
Abstract
Background:
To ensure the safety of higher dose vitamin D supplementation in pregnant and lactating mothers, and urinary calcium/creatinine (UCa/Cr) ratios, serum calcium, and serum 25(OH)D concentrations are closely monitored. To achieve optimal maternal and infant vitamin D status, while avoiding hypercalcemia, safety measures assessing vitD supplementation must be reliable. Whether or not this holds true for infants before 7 months of age, remains unknown.
Objective:
Analyze the association among UCa/Cr ratio, serum calcium, intact serum parathyroid hormone (iPTH), 25(OH)D, and 25(OH)D/iPTH ratio in infants to determine whether evidence supports the use of these parameters as valuable measures of hypervitaminosis D or toxicity in infants.
Methods:
A series of analyses were performed on the cohort of infants who participated in the National Institute of Child Health and Human Development lactation vitD supplementation trial to determine the association among UCa/Cr ratio, serum calcium, iPTH, 25(OH)D, and 25(OH)D/iPTH ratio.
Results:
Upon multivariate analysis, serum calcium was significantly associated with 25(OH)D (p = 0.0441), iPTH (p = 0.0017), and 25(OH)D/iPTH ratio (p = 0.0001). Infant UCa/Cr did not associate with 25(OH)D but did associate with iPTH (p = 0.0008) and 25(OH)D/iPTH ratio (p = 0.0001). The correlation between UCa/Cr and 25(OH)D/iPTH ratios was significantly stronger than the association between UCa/Cr ratio and iPTH. Serum calcium more strongly correlated with 25(OH)D/iPTH ratio versus 25(OH)D and iPTH.
Conclusion:
In this healthy cohort of infants 1 to 7 months old, UCa/Cr and serum calcium are more valid indicators of 25(OH)D/iPTH ratio than either 25(OH)D or iPTH alone. Moreover, serum calcium (and not UCa/Cr) is a valid indicator of infant total circulating 25(OH)D and should be measured if vitamin D toxicity is a concern.
Clinical Trial Registration number: FDA IND Number: 66,346; ClinicalTrials.gov Number: NCT00412074.
Introduction
Vitamin D plays an essential role in calcium and phosphorus metabolism and bone mineralization when present in ample supply. During pregnancy, however, the role of vitamin D is particularly crucial because it maintains maternal calcium homeostasis and thus greatly affects fetal bone development. 1 There is increasing attention on vitamin D because of its role in pregnancy outcomes that carries over into lactation, immunity, and long-term health.1–3 The upsurge in the prevalence of vitamin D deficiency in pregnant and lactating women raises concerns about the health outcomes of infants with deficient vitamin D levels.1,3 Thus, there is a heightened focus on vitamin D supplementation in pregnant and lactating women to provide vitamin D sufficiency for both the mother and her infant.1,3,4
Historically, several laboratory parameters have been monitored to ensure the safety of higher dose vitamin D supplementation in pregnant and lactating mothers: urinary calcium/creatinine (UCa/Cr) ratios, serum calcium, intact serum parathyroid hormone (iPTH), and serum 25(OH)D. 5 Although reported in some trials, consistent normative and safety guidelines for young infants are unavailable.6,7
Calcium homeostasis in the human body depends on calcium absorption and excretion, which, in turn, depend on vitamin D status. Vitamin D acts in concert with intestinal epithelial cells as well as the distal nephron and bone matrix to increase calcium reabsorption. Higher blood concentrations of the parent compound vitamin D and its metabolites—25-hydroxyvitamin D and 1,25-dihydroxy-vitamin D—increase calcium reabsorption and lead to increased filtration of calcium by the kidneys. High serum calcium overwhelms the glomeruli causing excretion of excess calcium in the urine.8,9
Urinary calcium excretion is a measure of hypercalciuria that precedes hypercalcemia. 10 However, obtaining a 24-hour urine sample is difficult and is often nonrepresentative of urinary excretion of the solute of interest. 11 In older children, adolescents, and adults, creatinine excretion is relatively constant over a 24-hour period; thus, these levels serve as a reference value for calcium/creatinine ratios in random urine samples. 11 The calcium-to-creatinine concentration ratio in random urine samples is an accurate index of urinary calcium excretion in adults and older children.7,11 Consequently, the use of urinary calcium excretion in 24-hour samples has been superseded through measurements of UCa/Cr ratios in spot (random) urine samples. 6
