
Abstract
Introduction:
The initiation of breastfeeding, exclusive breastfeeding, and its duration for 2 years in adolescent mothers is less than adult mothers. The purpose of this study is to determine the effect of supportive interventions on the initiation of breastfeeding, exclusive breastfeeding, and continuation of breastfeeding in adolescent mothers.
Methods:
Web of Science, PubMed, Scopus, Cochrane Library, EMBASE, ProQuest, SID, Iranmedex, and Google Scholar were searched to find English and Persian clinical trial studies without time limit. The Cochrane checklist was used to check the bias of the articles. Data analysis was done using STATA version 11. I-squared index was used to check the heterogeneity, and funnel plot and Begg test were used to examine the publication bias. The combined odds ratio (OR) and random effects model were used to combine the studies and perform meta-analysis.
Results:
Of 492 articles, 11 articles were entered to the systematic review. Of 11 articles, three articles were entered to the meta-analysis. The supportive interventions included educational and counseling interventions, home visit, and peer support. The results of the present random effects meta-analysis model showed that the combined OR was 3.38 with 95% confidence interval (1.66–6.88, p = 0.001), thus that, breastfeeding initiation in the intervention group was higher than the control group.
Conclusion:
Supportive interventions such as educational and counseling interventions, home visits, and peer support are suitable strategies to promote breastfeeding in adolescent mothers. Therefore, it is suggested to integrate these strategies in prenatal and postpartum care of adolescent mothers.
Introduction
The initiation of breastfeeding, exclusive breastfeeding, and its duration for 2 years in adolescent mothers is less than adult mothers.1–3 So, the World Health Organization (WHO) has announced breastfeeding of adolescent mothers as “Feeding in exceptionally difficult circumstances.” 4
Breast milk is the best source of food for mental, physical, and developmental needs of the child as if it is specifically designed for all the needs of infants and no other type of milk can completely substitute it.5,6 WHO recommends early initiation of breastfeeding in the first hour after birth and also exclusive breastfeeding until 6 months and continued breastfeeding with complementary foods for 2 years. Despite the recommendations of WHO, the vast majority of children around the world are not breastfed as recommended. Approximately 44% of infants are breastfed for 6 months and 45% of them are breastfed up to 2 years worldwide.4,5 The rate of breastfeeding among adolescent mothers is lower than the global average.7,8
Breastfeeding is the best nutrition for infants of adolescent mothers because their babies often face health problems such as premature birth, low birth weight, and intrauterine growth retardation, which could have short-term and long-term effects on infants' health.9–11 Breastfeeding can reduce the severity of these babies' health problems, as human milk contains antibodies, hormones, and enzymes that reduce infection, inflammation, and neurodevelopmental problems and supports the growth and development of babies.11–13
According to the searches of the research team, two systematic review studies have been conducted in the field of interventions on the breastfeeding of adolescent mothers and both of them were interventions conducted in high-income countries,14,15 therefore, it may not be generalizable to other countries with different support systems and social attitudes. However, in the present study, all the interventions performed on the breastfeeding of adolescent mothers with full-term newborns in high-, low-, and middle-income countries will be examined based on the inclusion criteria.
Considering the fact that the rate of initiation and duration of breastfeeding in adolescent mothers in different countries is low, it seems crucial to focus on this population. Because of these reasons, in previous studies, interventions such as home visits, peer support, and educational interventions for increasing the initiation of breastfeeding and exclusive breastfeeding have been conducted, but the results was conflicting.7,16,17
Systematic review and meta-analysis should be taken into account due to conflicting effects of different interventions on the initiation of breastfeeding, exclusive breastfeeding, breastfeeding duration in adolescent mothers, and also determining the most successful intervention to promote breastfeeding in this group of mothers.18,19 Therefore, the purpose of this systematic review and meta-analysis was to investigate the scope and effectiveness of interventions that are designed to increase the prevalence of breastfeeding, exclusive breastfeeding, and breastfeeding continuity among adolescent mothers in high-, low-, and middle-income countries.
Materials and Methods
Ethical Statement
The research project was confirmed by the Ethics Committee of Mashhad University of Medical Sciences, Mashhad, Iran, with the ethics code of IR.MUMS.NURSE.REC.1401.067.
This review study was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (Supplementary Material). 20 The Population Intervention Comparator Outcome Study Design (PICOS) criteria were used to design the review question and search terms: (P: Adolescent mothers with full-term infants (mothers aged 19 years or younger), I: any intervention, C: routine care, O: increasing initiate, exclusive breastfeeding rates, and duration of breastfeeding, S: randomized controlled trials).
