
Abstract
Background:
Health care trainees lack opportunities to practice breast assessment and clinical skills with patients, making breast models significant for hands-on training. Insufficient training leads to low competence across practitioners in breast health areas of practice, including clinical lactation. The aim of this review was to describe types of breast models used to teach clinical skills of the breast across breast health areas. The secondary aims were to describe education interventions that included each model and identify whether multiple skin tones were available in models.
Methods:
Authors conducted a scoping review to identify which types of breast models are used to teach clinical skills across breast health areas of practice and determine gaps in literature regarding how clinical lactation skills are taught. The literature search was conducted in PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus, MedLine, and ProQuest. Inclusion criteria were students/professionals engaging in breast model simulation. Eighteen studies were reviewed. Authors extracted data on participants, breast health area, breast model, intervention, evaluation, general outcomes, skin tone, and research design.
Results:
The most common skill area was clinical breast exam (n = 7), while least was breastfeeding education (n = 1). Most models were commercial (n = 12). Zero studies described skin tone. Generally, breast model simulations were correlated with increased clinical skills and confidence regardless of model used.
Conclusions:
Despite demonstrated gain of skills, this review reveals inconsistent use of breast models and evaluation, exclusion of diverse skin tones, and lack of breast models reported to teach clinical lactation skills.
Introduction
Hands-on clinical and surgical training for intimate body parts including the breast are limited because patients are hesitant to reveal an intimate body part to health professional trainees. 1 Performing a clinical breast exam is a necessary skill of health practitioners for routine physical examinations for all women; in particular, it is significant for breastfeeding management or for screening and diagnosing breast anomalies.2,3 For example, a female patient might have interaction with medical trainees in the hospital setting within the context of a breastfeeding assessment in the early post-partum period. However, these real-life patient interactions are often not feasible during medical training. 4 As a result, health care trainees have a limited number of opportunities to interact with patients and practice hands-on breast assessments. Clinicians without adequate training for clinical skills with an intimate body part have low competence and confidence and are at risk of making errors in clinical decision making, resulting in morbidities that may have otherwise been preventable.5–7
High-fidelity simulation, which represents the psychological, environmental, and situational factors within clinical scenario, is the gold standard for clinical skills acquisition in nursing and medical education.8–10 Therefore, high-fidelity breast models should appropriately represent anatomy, physiology, and racial/ethnic backgrounds through realistic features and abilities (look, feel, and functionality), such as expression of milk from nipples by hand, use of a breast pump with different flanges, multiple skin tones, ability to perform a biopsy, and ability to aspirate fluid.10–12
However, the training that is provided to pre-licensure or practicing health practitioners for breast assessments vary and include low- (i.e., unrealistic) or high-fidelity simulators, passive learning (e.g., watching a video), or a hybrid approach (i.e., using two or more approaches). 13 For simulated experiences, hospitals and training programs have used sock puppets, the instructors' or learners' own elbows, cloth dolls, poultry breasts, and silicone models for teaching breast assessments or surgical skills of the breast. 14 Without the standardization of teaching methods or wide-spread use of high-fidelity simulators, health professional students, medical students, and residents enter their field with varying skill and confidence levels for breast assessments or surgical techniques. 14
One example of a field in which breast assessment skills are repeatedly reported as insufficient is clinical lactation. 15 The lack of appropriate health professional care is one of the top barriers reported for early cessation of breastfeeding by new mothers even though several leading health organizations have called out the importance of physician education in clinical lactation.16–18 The use of high-fidelity breast models has recently been reported in midwifery students to result in efficacy and development of clinical lactation skills, 19 yet widely speaking health professionals are still reporting a lack of confidence and ability to appropriately care for breastfeeding patients.20,21 With a lack of ability across health professions to manage breastfeeding patients' care, breastfeeding rates will continue to be inadequate and continue to feed into disparities we see across populations. 7
To unveil the types and number of breast models being reported to teach clinical lactation skills, we conducted a scoping review of breast models used for training of clinical skills in breastfeeding management, the general breast exam, and surgery. The primary aim was to describe the types of breast models used to teach clinical skills of the breast across different breast health areas. The secondary aims of this review were to describe the education intervention that included each breast model and to identify whether multiple skin tones were available in the model used.
