
Abstract
Background:
Living in fluoride-endemic areas and the inevitable use of groundwater for consumption have imposed children at high risk of dental fluorosis. To mitigate exposure to excessive fluoride at age of developing dentition, breastfeeding might serve as a natural public health intervention against dental fluorosis in that socially disadvantaged context.
Objective:
This study aimed to evaluate the preventive effect of breastfeeding against dental fluorosis in children living in fluoride-endemic areas in Nakhon Pathom Province, Thailand. Evaluation of the association through several epidemiological models depicted by a directed acyclic graph (DAG) was undertaken.
Methods:
A case–control study of 127 cases of dental fluorosis and 85 controls was conducted. Independent factor of breastfeeding, along with other past exposure variables, were traced backwardly since infancy by caregiver history taking. Fluoride concentrations in groundwater utilized for household supply matching to residence and number of years by age of each child were collected from 2008 to 2015. Multivariable Poisson regression with robust standard errors was sequentially executed to estimate prevalence ratio (PR) according to models in DAG.
Results:
Breastfeeding was significantly higher (95.3%) among controls compared to cases (84.2%), p = 0.014. Contrastingly, prevalence of using toothpaste larger than pea-sized and having fluoride ≥1.5 ppm in household water supply was higher among cases. Univariable and subsequent five multivariable regression models according to DAG consistently unveiled significant protective effect of breastfeeding on dental fluorosis with PR ranging from 0.66 to 0.75.
Conclusions:
Breastfeeding for at least 6 months had preventive effect against dental fluorosis among children living in fluoride-endemic areas.
Introduction
Dental fluorosis is a dental condition that varies in manifestations ranging from an initial mild form of opaque white discoloration that is irregularly scattered on the dental enamel surface to a more severe form of pitted and corroded enamel with apparent brown stains. 1 The condition that persists on permanent teeth can cause esthetic concerns2,3 and, in severe cases, physical damage to the dental enamel that may necessitate restoration.4,5 Dental fluorosis arises as a result of excessive fluoride consumption and accumulation over time, which occurs during tooth development.6,7 In general, the critical period in which permanent teeth are susceptible to chronic fluoride toxicity causing dental fluorosis is under 8 years old. 8 Nonetheless, in the case of maxillary incisors or the upper anterior teeth that are the most vital to dental esthetics, the critically susceptible period for dental fluorosis is within the first 2 years of life. 9
Several public health strategies have been proposed to mitigate the risk of this waterborne disease in children. These strategies comprise of identifying and utilizing alternative safe water sources, bringing in safe water from locations outside fluoride-endemic areas, rainwater collection, and defluoridation to remove fluoride from water using appropriate techniques such as reverse osmosis.10–13 Nonetheless, implementation of these strategies in fluoride-endemic and socially-disadvantaged communities may not be practical. 13 For instance, delivering clean water from distant locations to serve an entire community typically relies on the local government budget to invest in infrastructure and maintenance of public water irrigation systems which can be challenging in a resource-constrained setting. 14
Unlike other strategies, breastfeeding has been suggested as a natural approach feasible to minimize the risk of dental fluorosis. 15 According to physiological research, the transferability of fluoride from plasma into the breast milk was found limited and resulted in a low content of 0.005–0.01 mg/L of fluoride in breast milk.16,17 Fluoride levels in breast milk were only marginally elevated, and children's fluoride intake through breastfeeding was relatively low regardless of high fluoride consumption in mothers. 18 In addition, a breastfeeding period that naturally coincides with the susceptible period of dental fluorosis, particularly in the first 2 years of life, 9 may effectively lower the risk of high fluoride exposure from using infant formula mixed with fluoride-contaminated water.17,19 Breastfeeding itself is also cost-free and may be a practical public health intervention to control dental fluorosis in children even in the challenging context of socially-disadvantaged communities located in fluoride-endemic areas with limited access to safe water sources.