Data sources, search strategy
In this meta-analysis, the databases of Web of Science, PubMed, Scopus, Cochrane Library, EMBASE, ProQuest, SID, Iranmedex, and Google Scholar were searched by two researchers independently for published articles in English and Persian language until June 23, 2022. Date limitations were not applied to the search. The keywords used for the search included a combination of the following words or their equivalents from MESH, which were combined with AND and OR: breastfeeding, lactation, adolescent mothers, teen mothers, exclusive breastfeeding, infant feeding, young mothers, and randomized clinical trial, Intervention. All the mentioned databases were manually searched to retrieve the articles using relevant keywords. In addition, reference sections of relevant trials were manually checked to recognize further trials missed by electronic search.
Eligibility criteria
The inclusion criteria included clinical trial studies that investigated the effect of supportive interventions on initiation of breastfeeding, exclusive breastfeeding, or continuation of breastfeeding in mothers younger than 19 years of age with full-term infants and were published in Persian or English language. Exclusion criteria included case report studies, review studies, letters to the editor, systematic review studies, nonrandomized clinical trials, observational study designs, and studies with unrelated data.
Study selection and data collection process
Studies identified through the electronic databases were sent out to Endnote X8 for evacuating duplicates, screening, and determination. 21 Two researchers (A.Y. and F.Z.K.) autonomously screened the articles based on the consideration criteria. Full texts of the articles that met the consideration criteria were autonomously surveyed by two researchers (A.Y. and F.Z.K.) and any disagreements were resolved through discussion with a third researcher (T.K.). The search strategy led to the selection of 11 studies for review. This process is summarized in the PRISMA flowchart (Fig. 1).
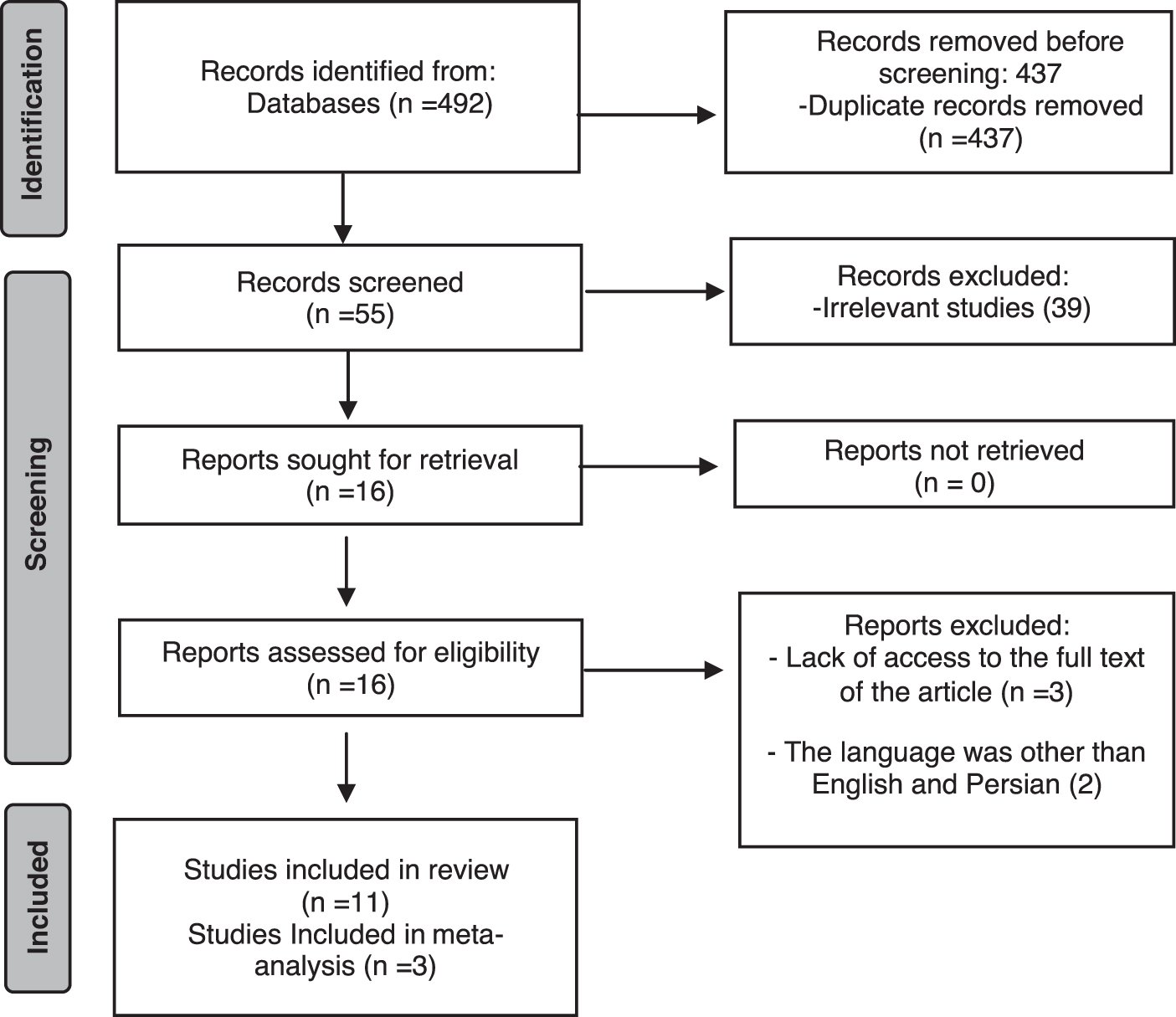
PRISMA 2020 flow diagram of the studies identified in the systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analysis.