Methods
Research design
The authors conducted a scoping review to describe the types of breast models used to teach clinical skills across various breast health areas of practice. The authors could not conduct a meta-analysis due to the inconsistency of the type of research studies utilized for the various educational interventions and diverse types of breast models used within each intervention. The scoping review allowed the authors to identify which types of breast models were used to teach clinical lactation skills across various breast health areas of practice and to determine gaps in the literature regarding how clinical lactation skills were taught and reported on. Additionally, it is of significance to understand across breast health areas including lactation/breastfeeding, general clinical breast exams, breast surgery, radiology, and biopsy, whether diverse skin tones are being utilized to identify if this is a gap in health profession training that could ultimately reduce health disparities, including disparities in breastfeeding, if addressed.
Sample
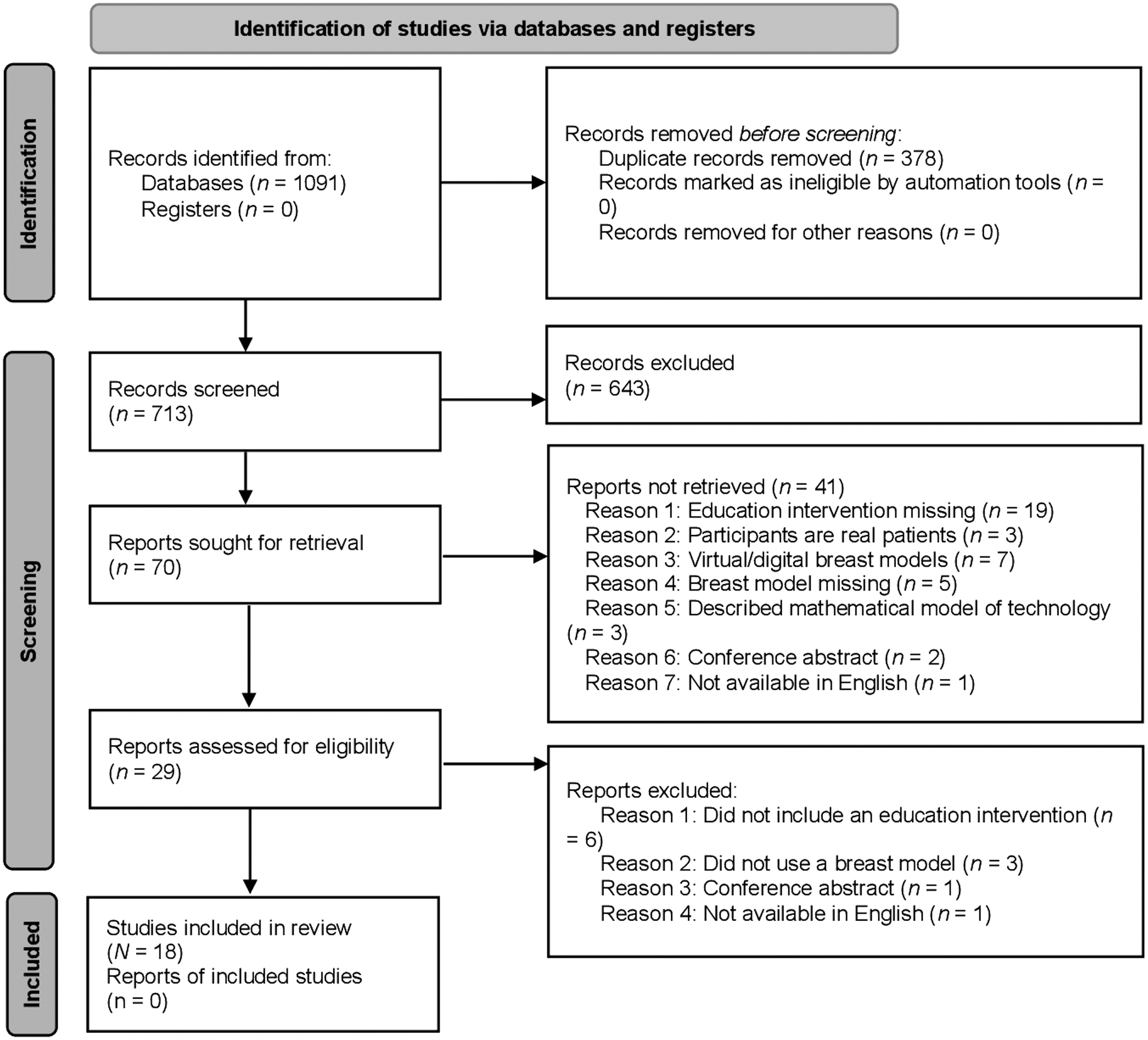
A total of 713 articles resulted from our initial search (Fig. 1). The inclusion criteria were determined before the literature search was initiated to best capture the study aims. The inclusion criteria included: (1) use of a breast model in an educational setting, (2) an education intervention with proposed outcomes, (3) undergraduates, graduate students, trainees, or professionals engaging in the education intervention, (4) original research publication in English, and (5) a study published in a peer-reviewed journal between 2011 and 2019. Exclusion criteria were studies published before 2011 and those utilizing virtual or mathematical simulation models.
Sample selection process.
The author who did the initial search excluded duplicated search results and those articles that were published before 2011 (n = 378). The article titles (N = 713) were screened by this author and one more. Articles were excluded (n = 643) after title screening if they there was not an indication of potential use of a breast model or an area of breast health was not indicated in their title. Article abstracts (N = 70) were then screened. Articles were excluded (n = 41) after the abstract screening for the following reasons: education intervention missing (n = 19); virtual/digital breast models used (n = 7); breast model missing (n = 5); subject/participants were patients (n = 4); described mathematical models of imaging technology (n = 3); conference abstract (n = 2); manuscript not available in English (n = 1).
