
Abstract
Objectives:
Breastfeeding and human milk (HM) improve maternal and infant morbidities and mortality. Therefore, monitoring the safety of breastfeeding and access to HM is of critical importance. In this study, we assessed tools to monitor the presence of monkeypox virus (MPXV) in HM and whether standard Holder pasteurization inactivates MPXV.
Materials and Methods:
Heat-inactivated MPXV was added to HM or viral transport media (VTM) and analyzed using both research and clinical MPXV quantitative polymerase chain reaction (qPCR) tests. Infectious MPXV was added to HM and was exposed to 1 cycle of freeze–thaw, incubation for 1 hour at room temperature, or conditions of Holder pasteurization (62.5°C for 30 minutes) followed by infectious unit quantification by plaque assay.
Results:
Research and clinical nucleic acid tests detect MPXV that was added to HM but with reduced sensitivity compared with equivalent samples in VTM at low virus inoculum. MPXV added to HM to achieve a starting concentration of 225,000 plaque forming units (pfu)/mL remains infectious after freeze–thaw or 1 hour storage at room temperature. However, Holder pasteurization reduced infectious virus below the limit of detection, >2,000-fold reduction in viral titer.
Conclusion:
MPXV can be detected when added to HM using a clinical laboratory-developed qPCR test without modification, but the detection limit is reduced compared with equivalent samples in VTM. MPXV remains viable in HM should the virus ever gain access to HM, but Holder pasteurization reduces infectious MPXV to below detection limits and can be used to reduce the risk of MPXV transmission to infants who receive pasteurized (donor) HM.
Introduction
Breastfeeding and human milk (HM) improve maternal and infant survival and have many other short- and long-term health benefits for both mothers and infants.1,2 Therefore, monitoring the safety of breastfeeding and safe access to mother's own milk (MOM) or pasteurized donor HM (PDHM) is of critical importance, especially during health crises such as the recent SARS-CoV-2 and monkey pox virus (MPXV) outbreaks.
Pandemic preparedness requires a rapid deployment of robust and reliable tools to screen whether infectious agents can be detected in HM and pose a risk for maternal–infant transmission through breastfeeding or exposure to HM. As the most vulnerable preterm infants often depend on access to MOM or PDHM, pandemic preparedness also needs to determine whether Holder pasteurization and other technologies commonly used to treat HM in milk bank settings inactivate an infectious agent should it ever get access to HM.
Most recently, we assessed that people with SARS-CoV-2 infection, the virus causing the COVID-19 pandemic, did not transmit replication competent virus through HM. We also found that Holder pasteurization inactivates the virus should HM ever get contaminated with SARS-CoV-2. 3
Shortly after, MPXV emerged as a new potential infectious disease threat of global scale. Mpox is a viral infection that causes a rash, similar to smallpox, with or without systemic symptoms. Limited data suggest that mpox may be severe in neonates.4–6 There is significant concern about MPXV transmission to infants by postnatal exposures, including breastfeeding and HM. It is unknown whether MPXV is shed in HM, but MPXV and the antigenically similar Vaccinia virus (live component of the ACAM2000 smallpox vaccine) have been transmitted to breastfed infants.7,8
Transmission could occur through virus shedding into HM, contamination of expressed HM from lesions with high viral loads, or through skin-to-skin contact. Currently, the U.S. Centers for Disease Control (CDC) recommend that HM be discarded, and breastfeeding delayed in symptomatic or isolated individuals with mpox. 9
To better understand the potential risk of MPXV transmission in HM and how to mitigate that risk, we evaluated whether MPXV can be detected in HM by quantitative polymerase chain reaction (qPCR), whether virus remains infectious in HM under different storage conditions, and whether pasteurization inactivates MPXV in HM.
Materials and Methods
Human milk
Frozen donor HM was provided by the UC Health Milk Bank, San Diego. Fresh HM was provided by healthy volunteers whose supply exceeded the need of their breastfed infants. Milk from a full expression was aliquoted according to the experimental protocols outlined below and used within <2 hours of expression. HM collection was approved by the UC San Diego Institutional Review Board.
Cells and viruses
VeroE6 cells were maintained at 37°C and 5% CO2 in Dulbecco's modified eagle medium with 10% fetal bovine serum (FBS) and 1 × penicillin/streptomycin. MPXV clade II was isolated from a PCR-positive patient swab collected under IRB 160524XL by applying serial dilutions of swab material to VeroE6 cells. Cells and supernatant were collected after appearance of cytopathic effect. To generate passage 2 virus used for experiments, VeroE6 cells were infected at a multiplicity of infection of 0.2. Infected cells were pelleted and subject to three cycles of freeze–thaw with vortexing. Supernatant was saved separately. Material was clarified by centrifugation and aliquots were stored at −80 and titered by plaque assay. Isolation and clade identity were confirmed by PCR as described below.