Vitamin D supplementation beyond certain threshold doses increases serum calcium concentration and UCa/Cr ratios in adults. 12 As such, a measure of vitamin D status—total circulating25-hydroxyvitamin D—is associated with an established range of safety parameters, UCa/Cr ratios, and serum calcium concentrations in adults. However, these laboratory safety measures are highly variable in infants, especially those younger than 7 months of age.6,7 Not only does calcium excretion depend on vitamin D status, but it is also influenced by gestational and chronological age, race, renal function, dietary intake, genetic factors, and parathyroid hormone.7,13 These factors and immature renal development in infants younger than 7 months of age may account for the variability in laboratory safety measures.7,13
Safety measures in assessing vitamin D supplementation must be reliable to successfully achieve optimal maternal and infant vitamin D status while avoiding hypercalcemia; this has not been the case in infants younger than 7 months, where published studies have been plagued by smaller sample sizes and inconsistencies in methodology. By default, researchers generalize from the safety measures used in assessing vitamin D supplementation for adults and apply those measures to infants.
To address this deficit, this study analyzes the association among UCa/Cr ratio, serum calcium, iPTH, 25(OH)D, and 25(OH)D/iPTH ratio in infants to determine whether evidence supports the use of those parameters as valuable measures of hypervitaminosis D or toxicity in infants. To determine their usefulness as safety measures, the authors sought to identify the point in time from birth to 7 months when those parameters begin to associate with vitamin D status.
This study analyzed a cohort of infants who participated in the National Institute of Child Health and Human Development (NICHD) lactation vitamin D supplementation trial. 14 A series of analyses were performed to determine the association among vitamin D status, iPTH, 25(OH)D/iPTH ratio, serum calcium, and UCa/Cr ratio. The authors hypothesized that UCa/Cr ratios do not correlate with vitamin D status as measured by 25(OH)D until at least 7 months of age. Until this point, infant UCa/Cr ratios are variable. The authors further hypothesized that the UCa/Cr ratio and serum calcium would more strongly associate with iPTH and 25(OH)D/iPTH ratio versus with 25(OH)D alone. Lastly, a goal of this study was to identify those laboratory measures in infants—those breastfeeding or formula feeding—that would be best to assess potential vitamin D deficiency as well as toxicity and to provide the expected ranges for those measures during this period of infant development from birth to 7 months.
Materials and Methods
Retrospective analysis was performed on the NICHD dataset collected prospectively from November 2005 to August 2012 to compare the effectiveness of three doses of vitamin D supplementation in lactating and nonlactating (control) mothers and their infants. 14 The NICHD Lactation Vitamin D Supplementation Study was a randomized double blinded trial conducted at two study sites: the Medical University of South Carolina (MUSC) and the University of Rochester (U of R). Details about this clinical trial and results based on treatment group have been previously reported. 14 Exclusively breastfeeding and formula feeding mothers were randomized into one of three treatment groups: 400, 2,400, or 6,400 IU vitamin D3 per day.
There were no safety issues based on treatment group in either the mothers or their infants using safety parameters in place at the onset of the study. 5 Further evaluation of those safety parameters applied to the infants in the study is presented in this study.
Approval was granted by MUSC's Institutional Review Board for Human Subjects HR 16536 and Clinical and Translational Research Center (CTRC; Protocol 752) as well as by the U of R's Institutional Review Board (14460) and CTRC (Protocol 1129). This approval was registered through ClinicalTrials.govNCT00412074. Additional details of the study protocol are included in the Supplementary Appendix S1 and have previously been reported.