The remaining full articles were screened (N = 29) after which 11 were excluded for the following reasons: education intervention missing (n = 6); breast model missing (n = 3); conference abstract (n = 1); and article not available in English (n = 1). Any discrepancies in exclusion strategies were discussed between the two authors. The final sample consisted of 18 studies that matched the inclusion criteria and were fully reviewed by the authors (Fig. 1).
Data collection
One author conducted the initial literature search in January 2020. The search terms were developed with assistance from a Health Sciences Informationist/Librarian at the author's institution. The search was conducted in the following five databases: PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus, MedLine, and ProQuest. The search strategy for each database was developed, finalized, and stored within a Google sheet. Upon completion of a search within a database, the items were downloaded into a Zotero library.
The search strategy used Boolean techniques. An example of the terms included are represented here in our MEDLINE search: (“Simulation Training”[Mesh] OR “Simulation Model” OR “Simulation Models” OR Simulator*[All Fields] OR Simulation* OR “Task trainer” OR “Task trainers” OR Manikin*) AND (“breast feeding”[mesh] OR “breast feeding” OR “breastfeeding”[all fields] OR “breast model”[all fields] OR “lactation”[all fields] OR “Breast”[TW] OR “Mammary gland”) AND (“Education” OR “Training” OR ((Knowledge OR Skill*) AND (Master* OR Acquir* OR Build*)) OR “Learning” OR “Education medical” OR “education professional” OR “students health occupations”). Please note that breastfeeding terms were specifically used to eliminate other non-human mammal articles.
Measurement
To determine the extent of breast models being used to specifically teach clinical lactation skills and what types of models were being used, the specific variables analyzed by the authors included type of research design, breast model, education intervention, evaluation techniques, and model skin tone. The main types of research design included were case study, correlational, longitudinal, experimental, or clinical trial (Supplementary Table S1). The types of breast models were defined as simulators but excluded computer-based simulated algorithms. The education intervention was defined as the study participants acting as learners by using the breast model to gain knowledge or skills. The evaluation techniques were defined as assessing learner knowledge or skills after interacting with the breast model. Skin tone was determined by mention of the model's skin tone in each article's Methods or Results sections.