Nonetheless, the majority of previous epidemiological studies suggesting the beneficial effect of breastfeeding on dental fluorosis were of cross-sectional design.19–22 Investigation using analytical designs capable of determining the temporal relationship between breastfeeding and dental fluorosis is needed. In addition, the novel epidemiological approach of using a directed acyclic graph (DAG) to visualize prior knowledge about biological and sociobehavioral systems concerning a specific causal research question 23 could potentially improve understanding of the various roles of explanatory factors (e.g., confounder and collider) influencing the occurrence of dental fluorosis. 14 However, the application of DAG to assess the effect of breastfeeding on dental fluorosis is still lacking. This study therefore aimed to evaluate the effect of breastfeeding on dental fluorosis in children living in fluoride-endemic areas in Nakhon Pathom Province, Thailand. Evaluation of the association through several epidemiological models depicted by a DAG was undertaken.
Methods
Study design and participants
This community-based case–control study was conducted in Bang Len District, Nakhon Pathom Province, Thailand in 2015, to evaluate the association between breastfeeding and dental fluorosis among children living in rural agrarian villages located in fluoride-endemic areas. Five subdistricts selected for this study were Bang Luang, Bang Sai Pa, Hin Mun, Nin Phet, and Sai Ngam. These study areas shared similar characteristics of (1) being areas predominantly focused on rice agriculture, (2) residents having low family income per month compared to the provincial average, (3) having village water sources containing natural fluoride that could exceed a local safety threshold of 0.7 ppm, (4) lacking access to standard water irrigation system provided by the Provincial Waterworks Authority (PWA), and (5) utilizing untreated groundwater from community wells for household consumption.
Participating children who were assessed for dental fluorosis were first and second graders enrolled in 11 primary schools located in the study areas. Permission to conduct this study was obtained from all schools along with written consent from each child's caregiver. During the in-school oral examination, no child opted out of participation. The participating children's mothers were contacted in person to obtain written consent to be interviewed regarding their breastfeeding history and other explanatory variables. Ethical approval was obtained from the Human Research Ethics Committee, Department of Health, Ministry of Public Health, Thailand (project no. 116). Permission of mothers and the consent of the children were obtained.
Study size
To evaluate the association between breastfeeding and dental fluorosis using the unmatched case–control design, the study size was estimated according to the method described by Fleiss. 24 The study size of 137 cases and 137 controls was estimated to have a two-sided confidence level (1-alpha) of 95, 80% statistical power, 1:1 ratio of controls to cases, the hypothetical proportion of controls with exposure or breastfeeding proportion among controls of 0.5, and an estimated effect measure of 0.5.
Outcome measurement
Dental fluorosis outcome was measured during the regular school-based dental checkup. An authorized dental officer from Nakhon Pathom Provincial Public Health Office—also an author (A.S.)—contacted school principals to inform them about the checkup program and obtain permission with assistance from local public health officers in Bang Len District. Informed consent forms were distributed to and collected back from caregivers of grade 1 and 2 students by the teachers. The National Oral Health Survey's standard oral examination protocol was adopted. 25 Outcome assessment in all children was carried out by one dentist—also an author (PN) —from Nakhon Pathom Provincial Public Health Office who underwent intra-examiner calibration with a result of nearly perfect agreement indicated by Kappa statistics of 0.9. The severity of dental fluorosis was assessed according to Dean's index. 1 In this study, cases included children with very mild to severe dental fluorosis, while controls were the counterparts.
Exposure measurement
The main exposure was breastfeeding for at least 6 months. Other explanatory variables were time-average fluoride concentration in household water sources, caregiver's socioeconomic factors (caregiver's education and family income sufficiency), child's characteristics (child's natal sex and age), and child's oral hygiene practice (tooth brushing frequency, brushing before bed, and fluoride toothpaste use). The explanatory variables for each child were traced back to birth. Data for all explanatory variables, except for the time-average fluoride concentration, were collected through in-person interviews with the children's caregivers using a structured questionnaire.
