
Abstract
Background:
Physician mothers face many barriers in their ability to meet their lactation goals. This is often due to short maternity leaves and an often busy, inflexible work schedule at the time of return to work. We aimed to characterize the effect of using wireless, wearable breast pumps in the workplace and determine if these devices may help overcome barriers to breastfeeding success for physician mothers.
Methods:
A cross-sectional survey was distributed to female physicians and trainees identified through the group “Doctor Mothers Interested in Lactation Knowledge (Dr. MILK)” using an anonymous, Qualtrics® survey on the group's social media site. Participants were analyzed in two groups: those who had used wearable pumps versus those who had only used traditional breast pumps.
Results:
Of the 542 respondents analyzed, 321 (59%) had used a wearable pump in the workplace and 221 (41%) had only used a traditional electric breast pump. Those who had used a wearable pump reported statistically significant shorter lactation breaks (p < 0.00001) and were more likely to be able to provide breast milk to their infants for their entire intended duration (p = 0.005) compared to the traditional pump group. The ability to pump as often as needed while at work (p = 0.16) and the frequency of lactation breaks throughout the day (p = 0.223) were not significantly different when comparing the two groups.
Conclusions:
This study demonstrates a benefit to using wearable breast pumps for women physicians as they return to work after maternity leave. Utilization of these new wearable pumps correlates with shorter lactation breaks and the ability of physician mothers to provide breast milk to their infants for their intended duration.
Introduction
The American Academy of Pediatrics recommends exclusive breastfeeding for 6 months and continued breastfeeding for 1 year or longer, as mutually desired by the mother or infant. 1 Mothers who breastfeed are at lower risk for postpartum hemorrhage, breast and ovarian cancer, obesity, diabetes, and myocardial infarctions later in life. 2 Likewise, infants who breastfeed have a lower risk of acute otitis media, asthma, type 1 and type 2 diabetes, sudden infant death syndrome, and obesity later in life. 3 While as many as 80% of physicians initiate breastfeeding, 1 in 3 do not meet their goal for exclusive breastfeeding.4,5
Although the support for breastfeeding physicians has improved over the years,6,7 women physicians continue to face a number of barriers to express milk in the workplace, including lack of time, space, and privacy, unpredictable schedules, short maternity leaves, and long working hours.4,8–11 Often, work demands are the main reason given for early cessation of breastfeeding in physician mothers.11–13 Early cessation has been associated with negative emotions and impact on mental health.4,14
To improve convenience and maximize flexibility, new wearable pumps have been designed as a discrete solution to pump on-the-go. The most prevalent of these include the Elvie™ and the Willow™ pumps, which are both wireless devices that can be worn under clothing and used to express milk without the restriction of an external pump motor or external wires or tubing.15,16 Many female physicians have turned to these options as a strategy to overcome the many barriers to expressing milk during a physician's schedule.15,16 Physician mothers have reported an increase in milk supply, reduced stress, and more efficient time management with the use of these devices. 15
In this cross-sectional study, we sought to characterize interventions that augment breastfeeding duration and experience. Specifically, does the use of newly available technologies in wearable breast pumps correlate with improved success and ease of breastfeeding for physician mothers?
Methods
The target population included a convenience sample of female physicians and trainees identified through the social media group “Doctor Mothers Interested in Lactation Knowledge” (Dr. MILK). Members of this group had previously been confirmed as allopathic or osteopathic medical students, residents, fellows, or attending physicians through National Provider Identifier (NPI) number or official work badge image before admission to the private group. The survey was posted to the group page, only visible to the preapproved members, and remained open for 14 days in April 2020. In accordance with the Code of Federal Regulations, 45 CFR 46.102, the activity was determined not to require Institutional Review Board (IRB) review.
The survey instrument (Supplementary Data) was created through an iterative process from collaboration with female physicians who had experience expressing milk in the workplace using either traditional or wearable pumps. The usability and technical functionality of the survey instrument had been trialed with the assistance of five nonparticipant volunteers, all who had previous experience with breastfeeding and pumping. Survey branching logic was incorporated to create alternate survey pathways based on participant responses.