Data analysis
The authors used a Google Sheet as a data abstraction tool for real-time collaboration. The Google Sheet contained a table with the following variables for each column: (1) Research aim/question, (2) Study design, (3) Learner type (including profession), (4) Location, (5) Type of breast health care, (6) Type of breast model, (7) Breast model manufacturer (if described, we explicitly included in our table), (8) Education intervention description, (9) Evaluation description, (10) Validity of evaluation tools, (11) Reliability of evaluation tools, (12) General direction of learning outcomes, (13) Appropriate conclusions, (14) Potential biases, and (15) Breast model skin tone (if applicable or stated; yes/no).
We critically analyzed the sample of articles by first deconstructing the data variables within each article. 22 The deconstructed variables were analyzed by two investigators for methodological congruence to ensure the research aim, study design, data collection, and analysis were in alignment. The two investigators also cross-examined each other regarding potential biases, appropriateness of stated conclusions, and the validity and reliability of the evaluation tools. The investigators cross-examined each other and discussed discrepancies. The learning outcomes were generalized regarding direction. The frequencies for research study design type, breast model type, potential biases, valid and reliable evaluation tools, and skin tone were calculated. The variables were reconstructed across the articles to compare contexts and identify strengths, weaknesses, and gaps in the literature.
Results
Characteristics of the sample
A total of 18 articles matched the inclusion criteria and underwent a full review (Table 1). Twelve (67%) of reviewed articles were quasi-experimental studies (Tables 1 and 2),23–34 4 (22%) of the articles were case studies,4,35–37 and 2 (11%) were experimental studies with clearly defined controls.38,39
Characteristics of the Articles Reviewed (N = 18)
CBE, clinical breast exam; SP, standardized patient.
Description of the Variables Analyzed Within the Articles Reviewed (N = 18) by Breast Health Area Including Breast Model Type, Educational Intervention, Summary of Intervention Results, and Critical Appraisal
“Not indicated in the article” means that the authors did not state the manufacturer of the breast model.
The results are indicated in directionality of outcomes.
BCNB, breast core needle biopsy; CBE, clinical breast exam; G1, intervention group, G2, control group; GRS, global rating scale; MD, multi-disciplinary; MDT, multi-disciplinary team; MOAT, mammaplasty objective assessment tool; ODS, oncoplastic deviation score; OSCE, objective structured clinical examination; SP, standardized patient; US, ultrasound; WLE, wide local excision.
Six (33%) of the studies were conducted in the United States,25,28,30,31,37,39 while two (11%) took place in Ireland35,36 and two (11%) took place in Canada (Table 1).26,27 The remaining studies took place in the following locations: China, Turkey, Lebanon, Rwanda, Columbia, Australia, and the United Kingdom.23,24,29,32–34,38 The study in Rwanda represented health professional breast health interventions in a developing, low-income country (n = 1, 6%). 32 The location of one study could not be determined. 4
Twelve (67%) of the studies were determined to have methodological congruence (Table 2).23–25,28,30,32–34,36–39 The six (33%) that were unclear regarding methodological congruence was due to small sample size.4,26,27,29,31,35 Two types of biases within the studies included investigator influence (n = 9, 50%)4,26,27,29,31,34–37 related to the breast model being made by the investigator and selection bias for the education intervention (n = 2, 11%).28,31 Fourteen (78%) of the investigators used validated evaluation tools4,24,26–29,31–38 while only 6 (33%) investigators used reliable evaluation tools.4,28,29,33,34,37 Six (33%) investigators used both validated and reliable evaluation tools.4,28,29,33,34,37 Three (17%) investigators used neither validated or reliable evaluation tools.23,25,30
The areas of breast health investigated by each article included breastfeeding education (n = 1, 6%), 33 clinical breast exam (n = 7, 39%),4,23,25,28,30,38,39 breast surgery and imaging (n = 10, 56%) including the sub-categories of non-biopsy surgical procedures (n = 4),26,27,29,34 ultrasound-guided biopsy procedures (n = 2),31,37 biopsy procedure without ultrasound guidance (n = 1), 32 and biopsy without associated surgical procedures (n = 3) (Table 2).24,35,36
Breastfeeding education
Only one article described models used in breastfeeding management skills (n = 1 of 18, 6%; Table 2). 33 The breast model in this study came from a manufacturer, but the investigators did not mention which manufacturer it was. The intervention included a didactic portion in addition to the simulation. The surveys measured learners' skills, confidence, and satisfaction. This article did not describe skin tone of the model.