Extracted data included name of the first author, year of publication, country, type of study, sample size, type of intervention, comparison group, sample attrition, and conclusion (Table 1). Data extraction was done by two researchers (A.Y. and F.Z.K.) independently. T.K. provided feedback and solution for any disagreements.
Characteristics of 12 Clinical Trials Included in Study
EXCEL, Early Experiences and Counseling for Effective Lactation; RCT, Randomized Clinical Trial; WHO, World Health Organization.
Risk of bias (quality) assessment
The risk of bias was examined for each study by two independent evaluators (A.Y. and F.Z.K.) using the Cochrane Collaboration's tool. In the event of a disagreement between the two evaluators, the issue would be resolved by a third researcher T.K. Using the mentioned tool, six types of biases were assessed, including selection bias (random sequence generation and allocation concealment), performance bias (examining the blinding of participants and personnel), detection bias (the blinding of outcome assessors), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other sources of biases. 22 Based on the degree of each type of bias, the studies were assessed and reported with low, high, and uncertain risks (Figs. 2 and 3).

Author's judgments of risk of bias items for each study included.
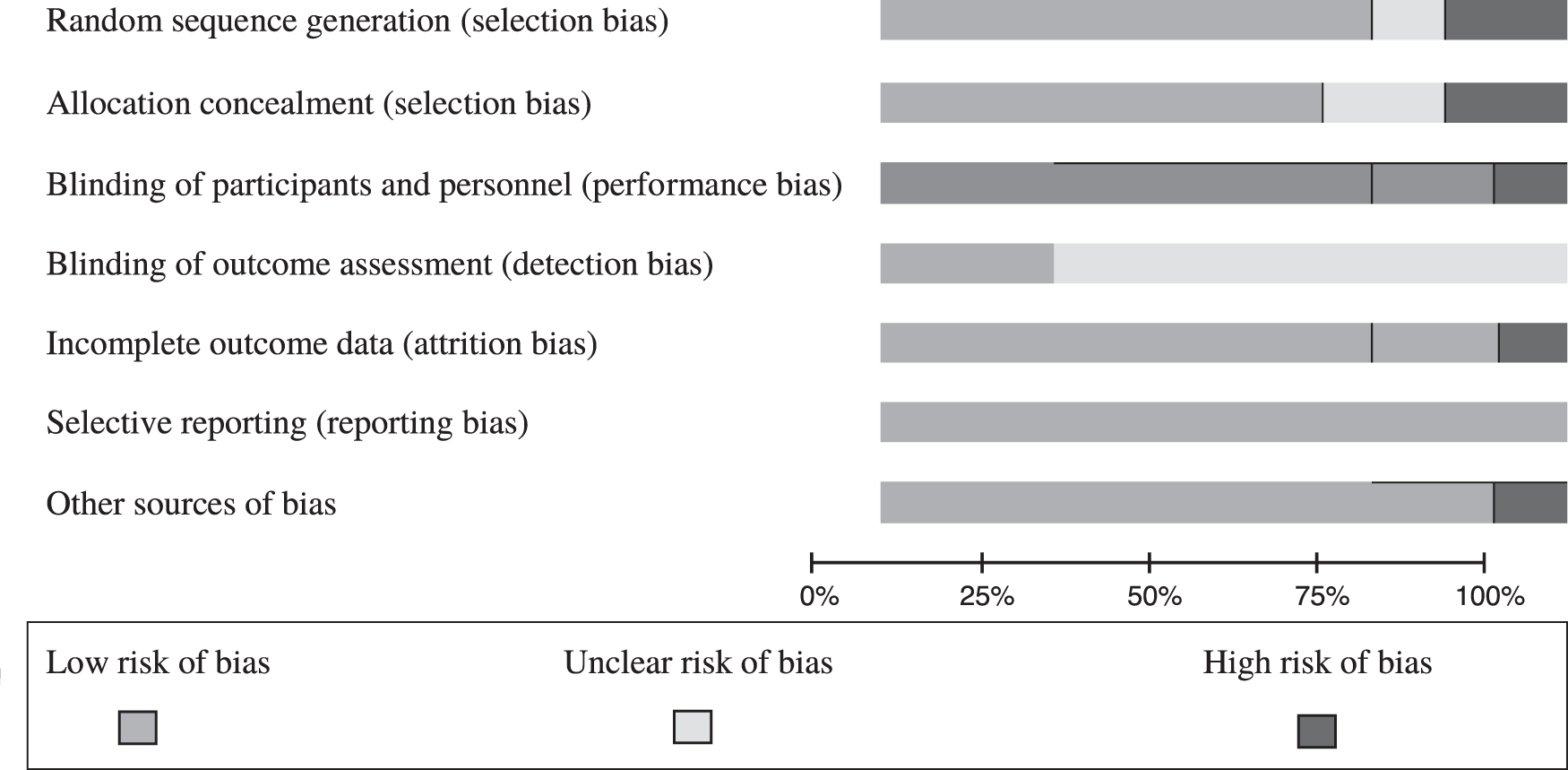
Authors' judgments of risk of bias presented as percentages across all included studies.
Data synthesis
The data analyzed using STATA version 11. To combine the results of the studies, combined OR was used. For checking the homogeneity of the studies, I-squared index was used. I-squared index less than 0.25 indicates low heterogeneity, between 0.25 and 0.75 indicates moderate heterogeneity, and more than 0.75 indicates high heterogeneity. If there was heterogeneity in the studies, random effects model was used. Also, funnel plot and Begg test were used to assessing publication bias. p < 0.05 was considered significant.
Result
From a total of 492 articles obtained through databases, 11 articles were systematically reviewed. In these articles, a total of 1282 participants were examined in the intervention group and 1214 participants in the control group. Five articles were conducted in United States,8,17,23–25 four articles in Brazil,7,26–28 one article in Canada, 16 and one article in Colombia. 29 The publication date ranges from 1988 to 2021. The range of sample size in the studies varied from 78 to 407. All mothers participating in the studies were younger than the age of 19 years. In all studies, there was no statistically significant difference between the intervention and control groups in terms of sociodemographic characteristics before starting the interventions. The interventions included educational and counseling interventions,17,25,29 home visit,7,23,26–28 peer support,8,16 and gift pack. 24 The follow-up period in the reviewed studies was between 3 months and 2 years.
