
Abstract
Background:
Low human milk production frequently occurs in mothers of premature children with low birth weights who require intensive care.
Research Aims:
To investigate whether corn-based preparations increase human milk production in women with insufficient milk volumes.
Method:
This was an intervention study evaluated whether there was an increase in human milk production after a mother's consumption of corn-based preparations. The participants included women with hypogalactia and mothers of infants in neonatal and pediatric intensive care units. The corn-based preparations included green corn cakes and sweet hominies. A total of 35 mother–infant pairs participated in this study. Each mother served as their own control. The study took place over 2 weeks, and data were collected at baseline and after the intervention. At baseline, a socioeconomic questionnaire was used to collect information regarding maternal food consumption, volume of milk expressed, and infant weight and length. All evaluations, except for questionnaire administration, were performed during the intervention phase, when the lactating women ingested the corn-based preparations.
Results:
A significantly higher average volume of milk was expressed in the intervention period (397.6 ± 182.6 mL/day) compared to baseline (343.6 ± 155.8 mL/day) on the paired t-test (p < 0.001) analysis. Neither energy nor macronutrients consumed correlated with milk volume.
Conclusion:
The tested corn-based preparations acted as galactagogues and could be used to stimulate milk production in lactating women.
Introduction
The World Health Organization recommends that breastfeeding be continued exclusively until the sixth month of life and continue for 2 years or more. 1 In addition to being suitable for the infant's nutritional needs, human milk plays a role in protecting them against infectious diseases in childhood and chronic diseases later in life. 2 Despite these benefits, many mothers are unable to exclusively breastfeed their children.
Hypogalactia is a common cause of early weaning, especially in mothers of premature infants with a low birth weight or neonatal complications that require intensive care. These infants may have feeding difficulties due to poor development of the oral motor system that compromises the initiation of breastfeeding. 3 Feeding difficulties are associated with cesarean delivery, which inhibits or delays the onset of lactation 4 and is commonly used in cases of preterm birth.
When a newborn must remain in the neonatal intensive care unit (NICU), prolonged separation of the mother from the infant may occur. This separation is associated with maternal anxiety when managing newborns who need special care, which can lead to reduced production of the hormones necessary for lactation 5 and hinder milk production.
Galactagogues are commonly used worldwide to stimulate human milk production. 6 They are substances that increase milk production or flow and aim to improve the supply.7,8 A study on lactating mothers in Bali found that most mothers used herbal galactagogues after giving birth (82%) for <1 month. About 95% of respondents felt confident and self-empowered after using herbal galactagogues, demonstrating their psychological benefits. 9 A study in Australia found that 60% of lactating women reported using one or more galactagogues. Commonly reported galactagogues include lactation cookies (47%), brewer's yeast (32%), fenugreek (22%), and domperidone (19%). 10
Among the products with galactagogue properties, some medications and various herbal medicines and foods have been described in the literature. Metoclopramide, domperidone, sulpiride, and oxytocin nasal sprays are among the most commonly used drugs to increase milk supply. 8 These drugs are generally prescribed to women with hypogalactia, whose children are hospitalized in the NICU, to aid with re-lactation, and to adoptive mothers who wish to breastfeed. 7
Several studies have investigated the galactagogue potential of herbal medicines. Moringa (Moringa oleifera Lam), 11 fenugreek (Trigonella foenicum-graecum),12,13 and rue-capraria (Galega officinalis) 14 have been studied for this purpose. These studies have confirmed the galactagogue properties of these herbal medicines.
Different cultures have adopted different foods with galactagogical properties. Peruvian mothers consume soups rich in proteins, such as quinoa soup, lamb meat, Andean bird, and lamb lung soup. 15 Philippine nursing mothers use moringa soup, 16 while Indian women choose turmeric, papaya, and shatavari root soups. 17 Thai women use banana flower soup, spicy vegetable mix soup, and a variety of foods to improve lactation. 18 A study of Malawian women tested the galactagogue properties of banana flower–based biscuits 6 and found that it was associated with increased milk production. In Brazil, hominy and black beer are among the most commonly consumed foods to increase human milk production. 19 However, no studies to date have tested the galactagogue potential of foods or food preparations in Brazil.