Breastfeeding was evaluated through a yes/no question of whether the child was breastfed for at least 6 months. Continuous data on family income per month, in Thai Bahts (THB), were collected before being transformed into a binary variable of income sufficiency. Using the average family spending per month in 2015 in Nakhon Pathom Province of 26,025 THB as a cut point, income sufficiency was defined as having family income per month ≥ the cut point. Tooth brushing frequency was assessed as times per day and for two periods, including before and at ≥2 years old, according to the susceptible period for dental fluorosis development in anterior permanent teeth. 9
To obtain the time-average fluoride concentration data, the database from 2008 to 2015 at Nakhon Pathom Provincial Public Health Office was initially accessed to extract yearly records of fluoride concentration (parts per million, ppm) in water used for household consumption relevant to each child's address and age—all years from birth, before averaging the concentrations by age. The time-average fluoride concentration was later transformed into a polytomous variable having three categories of concentrations comprising <0.7, 0.7–1.49, and ≥1.5 ppm. The first cut point of 0.7 ppm was specified according to the local recommendation of <0.7 ppm fluoride in drinking water. 26 The second cut point of 1.5 ppm was specified according to the World Health Organization's recommendation of <1.5 ppm in drinking water. 27
Statistical analysis
Descriptive statistics was used to summarize the characteristics of caregivers and children. For comparison between cases and controls, independent samples t-test was used to compare means for continuous variables. When the normal distribution of data could not be assumed for the t-test, the two-sample Wilcoxon rank-sum test was instead applied. Exact probability test was used to assess the difference in proportions. To evaluate the crude and adjusted effect of breastfeeding on dental fluorosis, univariable and multivariable Poisson regression with robust standard errors was applied to estimate the dental fluorosis prevalence ratio (PR). The approach was used instead of binary logistic regression to prevent the overestimation of effect by odds ratio when the outcome of dental fluorosis in the fluoride-endemic areas under investigation was expected to be relatively common. 28 Epidemiological models depicted by DAG (Fig. 1) guided the sequential execution of the multivariable regression analyses.
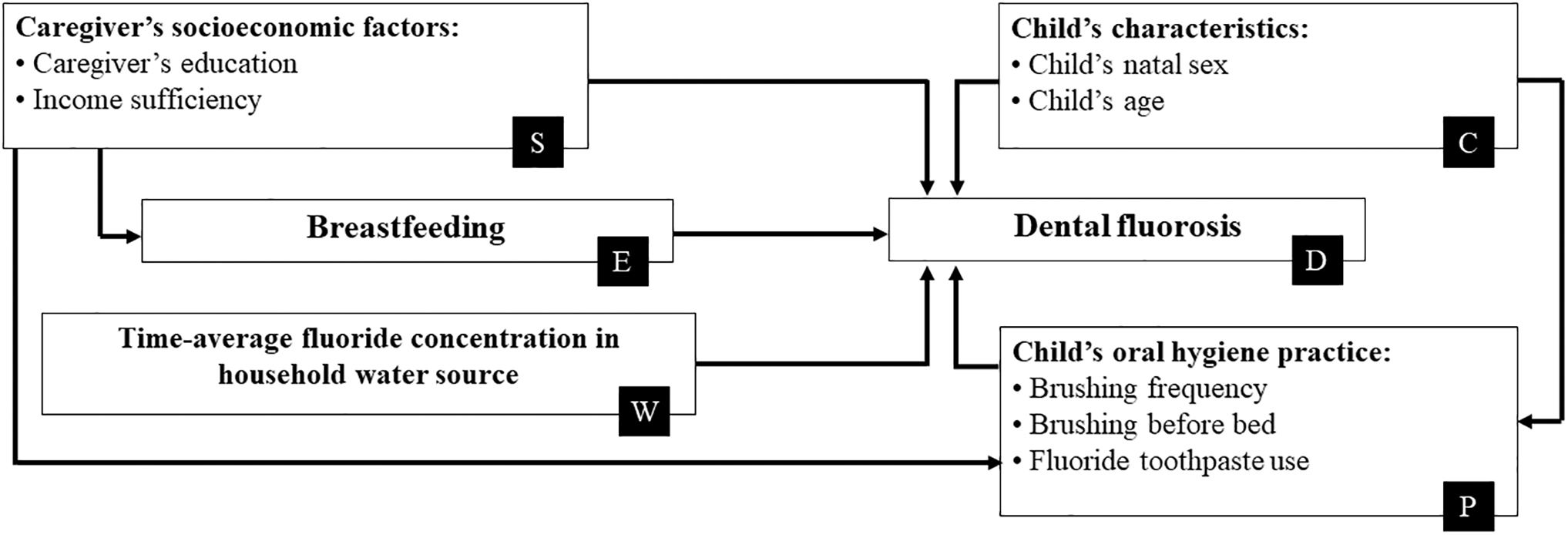