Peer support
In the present research, two studies included peer support intervention.8,16 In 2010, Meglio et al designed a clinical trial study that included peer support. These people were adolescent mothers who had a history of breastfeeding and were trained to provide the necessary support during breastfeeding to their peers. On days 2, 4, and 7 after discharge, and then on weeks 2, 3, 4, and 5 after discharge, the support peers called the new adolescent mothers and gave them telephone counseling about breastfeeding problems. 16
In 2011, Wambach conducted a clinical trial that the intervention was consisted of breastfeeding education and counseling based on the theory of planned behavior and developmental theory that were provided by peer counselors. Intervention was presented face to face in the hospital (during the hospitalization of teenage mothers for childbirth) to start breastfeeding and also after delivery by phone on days 4, 7, 11, and 18 for those participants in the intervention group who had started breastfeeding. 8
Home visit
Bica et al 26 designed a clinical trial study that included breastfeeding counseling sessions based on the principles recommended by the WHO for adolescent mothers who lived alone or with their mothers. The interventions were implemented by individuals who had received the necessary training on breastfeeding counseling. The first intervention session was conducted in the maternity ward, 24–72 hours after delivery for adolescent mothers. The next meetings were held as home visits on days 7, 15, 30, 60, and 120 for adolescent mothers and grandmothers. During each session, adolescent mothers expressed their experiences and beliefs about breastfeeding through structured conversations. In the sessions, the discussions were mainly about infant feeding, the importance and duration of exclusive feeding. The positive effect of systematic counseling sessions on the initiation of breastfeeding in the first year of life was significant for adolescent mothers, but living with their mothers (grandmothers) reduced such an effect. 26
Black et al 23 designed a clinical trial study, in which the intervention consisted of a home visit accompanied by a videotape. The videotape was developed by a consultative group of black teenage mothers focusing on three main subjects: (1) recognizing infant cues; (2) nonfood strategies to manage infant behavior; and (3) the strategies to negotiate with grandmothers. The mothers of the intervention group received home visits once a week for 1 year after delivery. The people who attended the home visits were educated black women who received 40 hours of training and counseling.