The interim analysis conducted by the Data Monitoring and Safety Committee in February 2009 indicated that the 2,400 IU treatment arm should be discontinued because a disproportionate number of infants were vitamin D deficient (<20 ng/mL) at the 4-month visit versus the 400 and 6,400 IU treatment arms. 14 Although fewer infants were included in the 2,400 IU arm compared with the 400 and 6,400 IU treatment arms, this post hoc analysis included all three treatment arms to display a wider range in vitamin D status that was more representative of the population.
Outcome measures
Maternal and infant serum calcium and creatinine concentrations were measured at baseline using standard methodology and laboratory normative data by Clinical Chemistry Laboratories at the MUSC and the University of Rochester. Cross-validation between these two laboratories was performed for 5% of the samples (interassay variation 5.4%).
Circulating 25(OH)D and vitamin D (parent compound) were measured in the MUSC laboratory of Dr. Bruce Hollis using high-performance liquid chromatography and radioimmunoassay techniques as previously described.15–18 The inter- and intraassay coefficient of variation was <10%. The 25(OH)D concentration was expressed in ng/mL.
Maternal and infant circulating intact PTH concentrations were measured in Dr. Hollis' laboratory using a commercially available immunoradiometric assay (IRMA, DiaSorin, Stillwater, MN) and expressed in pg/mL. 19
Infant total circulating 25(OH)D/iPTH ratio was derived and utilized to quantify functional vitamin D deficiency (FVDD) defined as serum 25(OH)D levels below 20 ng/mL and PTH serum levels above 65 pg/mL (or 0.308).
Statistical analyses
The primary outcome variables for this post hoc analysis were the safety measures for vitamin D toxicity: UCa/Cr ratio, and serum calcium. The independent variables were 25(OH)D, iPTH, and 25(OH)D/iPTH ratio.
Statistical analyses were performed using SAS software version 9.4 (SAS, Inc., Cary, NC). Descriptive statistics were used to characterize infant laboratories at baseline (V1), 4 months (V4), and 7 months (V7). Student's t test was used to compare laboratory values between breastfeeding groups; analysis of variance was used to test for differences in laboratory values among treatment groups and races. Regression analyses showed an association with the laboratory infant UCa/Cr ratio and serum calcium, iPTH, 25(OH)D, and 25(OH)D/iPTH ratio. Generalized linear mixed effect models were used to measure the relationship with infant UCa/Cr ratio and with serum calcium while controlling for race, breastfeeding, treatment, visit, 25(OH)D, iPTH, and 25(OH)D/iPTH ratio. Significance was set a priori as p < 0.05.
Results
A total of 564 mother/infant pairs were consented, of whom 419 mother/infant pairs were randomized into 400, 2,400, and 6,400 IU treatment arms. The number of infants sampled for each laboratory safety parameter by treatment group across all visits are shown in Figure 1. Maternal and infant sociodemographic and clinical characteristics at enrollment are summarized in Table 1.