Considering these aspects, the present study aimed to verify whether corn-based preparations can increase milk production in women with hypogalactia.
Materials and Methods
Research design
This intervention study investigated milk production before and after the consumption of corn-based preparations. The study duration was 2 weeks, with the first week acting as the baseline and the second week as the intervention. The protocol used in this study is illustrated in Figure 1. We defined an intervention time of 1 week for each phase of the study because the milk production effects caused by the food consumed are reflected in the short term. The food ingested by lactating women generally affect their milk production on the same day. 20
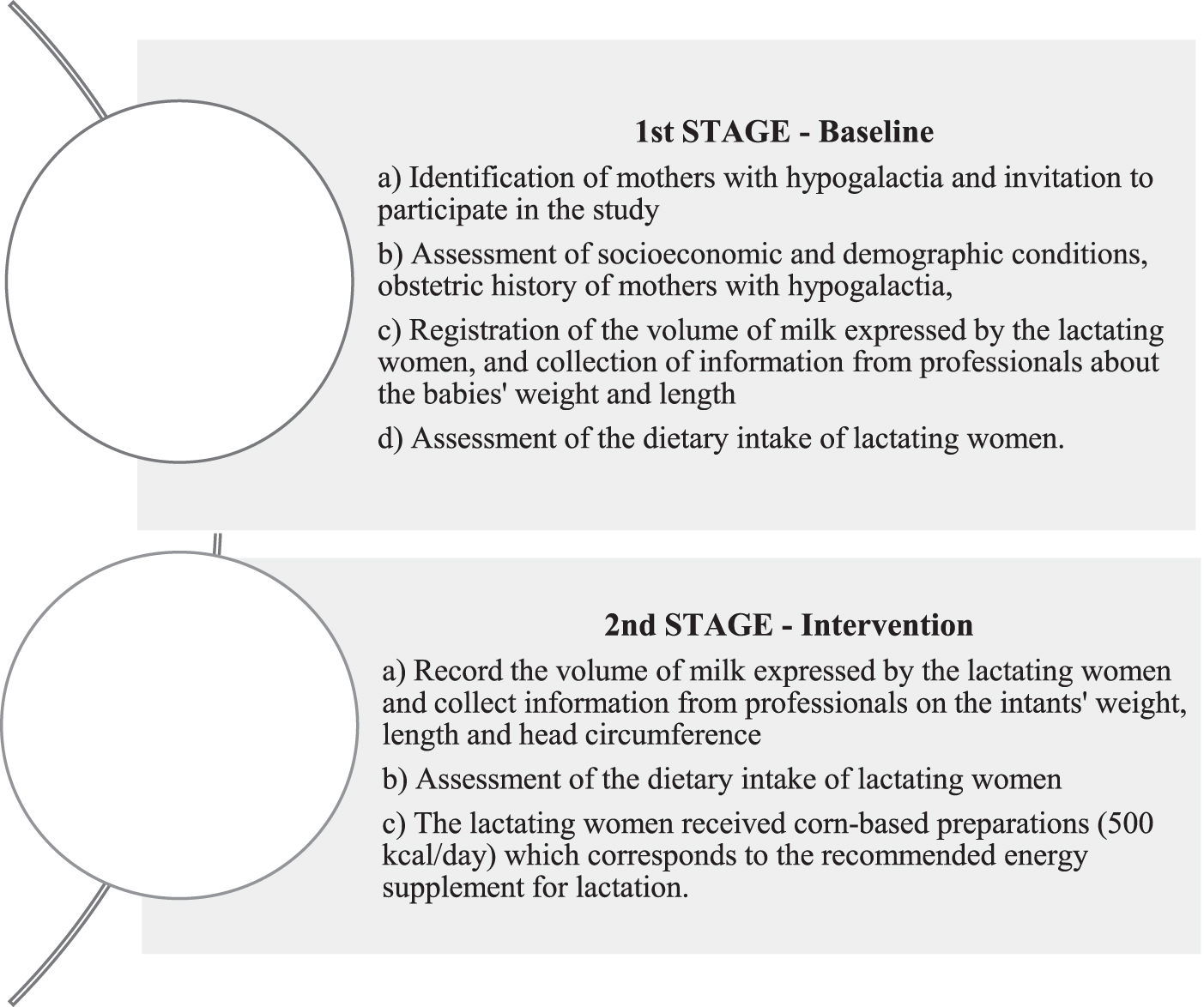
Flowchart of the study enrollment and procedures.