On the first day of the home visit-based intervention, the videotape was shown to each adolescent mother and she received a copy of the videotape to share and discuss with friends and family. The home visitor used the videotape to create discussions and skill-oriented activities about infant feeding, and in subsequent visits, they addressed breastfeeding and child development problems and gave mothers the necessary training and advice. 23
In clinical trials conducted by Oliveira et al, 7 Nunes et al, 27 and Silva et al, 28 the adolescent mothers of the intervention group received a counseling and educational sessions about breastfeeding in the hospital after delivery, and the next five sessions were held as home visits by breastfeeding specialists. In the study conducted by Oliveira et al, 7 mothers who lived with grandmothers received breastfeeding counseling and information about the appropriate time to introduce complementary foods (at 6 months), foods that should be offered or avoided, and how they should be presented.
The presence of grandmothers did not have an effect on the time of the introduction of complementary foods, either in the control group or in the intervention group. 7 In the study done by Nunes et al, intervention group mothers who lived with grandmothers received counseling sessions and home visits together, and compared to mothers who lived alone, they gave less unnecessary water and tea to babies in the first 6 months. 27
Gift pack
Neifert et al designed a trial study in 1988 that the intervention consisted of a gift pack for adolescent mothers that included six commercial breast pads, a bubble suction breast pump that discharges into a jar, lanolin cream, infant vitamins, and a breastfeeding pamphlet. 24
Counseling and educational interventions
Poboci et al designed a clinical trial study in 2000 that included breastfeeding education and counseling program called EXCEL (Early Experiences and Counseling for Effective Lactation), which was formed during pregnancy and it included eight 45-minute group sessions. The EXCEL program includes (1) benefits of breastfeeding, (2) initiation of breastfeeding, (3) success in breastfeeding, (4) appropriate weight gain during pregnancy, (5) iron and folate during pregnancy, (6) the need for calcium during pregnancy is reduced, (7) risk of mother's chronic disease, and (8) the risk of taking drug during pregnancy. For the members of the intervention group, group classes were organized either in high school or in Women, Infants, and Children (WIC) clinics, and after delivery, home visits and education or telephone counseling related to breastfeeding would be conducted if the adolescent mothers asked. 17
In the clinical trial study conducted by Sabogal et al, 29 adolescent mothers in the intervention group were given breastfeeding counseling for four sessions by trained nurses. The intervention started during pregnancy. The frequency of each session was weekly and between 45 and 60 minutes. Each session consisted of three parts: introducing the topic, developing the topic using PowerPoint presentation, audio-visual materials such as photos and videos, and examining the main topic related to breastfeeding. 29 Volpe and Bear 25 designed a clinical trial study, in which teenage mothers were subjected to an educational and counseling intervention.
The intervention consisted of three weekly 1 hour sessions that began during pregnancy. This intervention used role-playing and games to teach adolescent mothers about the principles of breastfeeding in a nonthreatening and nonjudgmental way. This program not only focuses on breastfeeding, but also addresses other mother and child issues, including nutrition, safety, child development, and preventive health care. 25
It should be noted that in the studies done by Bica et al, 26 Oliveira et al, 7 and Nunes et al, 27 adolescent mothers who lived with their mothers received the interventions together.
Adolescent fertility rate (births per 1,000 women ages 15–19) in United States is 16, in Canada is 7, in Colombia is 63, and in Brazil is 55. 30 The rate of breastfeeding in adolescent mothers in the countries that were investigated includes mothers in the United States aged 30 years or older who were more than twice as likely, compared with mothers 20 years or younger, to exclusively breastfeed to 6 months (18.0% vs. 8.3%). 31 The prevalence of exclusive breastfeeding in adolescent from Brazil ranged from 47.8% in the first month of life up to 13.8% after 6 months period. 32 In Canada, at 6 months postpartum, 22% of adolescent mothers report any breastfeeding. In comparison, 6-month duration rates among slightly older mothers (20–24 years) was higher at 37.1% and mothers older than 25 years were the most successful with continued breastfeeding to 6 months, with rates between 51.3% and 69.7%. 33
Risk of bias assessment
One of the studies included in the current research was a protocol design and the results were not reported in the article, therefore, attrition bias, reporting bias, and other sources of bias were not judged. 29 Of the 11 studies reviewed for random sequence generation, they were low risk and 6 of the studies were low risk for allocation concealment. Due to the nature of the interventions, blinding of participants could not be done in most of the studies and could only be implemented in one study that was not done. 24 Blinding of outcome assessments was not reported in most studies. Only one study was high risk for attrition bias. 23 All studies were low risk for reporting bias and one study was high risk for other sources of bias. 8
Meta-analysis
Three studies were included in the meta-analysis. In two studies, educational and counseling interventions17,25 and in one study, peer support intervention 8 were done. Initiation of breastfeeding was reported in all three studies and analyzed.