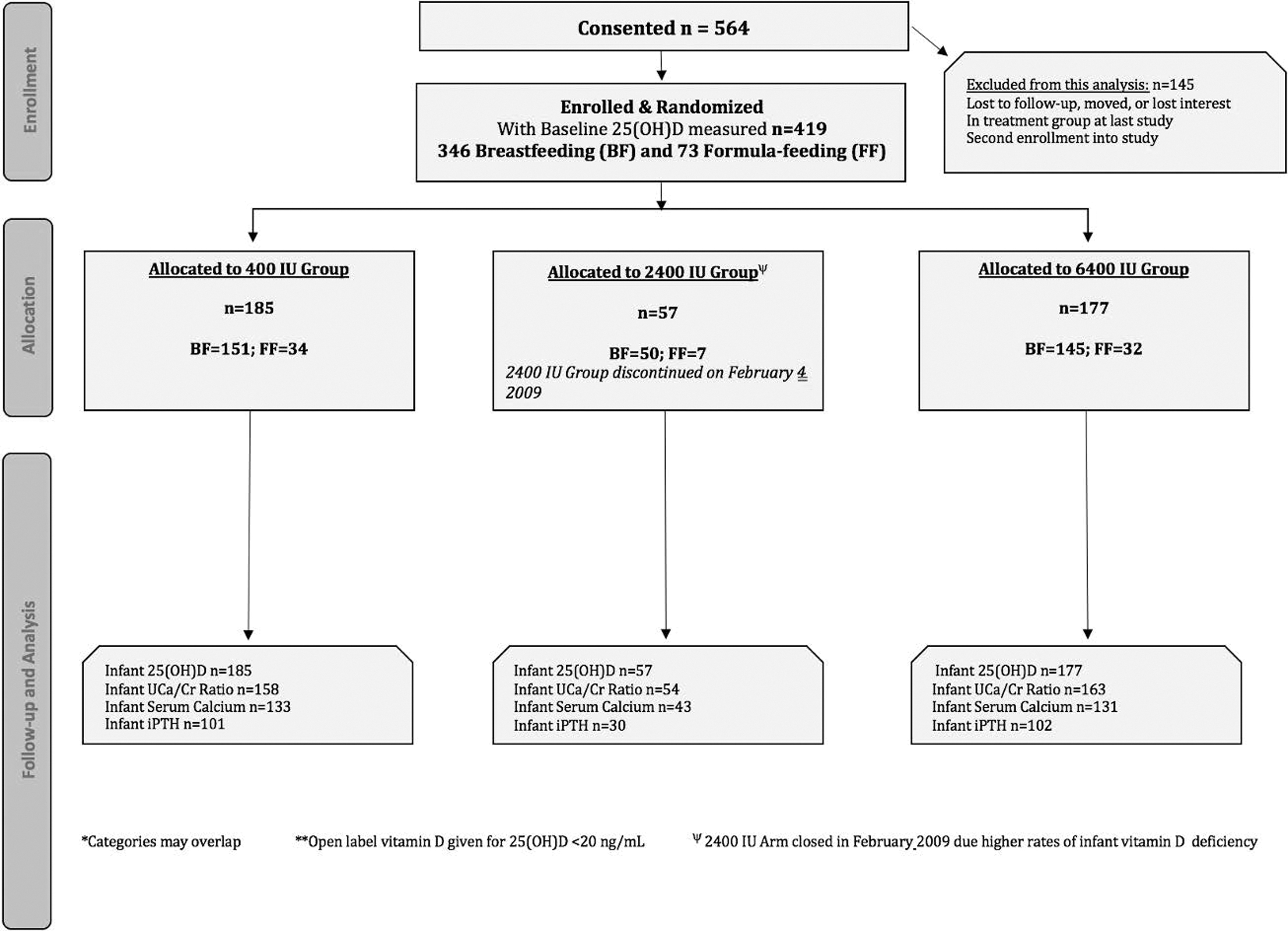
CONSORT flow diagram of study participants.
Maternal and Infant Sociographic and Clinical Characteristics at V1
IQR, interquartile range; NICHD, National Institute of Child Health and Human Development; SD, standard deviation.
The results of multiple linear regression analyses of the independent associations of infant 25(OH)D as well as iPTH with UCa/Cr ratio and serum calcium are summarized in Table 2. Serum calcium positively associated with 25(OH)D over time (β = 0.002276; p = 0.0441). Infant UCa/Cr (β = −0.00303; p = 0.0008) and serum calcium (β = −0.00344; p = 0.0017) negatively associated with iPTH over time. However, the association between UCa/Cr and 25(OH)D over time was not statistically significant.
Multiple Regression Analysis Model
The associations between infant 25(OH)D and iPTH (independent variables) and infant UCa/Cr and serum calcium (dependent variables).
iPTH, intact serum parathyroid hormone; UCa/Cr, urinary calcium/creatinine.