Statistical models according to different paths of DAG. Model 1: unadjusted model of breastfeeding (E) and dental fluorosis (D): E → D. Model 2: model of breastfeeding (E) and dental fluorosis (D) adjusted for caregiver's socioeconomic factors (S): E ← S → D. Model 3: model of breastfeeding (E) and dental fluorosis (D) adjusted for caregiver's socioeconomic factors (S), child's characteristics (C), and omit conditioning on child's oral hygiene practice (P) or collider: E ← S → P ← C → D. Model 4: Model of breastfeeding (E) and dental fluorosis (D) adjusted for child's oral hygiene practice (P): E ← S → P → D. Model 5: Model of breastfeeding (E) and dental fluorosis (D) adjusted for time-average fluoride concentration in household water source (W). Model 6. Model 3 with additional adjustment for the time-average fluoride concentration in household water source. DAG, directed acyclic graph.
Results
Among all 212 children, 127 of them had dental fluorosis and were regarded as cases, while 85 children without the outcome served as controls. Among the cases, the severity of dental fluorosis ranged from very mild to moderate levels. No severe dental fluorosis was identified. The proportion of no breastfeeding was significantly higher among cases (15.8%) compared to that of the controls (4.7%). About 44.3% of the caregivers in the controls reported having no schooling, while the proportion was higher among caregivers of the cases. The proportions of the families having sufficient income per month were very low in both groups. The proportion of children using toothpaste sizes larger than the pea-sized amount was significantly higher among cases (55.7%). The median of the time-averaged fluoride concentrations in household water sources was significantly higher among the cases (2 ppm). A greater proportion of the cases, 84.2%, resided in areas of high time-averaged fluoride concentrations (≥1.5 ppm) compared to 56.5% in the controls (Table 1).
Characteristics of Study Participants
Percentage by column.
Percentage by row.
Exact probability test.
Independent samples t-test.
Two-samples Wilcoxon rank-sum test.
Average family expenditure per month in 2015, Nakhon Pathom, Thailand.
For each child, available measures of groundwater fluoride concentrations in drinking water sources supplying the child's residence were time averaged over the period of birth to the study.
IQR, interquartile range; Min., minimum; Max., maximum; ppm, parts per million; SD, standard deviation; THB, Thai Bahts; USD, US Dollar.
Univariable analysis by Poisson regression with robust standard errors revealed crude estimates of the PR illustrated in Table 2. Regarding the main exposure of breastfeeding, the prevalence of dental fluorosis among the children who were breastfed was 0.68 times the prevalence among those whose mothers did not breastfeed. The prevalence of dental fluorosis was significantly higher among children who used toothpaste larger than a pea-sized amount. The prevalence of dental fluorosis among children with time-averaged fluoride concentrations in household water sources of ≥1.5 ppm was 1.97 times the prevalence among those living with fluoride concentrations <1.5 ppm.