Clinical breast exam
Of the seven articles using breast models in the context of clinical exams, three of the seven described the use of a silicone-based model (n = 3 of 7, 43%),4,23,28 while the others included a torso model (n = 1, 14%), 39 a jacket (n = 1, 14%), 38 an adult mannequin (n = 1, 14%), 30 or one just described as a “breast model” (n = 1, 14%; Table 2). 25 Of the these models six came from a manufacturer (86%),23,25,28,30,38,39 although two studies did not mention the manufacturer specifically,23,28 and one was made by the investigators (14%). 4
The interventions described were mostly traditional didactic learning environments (e.g., lecture plus simulation) (n = 6, 86%)4,23,25,30,38,39 and one was a validation study in which conference attendees were tasked to perform a clinical breast exam (14%). 28 Two studies (29%) utilized a clinical skills evaluation for baseline assessment of a model.28,30 Four of the interventions (57%) utilized pre- and post-surveys.25,28,30,39 One of the studies (14%) utilized practicing medical professionals (i.e., not students or residents) to evaluate the breast simulator in the intervention. 29 Most of the surveys measured learners' skills and confidence (n = 5, 71%).23,25,30,38,39 Two surveys (29%) measured learner satisfaction.23,38 Zero studies (0%) reviewed described the skin tone of the model.
Breast surgery and imaging
Non-biopsy surgical procedures
Four of the articles reviewed described simulation of non-biopsy surgical procedures (n = 4 of 18, 22%).26,27,29,34 Three of the four articles on surgery interventions were focused on breast augmentation (n = 3 of 4, 75%)26,27,34 and one on oncoplastic surgery (n = 1 of 4, 25%; Table 2). 29 Silicone-based models were the most common type of models used for surgery training (n = 3 of 4, 75%),26,27,29 while one used a mannequin made of fiberglass (25%). 34 Of these models one came from a manufacturer (25%), 29 although the study did not mention which manufacturer it was, and three were made by the investigators (75%).26,27,34
Most interventions described did not include a didactic portion but rather only the simulated task (n = 3, 75%),26,27,29 while one described a traditional didactic learning environment (i.e., lecture plus simulation) (25%). 34 One of the interventions (25%) utilized pre- and post-surveys. 34 Three of the studies (75%) utilized practicing medical professionals (i.e., not students or residents) to evaluate the breast simulator in the intervention.26,27,29 One survey measured learners' skills and confidence (25%). 34 Zero studies (0%) reviewed described the skin tone of the model.
Ultrasound-guided biopsy procedures
Two articles described ultrasound-guided needle biopsies (n = 2 of 18, 11%; Table 2).31,37 All interventions described used a breast phantom, but each consisted of unique materials. Both phantoms came from a manufacturer, although one study (n = 1 of 2, 50%) did not mention the manufacturer specifically. 31 Both of the interventions described did not include a didactic portion but rather only the simulated task. One of the studies (50%) utilized a clinical skills evaluation for baseline assessment of a model. 37 All interventions utilized pre- and post-surveys. One survey measured learners' skills (50%). 31 The surveys used in both interventions measured learners' confidence. Zero studies (0%) reviewed described the skin tone of the model.
