated lactation counselors could have helped us to bring down this dropout rate.
In conclusion, this RCT has shown that a simple and safe procedure like oral care with MOM reduced LOS by a third in VLBW premature neonates. It also decreased mortality and increased exclusive breastfeeding rates at discharge.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Appendix
Definition of Sepsis, Meningitis, and Pneumonia
| Septicemia (National Neonatal Perinatal Database, 2002–2003) 12 | (a) Culture negative (clinical/probable) sepsis: In an infant having clinical picture suggestive of septicemia, the presence of any one of the following criteria is sufficient to assign a probable diagnosis of infection: |
| • Positive septic screen (two of the four parameters: Total leukocyte count (<5,000/mm, band to total polymorph ratio of >0.2, absolute neutrophil count <1,800/cm, C-reactive protein >1 mg/dL and micro erythrocyte sedimentation ratio >10 mm first hour). | |
| • Radiological evidences of pneumonia. | |
| (b) Culture positive sepsis | |
| In an infant having symptoms suggestive of septicemia, pneumonia or meningitis along with either of the following. | |
| • Isolation of pathogens from blood, CSF, urine, or abscess(es) | |
| • Pathological evidence of sepsis on autopsy. | |
| Pneumonia (National Neonatal Perinatal Database, 2002–2003) 12 | In a neonate with respiratory distress, pneumonia is diagnosed in the presence of a positive blood culture or if any two of the following are present. |
| • Existing or predisposing factors: maternal fever, foul smelling liquor, prolonged rupture of membranes (>18 hours), or gastric polymorphs >5 per high power field. | |
| • Clinical picture of septicemia (poor feeding, lethargy, poor reflexes, hypo, hyperthermia, abdominal distension, etc.) | |
| • X-ray picture suggestive of pneumonia. | |
| • Positive sepsis screen | |
| Meningitis (National Neonatal Perinatal Database, 2002–2003) 12 | In the setting of septicemia, if a CSF culture is positive; or CSF microcopy and biochemistry are suggestive of meningitis. |
CSF, cerebrospinal fluid.