Univariable Analysis of Association Between Each Explanatory Variable and Dental Fluorosis
Univariable model estimated by Poisson regression with robust standard error.
Row percentage is presented to comply with analysis of PR.
Average family expenditure per month in 2015, Nakhon Pathom, Thailand.
For each child, available measures of groundwater fluoride concentrations in drinking water sources supplying the child's residence were time averaged over the period of birth to the study.
CI, confidence interval; ppm, parts per million; PR, prevalence ratio; THB, Thai Bahts; USD, US Dollar.
The multivariable analyses of the association between breastfeeding and dental fluorosis in children using Poisson regression with robust standard errors adjusting for covariates revealed results in Table 3. The models compared the prevalence of dental fluorosis in the index category of children with mothers who breastfed compared to those in the reference category whose mothers did not breastfeed. The PR of 0.68 in Model 1 was a crude estimate of the association when no other covariates were adjusted, providing the baseline value for further comparison to the adjusted estimates of PRs in the subsequent adjusted Models 2–6. In Model 2 where the caregiver's socioeconomic factors—comprising the caregiver's education and sufficiency of family income per month—were considered potential confounding factors, the adjusted PRs and confidence intervals indicating the effect of breastfeeding were similar to the crude estimates in Model 1. In Model 3, the child's characteristics—including sex and age—along with the caregiver's socioeconomic factors were simultaneously adjusted in the model while omitting adjustment for the child's oral hygiene practice factors—comprising tooth brushing frequency, brushing before bed, and fluoride toothpaste use—that were considered colliders. In Model 4, the child's oral hygiene practice factors were adjusted. The adjusted estimates in Models 3 and 4 remained relatively the same as the crude estimates. The PRs slightly increased but maintained statistical significance in Models 5 and 6 when the fluoride concentrations in household water sources and all covariates except for colliders were subsequently adjusted (Table 3).
Multivariable Analyses of Association Between Breastfeeding and Dental Fluorosis
Multivariable models were estimated by Poisson regression with robust standard errors.
For each child, available measures of groundwater fluoride concentrations in drinking water sources supplying the child's residence were time averaged over the period from birth to the study.
CI, confidence interval; PR, prevalence ratio.
Discussion
The protective effect of breastfeeding against dental fluorosis has previously been demonstrated in a nonfluoridated rural setting with 10% of children having home water fluoride ≥0.7 ppm and a fluorosis prevalence of 23.3%.19,22 This study further examined whether the preventive effect of breastfeeding continued to exist in a more extreme and vulnerable setting of fluoride-endemic rural areas, where 96.2% and 73.1% of all children had fluoride concentrations of ≥0.7 and ≥1.5 ppm in household water sources, nearly half of the caregivers had no schooling, and 95.5% of all families had insufficient income. The 59.9% proportion of cases among all children in this community-based study also implied a considerably greater prevalence or burden of dental fluorosis in this study population. The current results consistently indicated the significant preventive effect of breastfeeding on dental fluorosis across all six statistical models (Table 3). The magnitude of PRs ranged from the lower preventive effect of 0.78 (95% confidence interval [CI]: 0.63–0.96) in Model 5 to the higher preventive effect of 0.66 (95% CI: 0.52–0.83) in Model 3. Alternatively, Models 5 and 3 revealed that children who weren't breastfed for at least 6 months had 1.28 (or 1/0.78) and 1.52 (or 1/0.66) times the prevalence of dental fluorosis compared to their counterparts. Statistical significance obtained in all models implied a greater probability that breastfeeding is associated with decreased occurrence of dental fluorosis. Nonetheless, the magnitude of the PRs, which reflected the strength of the association, indicated that the preventive effect of breastfeeding against dental fluorosis in this extremely vulnerable context was not so strong. This finding may be related to the fact that dental fluorosis is a multifactorial disease caused by the complex interaction of multiple contributing factors rather than a strong impact of a single factor.29,30