The results of the meta-analysis showed that in based on I-squared index, there was heterogeneity in the studies (I 2 = 0.94). Therefore random effects model was used to combine the studies and final estimate of the studies. To the random effects method results, there was a significant difference between the control and intervention groups in initiation of breastfeeding (p = 0.001). The odds ratio (OR) was 3.38 with 95% confidence interval (CI) 1.66–6.88 (Fig. 4). For more investigation, Galbraith graph was drawn (Fig. 5). The results of Galbraith graph showed that some of the studies are out of the range and they may cause heterogeneity.

The effect of supportive interventions on initiation of breastfeeding.

Galbraith plot.
To assess the robustness of the studies, sensitive analysis was used (Fig. 6). The results of the sensitive analysis in graph 6 showed that after removing every study, the estimation of OR was within the combined CI (1.66–6.88). Thus, the results were robust and the odds of initiation of breastfeeding in the intervention group were higher than the control group. Also, the results of Begg test showed no publication bias in the studies (p = 0.023).
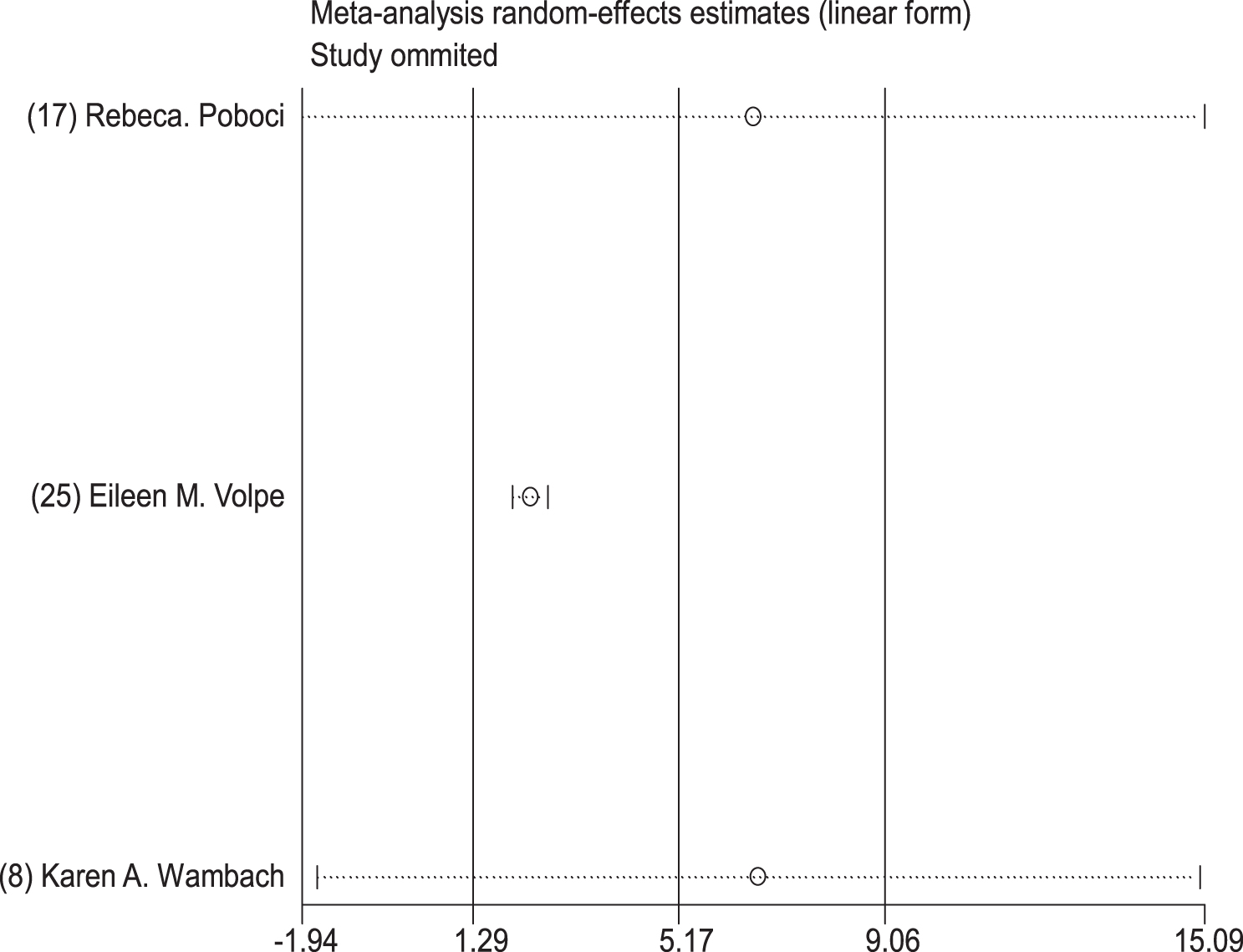
Sensitivity analysis plot.