Mpox clade II verification
Clade II identity was confirmed by Sanger sequencing of two regions of the viral genome previously used to differentiate clades I and II based on reports detailing Mpox genetic surveillance.10–13 Viral DNA was extracted from viral stock using the Zymo DNA miniprep kit following manufacturer's instructions for genomic DNA from liquid samples. Region 1 (46,239–46,737) and region 2 (133,388–133,984) were amplified using Q5 Hot Start High-Fidelity 2x Master Mix (New England Biolabs) with the following primers 1-F 5′-ACAGGGTTAACACCTTTCCAATA-3′ + 1-R 5′-AATCTCCAGAACCAGCATCAC-3′ and 2-F 5′ TACAGTTGAACGACTGCG 3′[13] + 2-R 5′-CTCTCTTGCTTCTTCGTCATAG-3′.
Positions refer to Mpox clade II RefSeq sequence NC_063383. Fragments were visualized as clean single bands on an agarose gel, and fragments were Sanger-sequenced using primers 1-R, 2-F, and 2-R resulting in 100% homology with clade II.
Viral heat inactivation
For inactivated virus spike-in experiments, titered viral supernatant was heat inactivated at 65°C for 35 minutes in a thermocycler. Work with infectious MPXV was conducted under BSL3 containment at UC San Diego following guidelines approved by the institutional biosafety committee.
Plaque assays
VeroE6 cells were plated in 12-well plates the day before infection. Serial dilutions of samples were added to monolayers (200 μL/well) and incubated with occasional rocking for 1 hour. Inputs were removed, and cells were overlaid with 0.8% methylcellulose in Minimum Essential Medium with 2% FBS and 1 × penicillin/streptomycin. After 3 days incubation, cells were fixed in 4% formaldehyde overnight and stained with crystal violet to visualize plaques.
Infectious virus spike-in experiments
For room temp incubation experiments, MPXV was added to 300 μL aliquots of fresh or frozen milk in triplicate. Samples were stored at −80°C immediately or after 1 hour at room temperature (RT). For Holder pasteurization experiments, MPXV was added to 20 mL fresh or frozen HM to an initial concentration of 100,000 plaque forming units (pfu)/mL. Milk was heated in 50 mL conical tubes in a heat block. An equal volume of HM without virus was monitored side by side with a thermometer. HM was heated for 30 minutes after temperature reached 62.5°C, after which HM was mixed well and triplicate 300 μL aliquots were stored at −80°C. Samples were saved before addition of viruses to monitor cytotoxicity of HM in the plaque assay and limit of detections (LoDs) are indicated in the figures.
DNA extraction and qPCR
Triplicate samples of viral transport media (VTM) or thawed HM from a single donor was spiked with serial dilutions of heat-inactivated MPXV. DNA was extracted using the Zymo DNA miniprep kit following manufacturer's instructions for genomic DNA from liquid samples or by Roche Cobas 5800 automated nucleic acid extraction protocol as described. 14 Laboratory-based qPCR was performed on a QuantStudio5 qPCR machine using mpox-specific primer/probe assay published by the CDC. 15
Primer and probe sequences: Forward: 5′-GGA AAA TGT AAA GAC AAC GAA TAC AG-3′. Reverse: 5′-GCT ATC ACA TAA TCT GGA AGC GTA-3′. Probe (FAM/ZEN/IBFQ): 5′-AAG CCG TAA TCT AGT TGT CTA TCG TGT CC-3′ Roche Cobas NVAR and mpox laboratory-developed tests were performed at UC San Diego CALM clinical laboratory.
Results
MPXV in HM is detectable by PCR assays
We first evaluated the ability to detect MPXV contamination in HM by qPCR tests. MPXV clade II was isolated and propagated in tissue culture from a positive clinical specimen collected in San Diego, CA, during the 2022 outbreak. For DNA detection experiments, viral stock was inactivated to facilitate handling in biosafety level 2 conditions. Inactivated MPXV dilutions were added to frozen donated HM or to VTM in triplicate to achieve concentrations equal to 0.1–100 pfu/mL. Samples were stored at −80°C and assayed using qPCR primers and probe published by the CDC with a commercial qPCR mastermix and a clinical laboratory-developed Roche Cobas 5800 Orthopox/MPXV test conducted in a CLIA laboratory.