Biopsy procedure without ultrasound guidance
Only one article described a needle biopsy without ultrasound guidance (n = 1 of 18, 6%; Table 2). 32 The breast model in this study was made by the investigator. The intervention included a didactic portion in addition to the simulation. The investigators described an intervention that utilized a clinical skills evaluation for baseline assessment of a model and utilized pre- and post-surveys. The surveys measured learners' skills and confidence. This article did not describe skin tone of the model.
Ultrasound without associated surgical procedures
Three articles focused on screening procedures through ultrasounds unrelated to surgical procedures (n = 3 of 18, 17%).24,35,36 All interventions described used a breast phantom, but each consisted of unique materials. One of the phantoms came from a manufacturer (n = 1 of 3, 33%), 24 but did not mention the manufacturer specifically and two were made by the investigators (67%).35,36 One of the interventions described did not include a didactic portion but rather only the simulated task (33%) 35 and two described a traditional didactic learning environment (67%).24,36 Two of the studies (67%) utilized a clinical skills evaluation for baseline assessment of a model.35,36 All interventions utilized pre- and post-surveys.24,35,36 One study specifically utilized the pre- and post-surveys to evaluate interprofessional collaboration and communication in breast cancer management (n = 1, 33%). 24 One survey (33%) measured learner satisfaction. 24 Zero studies (0%) reviewed described the skin tone of the model.
Discussion
This scoping review of studies that used breast models within the context of an educational experience for health professionals revealed a variety of models used, variability on the inclusion of manufacturer type in the methods, and a surprising propensity for the handmade construction of breast models by the investigators. Further, a multitude of evaluations, which were not always validated or reliable, were administered to assess participants' outcomes, even within the same field of breast health. The inconsistent features for comparison across these studies of breast models and health care professional education and assessment as well as lack of breast models reported for clinical lactation skills necessitate further discussion.
Quasi-experimental study design is commonly utilized across educational interventions, because randomized assignment to an experimental group is typically difficult or unethical due to the possible exclusion of learners to an intervention that could benefit their education. 40 Quasi-experimental design often induces selection bias, 41 particularly in the case of our reviewed sample, given that the learners are in training or experts within a self-selected health field. Developing interventions that allow for randomized groupings with a well-defined control group would alleviate bias and allow researchers to determine a clearer cause and effect relationship between the breast model intervention and learning or skill outcomes.
The use of different breast models within or across disciplines to learn skills that support breast health may result in variation of competence and clinical decision making among providers. Learning and practicing skills with different types of models could potentially lead to disparities of or inaccurate care. 14 This can further impact the communication or interpretation of care when health professionals of different areas of health must collaborate. 42 In this review, the reported interventions consisted of a breast model simulation conducted within one type of health profession, whereas simulations used in interprofessional education have evidenced their success in the development of collaborative and communication skills across disciplines that work in the same health area. 43 In addition to the varying breast models used across interventions, the assessments also differ. This disjunction brings into question the reliability of the standards expected of health professionals who are training in a breast health field.44,45 Future interventions should be designed based on evidence presented from validated and reliable breast models and associated assessments.
In our review, investigators that used low-fidelity or low-cost, investigator-developed models reported successful outcomes in the learners. As pointed out by Wang et al, this may be useful for institutions in developing countries where resources are limited. The preference for investigators to construct their own tabletop, low-fidelity breast models out of either turkey breasts or silicone does, however, underscore the lack of commercial breast models available for breast health simulations.