The before-and-after design was chosen because this type of study is most useful for demonstrating the immediate impacts of short-term programs 21 and features lower costs than long-term programs. In this type of study, it is necessary to have good control over internal validity. In this study, the important parameters cited by the Centers for Disease Control 21 as important to be verified were controlled; that is, the mothers were their own controls, all had hypogalactia, were hosted in the pregnant woman's home at the hospital with their children hospitalized in a NICU, consumed standard meals, and used the same method of milk extraction (collection under the supervision of an experienced lactation nurse). Thus, at both stages of the study, the participants were kept in the same emotional and environmental conditions, which are factors that can impact milk production.
The study was approved by the Ethics Committee on Human Research at Federal University of Vales do Jequitinhonha and Mucuri (no. 2.139.138).
Setting and relevant context
This study was conducted at a hospital in the municipality of Diamantina, a city located in north Minas Gerais, Brazil. This hospital is qualified to provide health care for high-risk pregnancies, with in-house pregnancy, baby, and postpartum (HPBP) units linked to the Rede Cegonha of Minas Gerais. This hospital also has a NICU; therefore, it is a reference center for the highly complex care of newborns in the municipality of Diamantina and Vale do Jequitinhonha.
According to the Brazilian Institute of Geography and Statistics, 22 Diamantina had a population of 47,723 in 2019. It is a reference city for health care in Vale do Jequitinhonha, where the city of Diamantina is located.
In this population, exclusive breastfeeding (EBF) rates for premature infants are lower than those for full-term infants. A recent study of the prevalence and duration of EBF of preterm newborns in the first 6 months of life in a prospective Brazilian cohort identified an overall prevalence of EBF at hospital discharge of 40%. The rate of supplementation in this group of infants was 38%. 23 In contrast, Oliveira and Volkmer 24 identified an EBF rate of 16.1%.
Even when it is possible to establish EBF in hospitalized premature infants, many are weaned early in the first weeks after hospital discharge, with EBF declining by a reported 7–25% in the first month after discharge. These rates reveal the lack of support for maternal interventions and the maintenance of breastfeeding despite the undisputed benefits that human milk consumption provides to these infants. 25
Sample
Thirty-five mother–infant pairs participated in the study. Each of their infants were admitted to the hospital's NICU. Mothers residing outside the headquarters of Diamantina or who had children undergoing treatment in the hospital's NICU had the right to stay at the HPBP until their infant's discharge.
Thus, the study eligibility criteria for lactating mothers were as follows: staying at the facility to wait for the discharge of their infants in the NICU; diagnosis of hypogalactia and not using galactagogues; manually extracting human milk to breastfeed their child; not using drugs that hinder lactation (e.g., diuretics, piridoxina) 26 ; the child's NICU stay being longer than 15 days; and the child older than 5 days postpartum. This was because the study lasted for 14 days, and the mothers were required to stay in the hospital for that period. In addition, 5 days postpartum was selected because the volume of milk production peaks by that point. All lactating mothers participating in the study were informed about the objectives and risks of the study, and each signed an informed consent form.
Lactating mothers were excluded from the study if: hypogalactia was not diagnosed; medications that reduce lactation were being used 26 ; galactagogues were being used 27 ; they did not like corn products; their children had an expected discharge date of <15 days; lack of EBF; children had allergic reactions, even if not directly related to the mother's diet; and if diabetes mellitus or lactase deficiency was diagnosed. Considering that the study verified whether corn-based preparations increased human milk production in lactating mothers with hypogalactia, no inclusion criteria were adopted for the study infants.