MPXV DNA Ct values for DNA extracted from HM were modestly higher than VTM samples at the highest concentration measured by a research qPCR assay (Fig. 1A). After dilution, sensitivity of the assay for HM declined relative to that of VTM. MPXV in VTM was detectable in three of three replicates down to 1 pfu/mL. In contrast, MPXV in HM was detectable in two of three replicates at 10 pfu/mL and zero of three replicates at 1 pfu/mL.

Reduced detection of MPXV DNA spiked into HM compared with VTM. Frozen donated HM or VTM was spiked with 10-fold serial dilutions of heat-inactivated MPXV in triplicate at the indicated preinactivation pfu/mL.
Samples evaluated using the clinical laboratory qPCR test on the Roche Cobas 5800 was more sensitive, detecting three of three MPXV replicates in VTM at 0.1 pfu/mL. MPXV spiked samples in HM were positive in only one of three replicates at 1 pfu/mL and zero of three replicates at 0.1 pfu/mL (Fig. 1B).
MPXV remains infectious in HM after freeze–thaw or incubation at room temperature
Donated fresh or frozen HM (n = 2 donors each) was spiked with infectious MPXV in triplicate to a starting concentration of 225,000 pfu/mL in a volume of 300 μL. Samples were stored immediately at −80°C or incubated 1 hour at RT before storage at −80°C. Infectious virus was measured by plaque assay and compared with input virus. Uninfected samples were included in the plaque assay to control for cytotoxicity and established the LoD of MPXV as 125 pfu/mL.
After freezing, MPXV remained infectious in HM samples. One freeze–thaw cycle resulted in an average reduction of 68% of the virus added (Fig. 2A). Both fresh and frozen donated milk samples spiked with virus retained infectious viral loads >50,000 pfu/mL (Fig. 2B). Samples frozen immediately retained 20–40% of the infectious virus, and extending RT incubation to 1 hour before freezing yielded a modest additional reduction in titers to 25–30% of the original input (Fig. 2C).
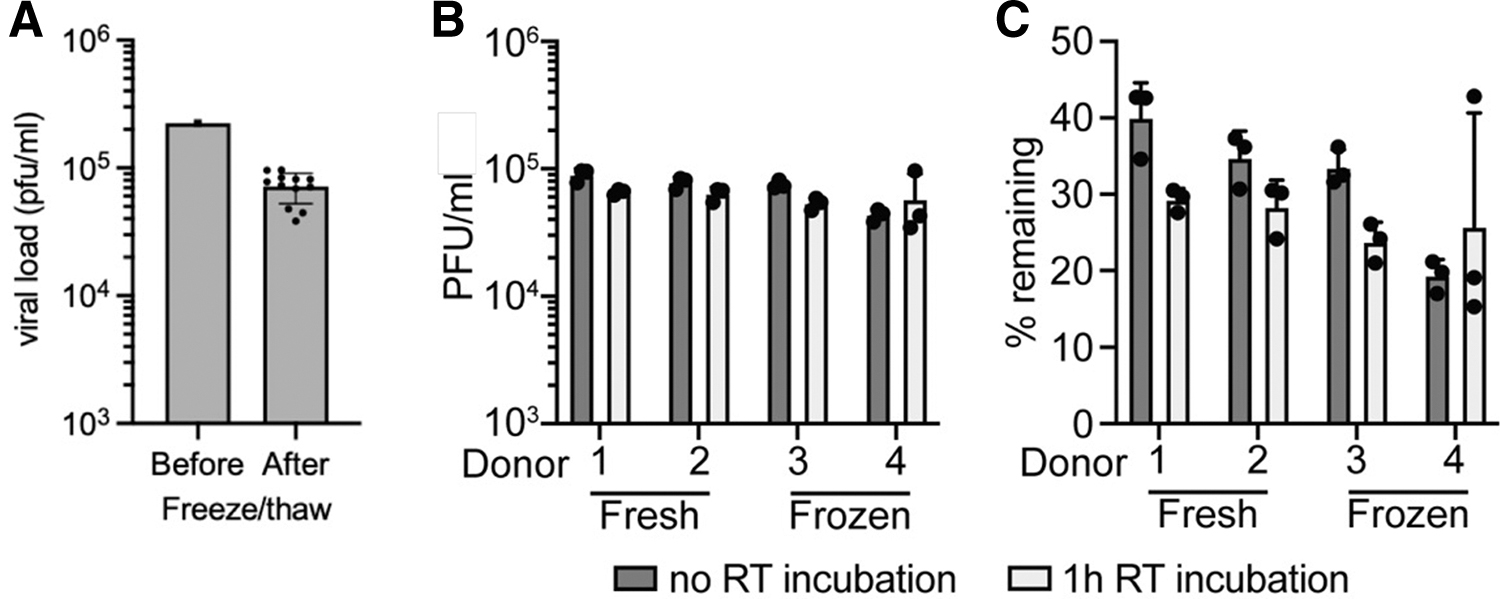
MPXV remains infectious in HM. Cultured MPXV was spiked into fresh or thawed HM and either stored immediately at −80°C or maintained at RT 1 hour before freezing.