The results of multiple linear regression analysis of the association of infant 25(OH)D/iPTH ratio with infant UCa/Cr ratio and serum calcium are summarized in Table 3. Infant UCa/Cr ratio (β = 0.03991; p = 0.0001) and serum calcium (β = 0.04643; p = 0.0001) positively associated with 25(OH)D/iPTH ratio over time. The correlation between UCa/Cr and 25(OH)D/iPTH ratios (β = 0.03991) was significantly stronger than the association between UCa/Cr ratio and iPTH (β = −0.00303) when analyzed separately. Also, serum calcium more strongly and independently correlated with 25(OH)D/iPTH ratio (β = 0.04643) versus 25(OH)D (β = 0.002276) and iPTH (β = −0.00344), when analyzed separately.
Multiple Regression Analysis Model
The associations between infant 25(OH)D/iPTH (independent variable) and infant UCa/Cr and serum calcium (dependent variables).
Table 4 shows the linear correlations among infant total circulating 25(OH)D, iPTH, and the 25(OH)D/iPTH ratio and UCa/Cr ratio at V1, V4, and V7. Infant UCa/Cr ratio was not associated with 25(OH)D at any of the study visits. At all three visits, infant UCa/Cr negatively associated with iPTH and positively associated with 25(OH)D/iPTH ratio. Upon comparison of beta estimates, the correlation between infant UCa/Cr ratio and 25(OH)D/iPTH ratio was stronger than the correlation between UCa/Cr ratio and iPTH at all three visits.
Linear Regression Analysis Model
Linear associations among infant 25(OH)D, iPTH, and 25(OH)D/iPTH ratio and UCa/Cr at visit 1, 4, and 7.
Table 5 shows the linear correlations between infant total circulating 25(OH)D, iPTH, and the 25(OH)D/iPTH ratio and serum calcium at V1, V4, and V7. Infant serum calcium positively associated with 25(OH)D only at V7. At all three visits, infant serum calcium negatively associated with iPTH and positively associated with the 25(OH)D/iPTH ratio. A comparison of beta estimates revealed that the association between infant serum calcium and 25(OH)D/iPTH was stronger than the independent associations between serum calcium and both 25(OH)D and iPTH at all three study visits. Moreover, an inverse association emerged between infant total circulating 25(OH)D and iPTH; the association was statistically significant at all three visits (data not shown).
Linear Regression Analysis Model
Linear associations between infant 25(OH)D, iPTH, and 25(OH)D/iPTH ratio and serum calcium at visit 1, 4, and 7.
Discussion
In this post hoc analysis of the NICHD Lactation Vitamin D Supplementation Trial cohort, infant serum calcium was not associated with 25(OH)D at the 1- or 4-month visit, but a positive association occurred at the 7-month visit. Upon controlling for potential confounders, serum calcium positively associated with 25(OH)D over time, as the authors expected according to the canonical scheme of vitamin D function. 20
Over the course of this study, both maternal and infant vitamin D supplementation associated with increased but equivalent infant serum 25(OH)D in the treatment groups, allowing for optimal conversion to the more active form [1,25(OH)2D], which is known to increase infant serum calcium and phosphorus absorption in the intestines and increase urinary calcium reabsorption, thus increasing serum calcium. 3 Based on this finding, vitamin D toxicity would be expected to elicit an excessive increase in serum calcium, thus prompting the kidneys to excrete more calcium in the urine. 21 This concept is the premise for using the UCa/Cr ratio as a safety measure of vitamin D toxicity in infancy, the reliability of which, until this post hoc analysis, remained uncertain.
In an effort to achieve adequate serum 25(OH)D values (>20 ng/mL), current guidelines recommend a daily intake of 400 IU/day for all infants within the first few days of life. 22 Routine monitoring of serum 25(OH)D in healthy infants is not currently recommended. Clinicians should consider monitoring serum 25(OH)D in infants at risk for vitamin D deficiency as outlined by the American Academy of Pediatrics (AAP). 23 Additionally, the AAP recommends monitoring serum calcium, iPTH, and urinary calcium creatinine ratio upon treatment of rickets and hypocalcemia with high-dose vitamin D and calcium supplementation. 23
Our findings suggest that practitioners monitoring vitamin D status should not rely on UCa/Cr ratio as a safety parameter. Clinicians should be aware that there is no association between UCa/Cr ratio and serum 25(OH)D from birth to 7 months. The traditional use of UCa/Cr ratio should be replaced with monitoring of serum calcium in conjunction with 25(OH)D/iPTH ratio as these safety parameters are stronger indicators of infant calcium homeostasis.