For this study, hypogalactia was defined as a low milk production (<500 mL/day) after manual expression 28 ; leading to the need to supplement an infant's milk intake with milk from the hospital's collection station.
The sample power calculation was performed a posteriori using the Minitab Statistical Software, considering paired t test, one-sided power
Measurement
Evaluated variables
Maternal and infant data included mother's age and education level, mode of delivery (vaginal or cesarean), marital status (with companion, without companion), whether if the mother worked outside the home (yes or no), gestational age (weeks), number of children, infant's weight (g), and sex (male or female). Maternal and infant data were collected using a questionnaire designed for this study.
During the basal week, the lactating women answered a questionnaire, measured their expressed milk, and recorded their food consumption. In the second week, the participants ingested the corn-based preparations, measured their expressed milk, and recorded their food consumption (Fig. 1).
Corn-based preparation
The corn-based preparation tested in this study was green corn cake and white hominy. These preparations were ingested by the lactating mothers during the intervention week during breakfast, as an afternoon snack, or at supper. One portion of each preparation was served in any of the meals mentioned, and the consumption of both ensured an additional caloric intake of ∼500 kcal/day. All mothers were instructed to consume a full portion of the corn-based preparation.
Before starting the study, standardization of these recipes and a sensory evaluation using acceptance tests were performed by the research team and employees from the hospital's nutrition department. In the sensory evaluation, a 5-point hedonic scale was used, with a classification ranging from “I disliked it a lot” (score of 1) to “I liked it a lot” (score of 5). The sensory evaluation was performed on hospitalized patients, including nursing mothers, and the corn-based preparations showed excellent acceptance. 29
After this stage, a nutritional calculation was performed for the recipes to define the portion size of the preparations necessary to reach 500 kcal. This amount refers to the additional caloric input to the diet of lactating mothers 28 and is recommended to ensure the adequate production of human milk. Therefore, this study proposed offering these additional calories through the corn preparation.
To achieve this amount, green corn cake and white hominy were served to lactating mothers in portions of 100 and 150 g, respectively, with the following nutritional composition: corn cake (229.4 kcal, 22.1 g of carbohydrate, 5.7 g of protein, and 13.2 g of lipid), white hominy (260.8 kcal, 40.3 g of carbohydrate, 6.5 g of protein, and 8.2 g of lipid). Notably, lactating mothers were instructed to eat both preparations to reach the additional caloric amount required for lactation. The proportion of corn in the recipes was 27.5% in the cakes (green corn and cornmeal) and 29.3% in the white hominy (hominy-corn).
Furthermore, the breastfeeding mothers were advised to preferentially consume the standard meals offered by the hospital's nutrition service during the 2-week study period and to ingest 2 L of liquid per day.
It is noteworthy that the hospital offers five meals to patients: breakfast, lunch, afternoon snack, dinner, and evening snack. In the case of lactating mothers, the menu offered has ∼2,700 calories, including the extra 500 calories required for lactation. Therefore, in the first week of the study, this additional food was provided along with the usual food on the menu. In the second week, minor adjustments were made, such as reducing the portion sizes of some foods or substituting products, especially for breakfast, afternoon snacks, or suppers, to guarantee the maintenance of 2,700 kcal/day, but including the 500 calories from the corn-based preparations.
Milk sample collection
The hospital's routine is that a breastfeeding woman with a child in the NICU should express milk every 3 hours to feed her child if the child is not feeding directly from the breast. This milking (manual milking) must occur at the hospital's milk collection station, which offers adequate space and professional nursing support. For the quantification of milk in this study, the lactating mother measured the milk expressed in fractionated glasses (bottles from the hospital itself) and noted the values on a specific form. All of the mothers were instructed to empty their breasts during each milking.
Evaluation of food consumption
The food consumption of these mothers was evaluated in the 2-week study period using four sets of 24-hour dietary recalls, with two performed at baseline and two performed in the intervention week.