Discussion
The present systematic review and meta-analysis were conducted with the aim of determining the impact of supportive interventions on initiation of breastfeeding, exclusive breastfeeding, and continuation of breastfeeding in adolescent mothers. According to the results of the present study, supportive interventions such as educational and counseling interventions, home visits, and peer support lead to promoting the initiation of breastfeeding, exclusive breastfeeding, and duration of breastfeeding in this group of mothers. In the study carried out by Volpe and Bear, 25 the initiation of breastfeeding in the adolescent mothers who were subjected to educational and counseling intervention was significantly higher than the mothers in the intervention group. 25 In Sabogal et al's study, the counseling and educational interventions related to breastfeeding caused a significant increase in the amount of exclusive breastfeeding in adolescent mothers of the intervention group. 29
In the study done by Poboci et al, the initiation of breastfeeding and the duration of breastfeeding in adolescent mothers who received breastfeeding counseling were significantly higher than mothers in the control group. 17 In the aforementioned three studies, educational and counseling interventions were used as the main strategy, in the other four studies, which include the studies done by Oliveir et al, 7 Bica et al, 26 Nunes et al, 27 and Silva et al, 28 educational and counseling interventions were used simultaneously with home visits, the results of these studies also showed that educational and counseling interventions at the same time as home visits lead to a later start of complementary feeding. The duration of breastfeeding up to 1 year of age in adolescent mothers of the intervention group is increased compared to the control group.26,28
In addition, educational and counseling interventions related to breastfeeding are an effective strategy to ensure the proper breastfeeding technique, help mothers adapt to the physical changes during breastfeeding, solve breastfeeding problems, and improve their self-confidence to successfully breastfeed.34,35 Home visits, which are defined as the provision of specialized nursing and midwifery care services at home, are a suitable solution for providing the necessary supportive care related to breastfeeding to mothers. 36
In 2015, Sipsma et al done a systematic review with the aim of determining the interventions that were carried out to promote breastfeeding in mothers younger than 22 years of age in high-income countries showed that most of the interventions done to promote exclusive breastfeeding and initiation of breastfeeding are not effective in adolescent mothers. They concluded that more and more diverse interventions are needed to influence the breastfeeding of adolescent mothers and the interventions should be more theoretically guided and specifically include mothers and their partners to successfully promote breastfeeding. 14 The results of the study by Sipsma et al 14 on choosing effective interventions to promote breastfeeding in young mothers are different from the results of the present study.
The reason for the inconsistency of the results can be due to the older age of the mothers examined in Heather's study, so the mothers younger than 22 years of age were also examined, while in the present study, all the mothers examined were younger than 19 years of age. Also, the current research has examined all clinical trial interventions conducted around the world, but in Heather's study, only interventions conducted in high-income countries have been examined.
The results of a systematic review and meta-analysis by Buckland et al, 15 which examined interventions to increase the amount of exclusive breastfeeding among young mothers in the 17–24 age group in high-income countries, represent peer counseling as the most promising strategy associated with higher rates of exclusive breastfeeding among young mothers. Moreover, they concluded that few interventions have been carried out with the aim of promoting breastfeeding in young mothers, thus young mothers should be specifically targeted in interventional studies related to breastfeeding. 15
In the current study, peer support in the study by Wambach et al 8 caused a significant increase in the duration of breastfeeding, but did not affect the rate of initiation of breastfeeding or the rate of exclusive breastfeeding, and in the study by Meglio et al, 16 it caused an increase in the duration of breastfeeding. Peer support, which refers to the support provided by a nonprofessional individual from the community who has a personal experience of breastfeeding and a desire to support others, can provide mothers with the necessary guidance related to successful breastfeeding and can effectively promote breastfeeding of mothers. 37
According to the features and characteristics of adolescence, in which the person's behavior is more influenced by the environment, and since some adolescent mothers live with their mothers, their breastfeeding behaviors may be influenced by their mothers' breastfeeding beliefs and orders. The grandmothers' breastfeeding teachings and beliefs may promote breastfeeding behavior in adolescent mothers or lead to inducing wrong breastfeeding behaviors.38,39 In this regard, in the studies of Bica et al, 26 Oliveira et al, 7 and Nunes et al, 27 adolescent mothers who live with their mothers received breastfeeding interventions together.