Although using low-fidelity models do show improvements in knowledge, learner satisfaction, and confidence, high-fidelity models that are realistic continue to be the gold standard.46,47 For example, the Medical Education Technologies Inc. (METI) Human Patient Simulators (HPS) are used as a teaching tool for medical students to experience trauma scenarios and develop essential medical skills like intubation. 48 The METI HPS are designed to resemble reality and complement multiple learning strategies that foster better retention of clinical knowledge in students. 49 Realistic models foster a progression in learning to a high level of competence that transfers to patient care and retainment of skills over time. 50 Investigators should explore cost-effective use of high-fidelity breast models, such as conducting interventions with a group of individuals rather than one-one-one training. 51
It has been established that there is a lack of hands-on learning of breastfeeding management skills in the education of health care professionals. 14 In this study, we identified only one article that reported using a model to support clinical lactation skills. 33 About 13% of women will be diagnosed with breast cancer over their lifetime, while 86% of women give birth, and of those, up to 92% have at least one concern with breastfeeding after birth. 52 Further, breastfeeding reduces maternal risk of maternal hypertension, type 2 diabetes, and ovarian cancer.53,54
The insufficient focus on and inclusion of breastfeeding skills in breast health education simulations speaks to a greater narrative of the lower priority for breastfeeding in promoting population health. 55 Furthermore, this presents a missed opportunity to support the development of skills needed across health professions that are critical to support mothers and are necessary to increase breastfeeding rates and duration. The success identified by Terzioğlu et al, (2016) in utilizing integrated simulations with standardized patients, wearable breast models, and real-life scenarios with patients demonstrates both the feasibility of including breastfeeding and clinical lactation education into health professional education and the measurable benefit in increasing provider confidence and communication skills.
The lack of reviewed studies in which investigators mentioned skin tone in their breast models is exemplary of the significant underrepresentation of racial diversity in simulation training 56 even though medical and nursing educators are encouraged to include diversity across simulation training.57,58 Simulation is well-documented to support the development of skills needed in real-life clinical scenarios; however, the lack of diverse skin tones is perpetuating systemic disparities in health care that lead to unequal treatments and outcomes for different racial and ethnic groups. Missed opportunities to be hands-on with a physical human breast with variation in skin color limits the educators' abilities to represent the full array of patients, conditions, and scenarios encountered in medicine and training and can lead to medical errors. 59 Initial diagnosis of breast cancer, in addition to clinical progression and treatment, is associated with skin color changes and dermatologic sequelae. 60
Limited exposure to patients and simulation models with different skin types may inhibit timely diagnosis of various breast cancers. When learners are only presented with white models, the retention rate of health profession trainees who are minorities is compromised. 61 Conversely, for example, when presented with a Black manikin and/or a Black preceptor, Black students are better able to connect with the learning experience and it fosters a sense of belonging to the health care field as a competent provider with the ability to provide care to diverse populations. 62 Better representation of various skin tones on realistic, high-fidelity breast models should be integrated into breast health education.
Limitations
We recognize some limitations to the design and interpretation of the studies evaluated in this literature review. First, the lack of consistency in validated or reliable evaluation tools and diverse use of breast models across different areas of breast health makes it difficult to compare the learner outcomes across the interventions. The final sample size of eighteen studies may not represent all types of breast model interventions utilized in health professional education to support breast health. In other words, interventions aimed to develop clinical skills to support breastfeeding, clinical breast exams, screening, or surgery that are incorporated into curricula or continued education may not be formally evaluated and formally disseminated for other health professional educators to understand their purpose, feasibility, and outcomes. Lastly, this review was conducted before evaluative studies that were published on the use of high-fidelity simulation clinical lactation and we believe the readership should be aware of these data.12,14,51
Conclusion
This work provides baseline information about the use of breast models in health profession education settings and demonstrates inconsistent evaluation and a need for consistent, reliable models that can be adopted across many settings. Even though it is clear the adequate breastfeeding rates will impact public health, there is still an obvious scarcity of interventions described in medicine or allied health professions for the development of clinical lactation skills. As breast models continue to be unrepresentative of the population (i.e., representation of skin tones), breast health care will continue to be inequitable across patients.
Footnotes
Acknowledgments
We would like to acknowledge Emily Ginier, a Senior Health Sciences Informationist at the University of Michigan for her consultation for our search strategy and Anna Sadovnikova for her feedback on the written article.
Authors' Contributions
C.F.M.: Conceptualization, Writing—original draft preparation, Data curation, Visualization; C.L.: Writing—original draft preparation, Data curation; B.G.: Writing—Resources, Review and editing; O.S.A.: Conceptualization, Writing—original draft preparation, Methodology, Validation.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.