The calculation of the energy and macronutrients of these recalls was performed using the food composition table of the family budget survey (POF) 2008/2009. 30 Considering the distribution of energy intake and macronutrients, the data were adjusted to reduce inter- and intraindividual variability and assessed using the multiple source method. 31 Thus, the usual intake values were used to analyze the relationship between food consumption and human milk production.
Data collection
Data were collected between October 2017 and July 2020. After identifying eligible lactating women, two nutritionists or nurses invited them to participate in the study. In cases of acceptance, informed consent was obtained from the mother. All participants were followed up for 2 weeks by two nutrition students who administered the survey questionnaires and followed up with the mothers during the 2-week survey period to evaluate their food consumption and expressed milk volume. Participant confidentiality was maintained by de-identifying all data collected and using password-protected files.
Data analysis
The data were analyzed using SPSS statistical software for Windows (SPSS ver. 25.0; IBM Corp, Armonk, NY, EUA) and Minitab (version 19; LLS, State College, Pennsylvania, EUA). Statistical significance was set at p ≤ 0.05. The analyzed variables were described using descriptive statistics. Before the analysis, the data were inspected for normality and outliers using the Kolmogorov–Smirnov test; no outliers were removed. As the food consumption data tended to be skewed and deviated significantly from normal for all variables, nonparametric tests were used for all of the analyses. The treatment effect (ingestion of corn-based preparations) was evaluated using a t-test for dependent samples, which evaluated the difference in the average volume of milk expressed during the baseline versus intervention periods. In addition, ordinal logistic regression was performed to identify how the corn-based preparations affected milk production considering the three milk volume strata expressed at baseline.
Results
Characteristics of the mother–infant pairs
During the study period, 107 mother–infant pairs were evaluated; however, due to several factors, such as mothers' withdrawal from the study, infants' hospital discharge, incomplete milking data, incomplete food intake data, transfer of the infant to another hospital unit, and infant death, the final sample comprised 35 mother–infant pairs. Table 1 presents the characteristics of the participating lactating mother–infant pairs.
Characterization of the Mother–Infant Pairs
Most mothers (n = 26 [74.3%]) received a minimum monthly wage. An assessment of per capita income revealed that the same number of breastfeeding women lived with a per capita income below half the minimum monthly wage. Most mothers lived in urban areas (n = 26 [74.3%]) and did not work outside the home (n = 26 [74.3%]).
Regarding obstetric history, the majority of the lactating mothers were of the first pregnancy, all of whom underwent prenatal care, most of which was performed in Brazilian public health system (n = 29 [82.9%]), and twenty one mothers (60%) had six prenatal consultations before delivery. Most of the women had a premature birth (n = 27 [77.1%]), and most had to undergo an emergency cesarean section (n = 16 [48.6%]). The average infant birth weight was 1,705 ± 833.7 g.
In this study, the causes of prematurity were not investigated; therefore, we did not collect this information. However, many mothers were primiparas (27.8%), and preterm birth during the first pregnancy was more common than that in multiparas.
Corn-based preparation and milk production
The total mean volume of milk expressed by the lactating mothers was 343.6 ± 155.8 mL/day at baseline versus 397.6 ± 182.6 mL/day in the intervention period (use of corn-based preparation); these values were compared using the t-test (p < 0.01) (Fig. 2). The paired mean difference of milk expressed between the 2 weeks was 53.5 ± 14.3 mL/day.