Before beginning the survey, participants were provided with a written description of the purpose of the study, the voluntary nature, and their ability to withdraw at any time. Incentives were not offered for participation. Participants were informed of the expected length of time to complete the survey and provided with contact information of the investigators. The Qualtrics® web-based survey allowed for the opportunity to review and modify answers before submitting. Demographics, including age, race/ethnicity, level of training, and current practice region, were collected.
Inclusion criteria for response analysis included physician or medical student status, having currently or previously expressed milk in the workplace using either a traditional or a wearable pump, and sufficient survey completion.
Summary statistics were used to characterize all participants regarding type of breast pump used in the workplace, duration and frequency of lactation breaks, success in achieving lactation goals, and ability to pump as frequently as desired while at work. These variables were compared between the wearable versus traditional pump groups using Fischer's exact test through the Qualtrics Stats iQ functionality or Mann-Whitney U test for ordinal variables (lactation break duration and frequency). Participants were also asked about the perceived impact a wearable pump had on their experience (if applicable), locations they had pumped while at work, reasons they did not use a wearable pump (if applicable), and their knowledge of policies regarding the use of wearable pumps in public areas of the workplace using preselected descriptors.
Results
Six hundred fifty-five individuals responded to the survey. Those who did not meet inclusion criteria (n = 113, 17.3%) were excluded from the analysis. Participants (n = 542) included physicians at various levels of training with attending physicians making up most of the study group (n = 329, 60.7%) (Table 1). Seventy-four percent of the participants were white (Table 1). A total of 321 (59%) participants had previously used a wearable pump, such as Elvie, Willow, or Freemie™, and a total of 221 (41%) participants had not used a wireless pump, but had used a traditional electric pump in the work setting.
Baseline Characteristics of Participants
Those who had used a wireless pump reported significantly shorter lactation breaks (p < 0.00001) and were more likely to breastfeed or pump for their infants for their entire intended duration (89.0% versus 81.0%, p = 0.005) (Table 2). The ability to pump as often as needed while at work (p = 0.16) and the frequency of lactation breaks throughout the day (p = 0.223) were not significantly different between the two groups (Table 2).
Participants' Ability to Breastfeed for Their Intended Duration, Ability to Pump as Often as Needed While at Work, Length of Dedicated Lactation Breaks While at Work, and Frequency of Lactation Breaks in the Workplace Among All Participants
If participants returned to work duties in a normal capacity while expressing breastmilk with a wearable pump, they were instructed to not include that time as part of the break.
Participants of the wearable pump group were asked to identify the impact that a wireless, wearable pump had on their pumping experience, compared to their use of a traditional pump (if applicable). Two hundred fifty-two of the wearable pump group (n = 321) also had experience using a traditional pump in the workplace and were able to comment. The top 3 perceived impacts of using a wearable pump included women's ability to pump more frequently throughout the day, fewer interruptions to patient care, and their ability to stay more involved in team communication or patient care (Fig. 1A).