In 2014, a study was carried out by Bica et al, 26 counseling interventions and home visits were presented together for adolescent mothers who lived with grandmothers, and the results of the study showed that the continuation of breastfeeding up to 12 months was significantly more in the adolescent mothers of the group of intervention who lived alone in comparison with the mothers of the control group who lived alone. 26 In the study conducted by Oliveira et al, 7 adolescent mothers' lives with grandmothers did not have an effect on the time of introducing complementary foods in the intervention and control groups.
Nunes et al conducted a study in 2011, in which counseling intervention and home visits were offered jointly to mothers who lived with grandmothers, and the results of the study indicated that adolescent mothers who live with grandmothers gave less unnecessary tea or water to their child. 27
In the present study, three studies that provided educational and counseling interventions and peer support about initiate breastfeeding were included in the meta-analysis, and the results of the meta-analysis showed that these interventions caused a significant increase in the rate of initiation of breastfeeding in mothers of the intervention group compared to the mothers of the control group.8,17,25 According to the amount of OR (95% CI) in the articles that were subjected to meta-analysis, the Volpe and Bear's 25 with 10.93 (3.95–30.25) has the largest effect size, which presented the counseling educational intervention and then Poboci et al 17 2.44 (1.60–3.73) with educational and counseling intervention and Wambach et al's 8 2.24 (1.29–3.91) with peer support intervention have the largest effect. Therefore, it can be said that educational and counseling interventions are particularly important in increasing the initiation of breastfeeding in teenage mothers.
The present study is the first meta-analysis study which evaluates the clinical trial interventions conducted around the world according to specific entry criteria, which is one of the main strengths of the present study.
One of the limitations of the present study was that the studies included in this systematic review were mostly conducted in the United States of United States and Brazil and high-income countries, and therefore, it may not be generalizable to other countries with different support systems and social attitudes. In addition, in the present study, eight studies that investigated supportive interventions in exclusive breastfeeding and duration of breastfeeding were excluded from the meta-analysis due to the lack of reporting the mean and standard deviation as well as the high heterogeneity of the studies. In the present study, only the data related to the initiation of breastfeeding were included in the quantitative analysis.
Conclusion
According to the results of the present study, supportive interventions such as educational and counseling interventions related to breastfeeding, peer support, and home visits could be considered as suitable strategies for initiation of breastfeeding, exclusive breastfeeding, and duration of breastfeeding in adolescent mothers. Therefore, it is suggested that health care providers and health systems in developed and developing countries use the mentioned interventions to increase the rate of breastfeeding in adolescent mothers, and these strategies should be integrated in the care related to pregnancy, delivery, and after delivery of this group of mothers. Health care providers in high-, low-, and middle-income countries can use educational and counseling interventions, home visits, and peer support according to the facilities of their country's health system and the level of breastfeeding problems of adolescent mothers and the extent of their cooperation.
The results of the present study showed that these interventions can improve at least one of the stages of breastfeeding in adolescent mothers (initiation, continuation, and exclusive breastfeeding). It seems that the combination of interventions according to the facilities of each country's health system will be useful in promoting breastfeeding among adolescent mothers. In some studies, the combination of two types of support interventions such as educational and counseling interventions and home visit have been used, which had effective results in promoting breastfeeding in adolescent mothers. In future studies, in addition to adolescent mothers, grandmothers should also be addressed because according to the available evidence, social support network members may affect the ability of adolescent mothers to breastfeed successfully.3,40 It is also suggested to conduct similar clinical trials with higher quality methodologies to obtain stronger evidence in high-, low-, and middle-income countries.
It should be noted that all authors are supported by Mashhad University of Medical Science or Torbat Heydarieh University of Medical Sciences which are active in the field of medical education and research.
Footnotes
Acknowledgment
We thank the authors whose articles were reviewed in this research.
Authors' Contributions
F.Z.K. and T.K.: review and editing, data extraction, and formal analysis. A.Y.: writing—original draft, formal analysis, writing and editing, and data extraction. M.A.: meta-analysis.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.