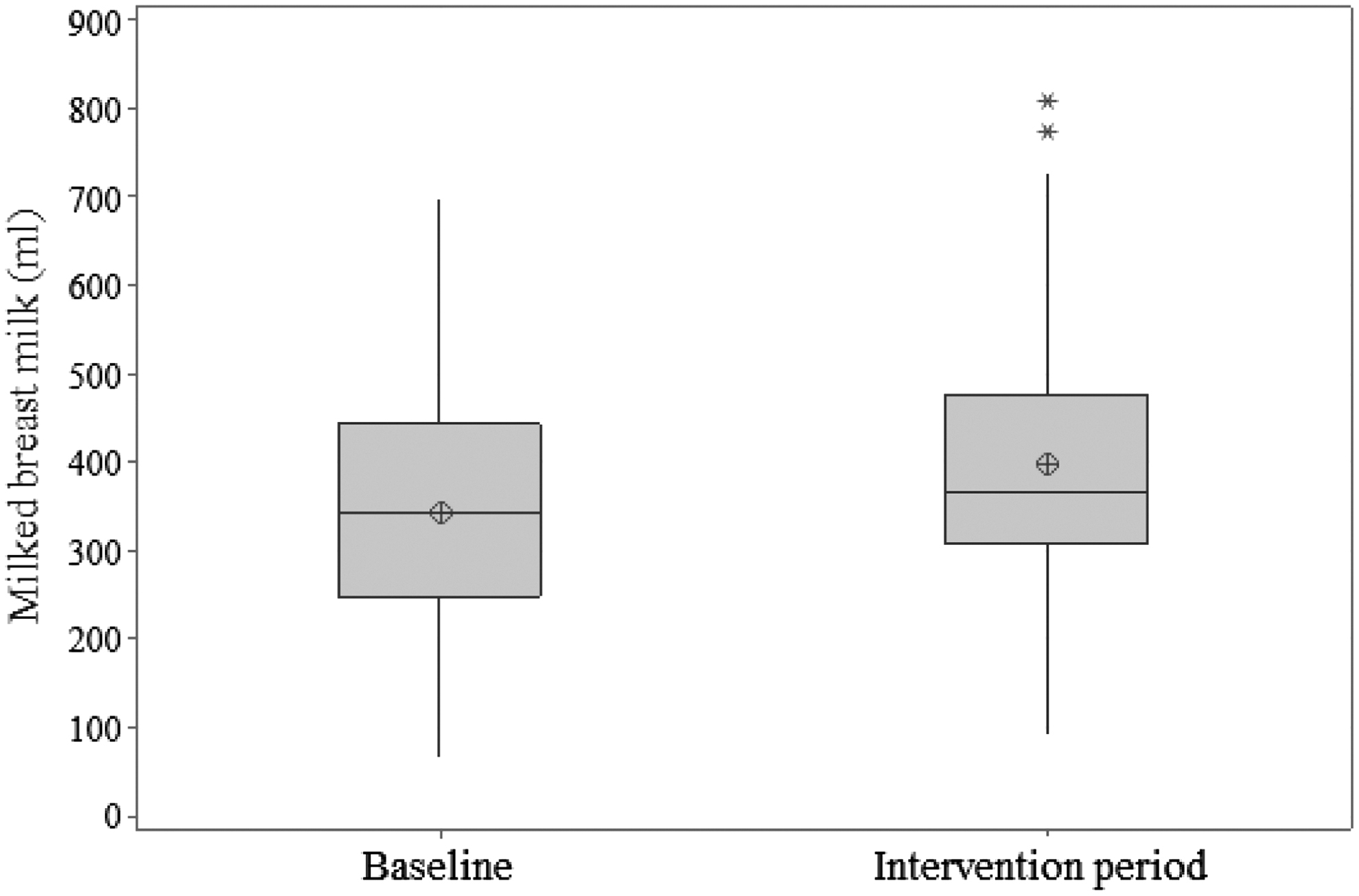
Average volume of milk expressed by mothers by study period.
Food intake and milk production
The lactating mothers' food intake indicated that they ingested a median of 2,685.6 kcal/day in the baseline period versus 2,779.2 kcal/day in the intervention period. When the percentage distribution of energy and macronutrients was verified, the following distribution was identified 59.9:14.7:24.8 (carbohydrate:protein:lipid) in the baseline period versus 58.2:14.4:27.2 (carbohydrate:protein:lipid) in the intervention period.