Infant total circulating 25(OH)D/iPTH ratio was derived and utilized to quantify FVDD defined as serum 25(OH)D levels below 20 ng/mL and PTH serum levels above 65 pg/mL, yielding 0.308 as the lower limit for normal values of 25(OH)D/iPTH ratio. There were no infants included in this analysis with vitamin D toxicity (>100 ng/mL) and thus we are unable to comment on the upper limit of 25(OH)D/iPTH ratio.
As stated above, there was no association between infant UCa/Cr ratio and 25(OH)D at any of the three study visits or over time after controlling for potential confounders. Those findings are consistent with studies that provided children and adults with vitamin D supplementation and reported no association between 25(OH)D and UCa/Cr.12,24,25 To our knowledge, no other studies to date have investigated the association between UCa/Cr and 25(OH)D over time in infants before 7 months of age.
Contrary to the authors' findings, researchers in Northern India evaluated children and adolescents who underwent vitamin D supplementation and reported a positive correlation between UCa/Cr and 25(OH)D. 13 Nonetheless, an abundance of literature supports the results reported herein; this study contests the usefulness of the UCa/Cr ratio given the wide variability of the UCa/Cr ratio previously reported in infants before 7 months of age.6,7,21,26 The unreliability of UCa/Cr ratio to predict daily calcium excretion—combined with the ratio's inconsistent range in infants younger than 7 months of age—calls the use of UCa/Cr ratio into question as a reliable safety parameter for vitamin D intoxication. It is also plausible that the lack of correlation between the UCa/Cr ratio and circulating 25(OH)D is related to the utility of using 25(OH)D as a biomarker of vitamin D status.
Serum 25(OH)D in infants before 7 months of age is a valid biomarker of vitamin D supply, yet the extent to which 25(OH)D estimates the vitamin D supply necessary to elicit a functional physiological response is disputed due to the influence of many downstream factors, 27 thus necessitating a biomarker more directly reflective of the physiological response to vitamin D. Of the many proposed biomarkers, PTH appears most promising. 27
At birth, PTH is the primary regulator of calcium and phosphorus homeostasis. The parathyroid gland is stimulated to secrete PTH when serum calcium decreases. 27 PTH then acts directly on bone to release calcium and phosphorus into circulation; it also acts on the kidneys to increase renal tubule reabsorption of calcium and decrease phosphorus reabsorption. PTH indirectly increases intestinal calcium reabsorption by stimulating the synthesis of 1,25(OH)2D. Thus, the net actions of PTH decrease urinary calcium excretion and increase calcium reabsorption resulting in a net increase in serum calcium. 28
When sufficient serum calcium concentrations are achieved, calcium-sensing receptors on the parathyroid gland signal a decrease in PTH secretion. As expected, infant serum calcium negatively associated with iPTH at each study visit and over time after controlling for potential confounders. This finding is consistent with a study conducted by Okonofua et al., who found an inverse relationship between serum calcium and iPTH in neonates. 29 The current authors found that infant UCa/Cr ratio negatively associated with iPTH at all three study visits and over time after controlling for potential confounders. This finding is consistent with the Northern Indian study of children and adolescents. 13 Thus, the findings reported herein support iPTH as a functional marker of the physiological response to vitamin D.