Holder pasteurization inactivates MPXV in HM
To evaluate the effectiveness of MPXV inactivation by Holder pasteurization, infectious MPXV was spiked into 20 mL of fresh or frozen donated HM (n = 2 donors each) to a concentration of 100,000 pfu/mL. Milk was heated in 50 mL conical tubes in a heat block, and the temperature of a noninfected milk sample control was measured side by side. Titers of samples taken before heating retained approximately one-third of the input virus after freeze–thaw as shown in Figure 3. No infectious virus was detectable after Holder pasteurization. Controls for cytotoxicity established LoDs of 50 (fresh) and 250 (frozen) pfu/mL.

Holder pasteurization inactivates MPXV in HM. MPXV was spiked into 20 mL HM from four donors. Samples were removed for storage at −80°C before and after heating at 62.5°C for 30 minutes.
Discussion
Emergence of MPXV has created yet another uncertainty about the safety of breastfeeding and safe access to PDHM. Our results demonstrate that MPXV is relatively stable in HM including after freeze–thaw, which suggests that infectious MPXV could be transmitted if it is secreted into or contaminates HM, for example, from skin lesions.
Clinical nucleic acid tests are the preferred diagnostic test for mpox. Clinical samples for mpox are typically submitted as dry swabs or swabs in VTM taken from skin lesions. We found that both research and clinical qPCR tests can detect MPXV in HM, but they do so with lower sensitivity compared with equivalent samples in VTM. Additional studies will be needed to determine whether the reduced sensitivity in HM compared with VTM is caused by interference in DNA extraction, presence of qPCR inhibitors, or degradation of free viral DNA. Our data suggest that qPCR assays do not reliably detect the presence of very low levels of infectious MPXV in HM. As the infectious dose of MPXV by ingestion is not known, negative qPCR results from HM samples should be treated with caution.
Currently, the CDC recommends pasteurization of HM to prevent transmission of MPXV. 9 Although MPXV is heat sensitive in other media, 16 there is no data to our knowledge demonstrating that MPXV in HM is inactivated by Holder pasteurization. We demonstrate that conditions mimicking Holder pasteurization of HM, commonly used in HM banks, reduce infectious titers to below the LoD of our assay (>2,000-fold in fresh and >400-fold in frozen). These results support the CDC recommendation to pasteurize HM and are reassuring given the benefits of breastfeeding and HM provided through PDHM.
Limitations of our study include the small sample size of HM from different donors and the inherent cytotoxicity of HM that increases the LoD when quantifying pfu in cell culture models.
Conclusion
In conclusion, our results suggest that MPXV contamination of HM is a transmission risk. Low MPXV levels in HM may escape detection by nucleic acid tests, but Holder pasteurization is effective at inactivating the virus. Fortunately, MPXV did not rise to pandemic levels. Nonetheless, national and global pandemic preparedness plans need to include protocols to rapidly develop, validate, and deploy robust tools that can monitor the safety of breastfeeding and safe access to PDHM. Breastfeeding and HM have robust maternal and child health implications and need to be protected, especially at the onset of health crises.
Footnotes
Authors' Contributions
A.E.C. conceptualized and designed the study, conducted experiments, and analyzed data. A.F., K.S., and M.P. conducted experiments and analyzed data. L.S., D.P., and D.S. conceptualized and designed the study. A.F.C. and L.B. conceptualized and designed the study, and wrote the initial article. All authors approved the final article as submitted and agree to be accountable for all aspects of the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by UCSD PREPARE and Human Milk Institutes, NIH grants AI036214 and AI131385 to D.S.; San Diego Center for AIDS Research (CFAR) AI100665, the Department of Veterans Affairs, the John and Mary Tu Foundation, and the James B. Pendleton Charitable Trust. A.F.C. was supported by an NIH grant K08 AI130381 and a Career Award for Medical Scientists from the Burroughs Wellcome Fund. L.B. is UC San Diego Chair of Collaborative Human Milk Research endowed by the Family Larsson-Rosenquist Foundation (FLRF), Switzerland.