Participants could select multiple choices that applied for
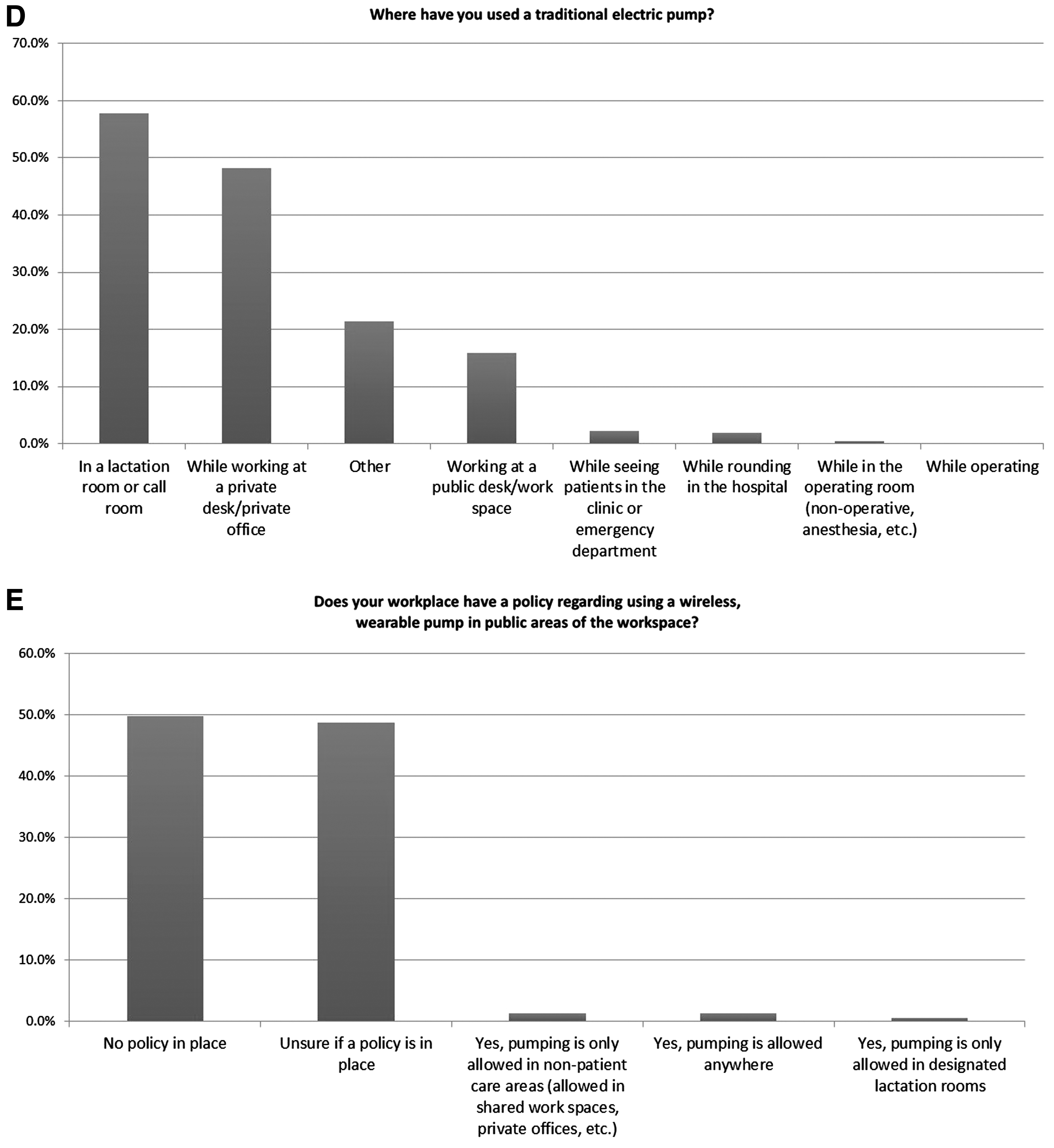
The most common perceived negative effect from wearable pumps was financial hardship associated with purchasing the pump (Fig. 1A), which was the most common reason women gave for not using wearable pumps (Fig. 1B). Women reported using wearable pumps in both private and public workspaces, while seeing patients in the clinic or emergency department, while rounding in the hospital, and while in the operating room (Fig. 1C). The most common locations for use of a traditional pump included lactation or call rooms and private offices (Fig. 1D).
Discussion
This cross-sectional, convenience sample study showed that the use of wearable breast pumps is associated with lactating physicians' ability to provide breast milk to their infants for their intended duration and with shorter lactation breaks. The ability to pump as often as needed while at work and the reported frequency of lactation breaks were not statistically significant between the wearable and traditional pump groups. However, those who used wearable pumps reported a perceived ability to pump more frequently throughout the day compared to their own personal experience using a traditional pump.