To rationally estimate the effect of breastfeeding on dental fluorosis, this study was conducted with three key methodological strategies, including (1) the use of a study design capable of assessing the temporal relationship, (2) the use of DAG to depict causal models being evaluated, and (3) the use of a statistical approach to avoid overestimation of effect measure. Previous cross-sectional studies have suggested the possible role of breastfeeding as a protective factor against dental fluorosis and paved the way to further improve the estimation of the effect using more rigorous analytical designs.20–22 This study thus applied the community-based case–control design to ensure that cases and controls reflected the burden of dental fluorosis in the studied villages and the temporal sequence of exposure factors that preceded dental fluorosis outcome. The use of DAG would also improve the validity of the effect estimate by understanding the various roles of factors in the etiology of dental fluorosis and enabling adjustment of appropriate confounders while avoiding the adjustment of mediators and colliders.23,31 Unlike conventional regression approach that typically selects explanatory variables based on statistically significant results of univariable analyses and adjusts all selected variables at once in the final multivariable analysis, DAG accounts for the role of each explanatory variable in various causal models that ultimately determine only pertinent confounders to be sequentially adjusted. In Figure 1, caregiver's socioeconomic factors were considered confounders in Model 2 as caregiver's education and family income could influence both breastfeeding practice 32 and risk of dental fluorosis. 33 In Model 3, child's oral hygiene practice variables were considered as colliders because the oral hygiene practice could be the consequence of both caregiver's socioeconomic factors and child's characteristics. 34 Although these colliders would block this path from breastfeeding to dental fluorosis, Model 3 was still executed to demonstrate another possible causal model. In Model 4, since child's oral health practice could be the consequence of caregiver's socioeconomic status, 34 these practice factors could also be considered as confounders and separately adjusted. In Model 5, fluoride concentration factor was assessed to determine whether it could confound the association. The percentage change in effect estimate of −12.8% was obtained from the formula of ([PRcrude−PRadjusted]/PRadjusted) × 100% or having ([0.68–0.78]/0.78) × 100%. As the 12.8% was greater than the 10% cutoff, fluoride concentration factor was thus considered a confounder. 35 In Model 6, all covariates were adjusted except for the colliders. The protective effect of breastfeeding was confirmed across all causal models. Ultimately, regression approach estimating PR was applied instead of the ones estimating odds ratio to avoid overestimation problem when disease outcome was common and to secure valid effect estimate. 36
Since past exposure factors of each child were traced retrospectively since birth, a possible threat to the validity of this study was the limitation to recall that affected recall accuracy. Nonetheless, recall of past exposure would be facilitated as these factors were habitual practice (e.g., breastfeeding and child's brushing frequency) or permanent characteristics (e.g., caregiver's education). Although exclusive breastfeeding (sole breastfeeding for 6 months with no formula) was generally advised during antenatal and postnatal care in these communities, the recommendation might have been followed to varying extents. The measurement of breastfeeding practice could therefore be further improved by a more in-depth categorization to identify exclusive and partial forms of breastfeeding, an area that could be addressed in future research.
Conclusions
Breastfeeding for at least 6 months had a preventive effect against dental fluorosis in permanent central incisors among children living in fluoride-endemic areas. Reinforcement of breastfeeding counseling during antenatal and postnatal care would improve maternal literacy and skills for breastfeeding to maintain a high rate and prolonged practice that potentially decreases the risk of dental fluorosis in the long term.
Footnotes
Acknowledgments
The authors acknowledge all the study participants and local public health officers for their valuable contributions to this study.
Authors' Contributions
Conceptualization by C.R., A.S., and P.N. Study design by C.R., S.O., A.S., and N.P. Data collection and validation by A.S. and P.N. Statistical analysis by C.R. and N.P. Writing and revising article by C.R. and S.O. All authors have read and agreed to the final version of the article.
Data Sharing Statement
The dataset used for this study is not publicly available due to the local public health office's restrictions.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.