In this study, an inverse association occurred between 25(OH)D and iPTH, prompting the authors to use the 25(OH)D/iPTH ratio to investigate how 25(OH)D and iPTH comparatively associate with serum calcium and UCa/Cr. A significant positive association occurred between serum calcium and 25(OH)D/iPTH ratio at all three study visits and in the multiple regression analyses. This association was stronger than independent associations among serum calcium and both 25(OH)D and iPTH when analyzed separately. Interestingly, the positive association between UCa/Cr and the 25(OH)D/iPTH ratio was stronger than the inverse association between UCa/Cr and iPTH at all three study visits and in the multiple regression analyses. The findings that iPTH alone and the ratio of 25(OH)D/iPTH were both correlated with UCa/Cr ratio and serum calcium suggest that these measures are better clinical indicators of calcium homeostasis in infants from birth to 7 months.
There is a lack of evidence supporting use of the UCa/Cr ratio as a consistent measure of 25(OH)D in infants before 7 months of age and thus as a valid measure of hypervitaminosis D or toxicity. Few prior studies have reported on the wide variability in UCa/Cr ratios in infants before 7 months of age; moreover, prior studies typically involved small sample sizes.6,7,26,30 The study reported herein contributes to the ongoing research conversation by assessing the associations among the UCa/Cr ratio and serum calcium, 25(OH)D, iPTH, and 25(OH)D/iPTH in a robust number of infants before 7 months of age.
The strengths of this analysis include the strong racial diversity in a large sample of breastfeeding and formula-feeding mother/infant pairs; thus, the findings are relevant to infants of diverse sociodemographic and nutritional backgrounds. Moreover, the infant laboratory safety parameters, UCa/Cr ratio, serum calcium, iPTH, 25(OH)D, and 25(OH)D/iPTH ratio are readily available indicators and, thus, are easily obtained in infants.
The recommendation to monitor serum calcium, iPTH, and to calculate the ratio of circulating 25(OH)D/iPTH if there are concerns of either hypovitaminosis D or hypervitaminosis D would augment measuring total circulating 25(OH)D concentration and place the arbitrary value of 25(OH)D in the context of vitamin D and calcium homeostasis. While such measures would provide guidance regarding the endocrine function of vitamin D and its effect on calcium metabolism, such values, however, do predict the optimal 25(OH)D concentrations necessary for nonendocrine functions of vitamin D, which impact immune development and function.
The limitations of this study include the ability of random urine samples to accurately reflect the concentration of calcium and creatinine over 24 hours because these measurements are influenced by various factors, including time of collection, feeding, and hydration status. 21 The chemical evaluation of random urine samples using a mineral/creatinine ratio relies on the constancy of urinary creatinine to correct for these factors. 11 Urinary creatinine in infancy, however, is variable. As such, it does not improve the reliability of random urine samples. This study only followed infants until 7 months of age, preventing the authors from determining at what point in time, if any, the UCa/Cr ratio becomes less variable and begins to more strongly associate with 25(OH)D. Finally, there were no infants included in this analysis with vitamin D excess or toxicity, and as such, further research should be performed to assess whether 25(OH)D/iPTH ratio is correlated with serum calcium and UCa/Cr ratio at serum 25(OH)D levels above 100 ng/mL.
In conclusion, this study found that infant UCa/Cr and serum calcium are more valid indicators of 25(OH)D/iPTH ratio than either 25(OH)D or iPTH alone. These findings suggest that the infant UCa/Cr ratio and serum calcium are valid markers for infant iPTH levels as well as 25(OH)D/iPTH ratios. Moreover, serum calcium (and not UCa/Cr) appears to be a valid indicator of infant total circulating 25(OH)D. Given these findings we now understand that in infants 1 to 7 months of age, UCa/Cr ratio alone is not a good predictor of total circulating 25-hydroxyvitamin D and therefore serum calcium, 25(OH)D/iPTH, and iPTH should be assessed when addressing vitamin D sufficiency and safety. Further research is needed to confirm these hypotheses.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Funded in part by NIH 5R01HD043921, NIH RR01070, MUSC Department of Pediatrics, and by the South Carolina Clinical & Translational Research (SCTR) Institute, with an academic home at the MUSC, NIH/NCAT Grant number UL1 TR000062.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.