Comparing the median values of energy intake and macronutrients between the study periods, we found that the median values of energy (p = 0.02), protein (p = 0.03), and lipid (p < 0.001) differed significantly between the study periods, whereas carbohydrate intake (p = 0.47) did not differ significantly according to the Wilcoxon test for paired samples. The statistical power for carbohydrate (0.15) and protein (0.40) intake were low, unlike that for lipid (1.0) and energy (0.80) intake. A resampling (bootstrapping) of 350 values was performed to obtain a distribution of the pairwise difference of these macronutrients with a statistical power of one. As a result, the difference in intake between the study periods differed statistically from zero (p < 0.001) for both energy and macronutrients. The influence of this higher macronutrient intake on the increase in milk production was evaluated using multiple linear regression. There was no significant effect of any increase in macronutrient intake on milk production.
Although there is a statistical difference between the median energy, lipid, and protein consumptions in the study periods, an expressive difference (14.4%) was observed only in lipid intake; the other intakes differed by less than 2%. A correlation analysis was performed between the volume of milk expressed and the consumed values of energy and macronutrients in both study phases. As shown in Table 2, there were no statistically significant correlations between any of the variables and milk production.
Median Energy and Macronutrient Intakes by Study Phase and Correlation with Volume of Expressed Milk
Correlation values obtained by Spearman's test.
Considering that the corn-based preparations tested in this study stimulated lactation, an ordinal logistic regression model was used to evaluate whether the increase in milk production was dependent on the volume of milk produced at the baseline (Table 3, Fig. 3).

Estimating the galactagogue potential of corn-based preparations considering the baseline expressed milk volume.
Ordinal Logistic Model for Increase in Average Daily Breast Milk Relative to Baseline (%) and Tertile of Human Milk Expressed
Lack of fit (p = 0.316).
The increase in milk production was related to the baseline milk volume (Fig. 3). When the volume of milk expressed at baseline was divided into three strata (tertiles), there was a greater probability of an increase in the lower tertile. Thus, the probabilities of a 25% increase in milk production were 37%, 36%, and 26% in the 1st, 2nd, and 3rd tertiles, respectively. The probabilities of a 50% increase in milk were 51%, 32%, and 15% in the 1st, 2nd, and 3rd tertiles, respectively. This result confirms that lactating women with lower baseline milk production benefited the most from the corn-based preparations tested in this study.
Discussion
The sociodemographic characteristics of lactating mothers in the present study differ from those of previous studies of galactagogues.6,11,12,18 In addition to delivery type, studies also identified a higher proportion of vaginal deliveries and male infants.12,18
It is difficult to compare the results of this study with those of other galactagogue studies because no scientific study to date has tested the galactagogue potential of corn or corn-based preparations. In a systematic review of galactagogues, 32 some studies used corn starch capsules, whereas none tested the corn galactagogue effect or corn-based preparations; thus, we conclude that corn is not considered by researchers as a possible galactagogue. However, studies suggest that, among other foods, corn and corn-based preparations are used by lactating Brazilian women to increase their milk production.33,34
Considering that no study has examined the galactagogue action of corn, it remains unknown which corn component would exert this action. Schettler 34 reported that corn and corn products exert estrogenic activities. This hormone stimulates mammary gland and duct development. This is one possible explanation for the relationship between corn consumption and milk production. The nutritional composition of corn can also explain this action; in addition to containing carbohydrate, corn is rich in fiber and polyunsaturated fatty acids. These nutrients have been used to explain the effect of banana blossoms on galactogenesis. 6
When comparing the intervention time of this study with that of similar studies, our results were similar to those of a study conducted in women from Malaysia 6 and the study by Abdoua and Fatheyb. 12 The first 6 lasted 10 days: 5 days for the baseline data collection and 5 days for the intervention period. The second 12 lasted for a period of 15 days. As previously stated, what the lactating woman ingests during the day is reflected on that same day in her milk production; thus, we believe that the intervention time was adequate. However, it is noteworthy that in the present study, the mothers performed manual milking, a process that is difficult to perform. In contrast, in the studies by Nordin et al 6 and Abdoua and Fatheyb, 12 milking was performed using an electric or manual pump, a more efficient process for emptying the breast. Despite this, a statistical difference was identified between milk volumes (baseline versus intervention).