Our results confirm previously published data that wearable pumps improve the lactation experience for physician and physician-in-training mothers. 15 McMillin et al. provided wearable breast pumps to a small group of their residents and collected feedback on the impact this had on their breastfeeding experience. 15 The participants reported increased length of time a mother could more easily provide breast milk to their infant, consistent with our findings. Given the substantial cost of these devices, which is typically near 500 dollars and often not wholly covered by insurance (Fig. 1E),17,18 institutions and training programs may consider supplementing the cost or offering a rental program.
While the Affordable Care Act (ACA) requires insurance policies to cover equipment used to express milk, there are no specifications on the types of breast pumps that must be provided. 17 Insurers may choose to only offer manual pumps rather than more expensive electric models, limiting the access to these devices. Organizations such as the American Medical Association should advocate for insurance companies to cover the full cost of wearable breast pumps and address the financial hardship faced by many women who did not use them in our survey.
Although wearable pumps should not be used as a replacement to supportive lactation policies, our results demonstrate that these devices provide an option to physician mothers to multitask and come with multiple benefits. Women identified they could use wearable pumps in many settings where traditional pumps were used uncommonly, such as while seeing patients in clinic, in the emergency department, or even while operating. Although there are policies and laws in place to ensure accessibility to lactation facilities, including sections of the ACA and the Program Requirements from the Accreditation Council for Graduate Medical Education (ACGME), 19 many physicians still perceive designated lactation rooms to be inaccessible due to location or frequent occupation by others.9,14,17
Section 4207 of the ACA requires employers to provide employees a reasonable amount of time to express milk for 1 year after a child's birth. 17 However, this provision generally applies only to hourly workers and employers are not required to compensate mothers during breaks to express milk. 17 This can lead to longer workdays to make up productivity, ultimately keeping mothers away from their infants for longer durations.
Both gaps highlight the benefit a wearable pump can offer, given that these devices do not necessarily require the use of a designated lactation room and they allow for shorter lactation breaks. Lactating physicians have also faced discrimination for discretely pumping in public areas.4,14,16,20 Breast milk is not recognized as a bodily fluid that requires universal precautions and women should not be restricted from performing clinical work while pumping if they so choose. 16 It is imperative that medical institutions support women by instituting clear, evidence-based policies and practices that offer maximal flexibility regarding acceptable locations of use for these closed-system medical devices. Policies normalizing pumping while performing clinical duties can further ensure that women benefit from these devices.
This study is the first of its kind to demonstrate measured benefits of wearable pumps compared to traditional electric pumps. The study captured physicians at all levels of training and from different practice locations throughout the United States. Limitations of this study include recruitment strategy, as the sole distribution of the survey was through a social media group focused on breastfeeding in physician mothers. This has the potential to skew results to those physicians who actively sought support for breastfeeding or had a high pretest probability of initiating and continuing breastfeeding. Also, while we use terms that apply to cis-gendered women, we recognize that breastfeeding and expression of milk are activities that apply to transgender and nonbinary individuals as well.
Nearly three out of every four participants in our study identified as white and we acknowledge that the limited representation from female physicians from other races may limit the generalizability of these results. Future work should examine the benefits of wearable pumps across specialties, as we postulate that these benefits are likely strongest in the surgical specialties due the number of hours dedicated to the operating room and the ability to use these pumps while operating. Although wearable pumps have the potential to improve convenience and ease of pumping for physician mothers, it should be noted that some women will continue to require quiet time and manual expression to allow for an adequate letdown reflex and should be provided with the time and space to do so, even with the use of wearable pumps.
Conclusion
Women physicians benefit from using wireless, wearable breast pumps as they return to work after maternity leave. Utilization of these new wearable pumps correlates with shorter lactation breaks and the ability of physician mothers to provide breast milk to their infants for their intended duration. Medical institutions should enact lactation policies that allow maximal flexibility in the use of these devices in the workplace.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.