Conducting an intervention study in this group was difficult. The experience of motherhood and all the changes it triggers in a woman's life, especially in the early breastfeeding period, can make studies difficult; this is likely why such studies are scarce. We identified only one study 6 that tested the effect of food preparation on human milk production.
The production of human milk can be affected by several factors, including emotional state. In this study, all lactating women were under stress, as their children were hospitalized in the NICU and away from their families, a negative factor for lactogenesis. However, corn-based preparations favored increased milk production, especially in women with lower baseline production volumes. Thus, in environments with greater comfort and stress reduction, an even better result would likely have been obtained than that observed in this study.
Although we cannot affirm that corn was responsible for the increase in human milk production, this study seems to confirm the popular knowledge present in Brazilian culture that preparations with corn increase the production of human milk.
The results presented here corroborate the statement by Brotto et al, 35 who affirmed that it is essential for health professionals to add the cultural legacy of puerperal women to their care to identify a balance between science and common sense, thereby discouraging practices that are harmful to the mother–child pair and providing scientific support to practices for women that are part of the cultural and family heritage.
The study has positive points that set it apart from the intervention studies mentioned here: the collection of human milk was performed in a hospital with the help of a lactation specialist. As all lactating mothers were staying at a nursing home for pregnant women, it was easier for them to adhere to the study protocol and obtain and record their dietary information.
However, it is important to note that in this study, each mother was their own historical control, and it is expected that as the postpartum days go by, there is an increase in breast milk production. Thus, this time could explain why in the second week (intervention period), there was an increase in the volume of milk; and not eating corn-based food products. It is noteworthy that several of the mothers studied had more than 20 days postpartum, a period in which breastmilk would be in full production. And possible justifications for this problem is this that hypogalactia is common in mothers whose children are in the NICU, either because of the baby's difficulty in sucking the breast or because of anxiety and worry about the babies' health. Both factors impact the lower production of breast milk.
Limitations
Some limitations of our study were that it was a relatively small and sociodemographically homogeneous sample, which limits the generalizability of our findings. Due to a lack of financial resources, it was not possible to measure prolactin levels of the lactating women during the experiment, which could have indicated whether the corn-based preparations induced increased prolactin secretion. Another limitation is that each mother served as their own historical control, and the ideal would be to develop a randomized controlled study.
Conclusion
To our knowledge, this study is the first to evaluate the relationship between corn-based product consumption and increased human milk production. The study confirmed the cultural legacy experienced by lactating Brazilian women that has been passed down from generation to generation that corn-based preparations increase human milk production.
In our study, energy and macronutrient intakes did not correlate with human milk production, and there was no statistical difference in energy intake between the baseline and intervention study periods. We found that corn-based preparations are more likely to increase human milk production among women with a lower baseline milk production, indicating that their use can be recommended for lactating women with more severe hypogalactia, such as those whose infants are admitted to the NICU.
However, further studies are needed, including the testing of other corn-based preparations and corn alone, studying the nutritional components of corn that may impact milk production and measuring prolactin levels to better understand the mechanism of action of this phenomenon.
Footnotes
Authors' Contributions
M.C.A.: conceptualization (supporting); article writing—original draft (lead); article writing—review and editing (equal). J.P.V.D.: data collection (lead); article writing, reviewing, and editing (equal). M.C.C.: data collection (lead); article writing, reviewing, and editing (equal). C.A.S.: article writing—review and editing (equal). D.S.S.S.: article writing—review and editing (equal). P.S.C.S.: article writing—review and editing (equal). L.N.N.: study conceptualization (supporting); methodology (lead); article writing—review and editing (lead).
Disclosure Statement
The authors declare no conflicts of interest. The first author is currently a master's student in the Graduate Program in Health, Society, and Environment in Diamantina, MG, Brazil. This article is the product of her dissertation.
Funding Information
No funding was received for this article.