
Abstract
Background and Objective:
The prevalence of ankyloglossia and its impact on breastfeeding practices may be overestimated, leading to surgical overtreatment in newborns. The study was conducted to estimate the prevalence of ankyloglossia in the first year of life and investigate the association with exclusive and total breastfeeding duration in different regions of Brazil.
Materials and Methods:
This multicenter prospective cohort study involved the recruitment of mother–infant pairs soon after childbirth in public hospitals in three state capitals in Brazil. Interviews were held with the mothers after birth, at 6 and 12 months to collect sociodemographic variables and data on exclusive and total breastfeeding duration. At 12 months of age, the children were submitted to a dental examination for classification of the lingual frenulum using the Bristol Tongue Assessment Tool. Data analysis involved Poisson regression with robust variance, with the calculation of unadjusted and adjusted relative risk (RR).
Results:
The final sample was composed of 293 children. The prevalence of defined and suspected ankyloglossia was 1% and 4.8%, respectively, totaling 5.8% (confidence interval [95% CI]: 3.1–8.5). No significant difference was found in the prevalence of exclusive and total breastfeeding at 1, 4, and 6 months between children with defined/suspected ankyloglossia and those without ankyloglossia. The multivariable analysis showed that the probability of the child achieving 6 months of breastfeeding did not differ between groups (RR = 0.98; 95% CI: 0.79–1.23; p = 0.907).
Conclusion:
The prevalence of defined ankyloglossia was very low and defined/suspected ankyloglossia was not associated with exclusive or total breastfeeding duration.
Clinical Trial Registration:
Registered with clinicaltrials.gov (n° NCT03841123).
Introduction
Breastfeeding protects from malnutrition, infectious diseases, and child mortality and also reduces the risk of obesity and chronic diseases in the long term.1–3 Although 80% of newborns receive breast milk in practically all countries of the world, only 37% of infants <6 months of age are exclusively breastfed in middle- and low-income countries.4,5 The factors associated with early weaning include maternal depression, self-reported insufficient milk, pain during breastfeeding, early introduction of milk formula, and pacifier use.3,6–9 Recently, there has been an important discussion on the role of ankyloglossia (tongue-tie) in early weaning. 10
Ankyloglossia can potentially impede or hamper the transference of milk and increase maternal discomfort, exerting a negative impact on the establishment and maintenance of adequate breastfeeding practices.11,12 However, the impact of this condition on breastfeeding duration in newborns is generally reported in case reports, whereas prospective cohort studies with adequate methodological quality are scarce. The clarification of this issue is essential to defining the need for early surgical intervention in cases of ankyloglossia. Although systematic reviews have reported that frenotomy in newborns reduces maternal nipple pain in the short term, divergent opinions are found regarding the positive effect on the duration of breastfeeding,13–15 putting into question the benefits of the intervention.16,17
Another point to clarify is the prevalence of ankyloglossia. Although a recent systematic review reported the prevalence of ankyloglossia in newborns to be 5%, 18 there is considerable variation among the studies (1.5–38%),19–21 which demonstrates differences in diagnostic criteria. 11 An overestimation of the prevalence can lead to unnecessary surgeries in newborns, which has been reported in different countries,22–24 with possible adverse effects, such as bleeding requiring medical attention, hypovolemic shock, apnea, acute airway obstruction, and a delayed diagnosis of an alternative underlying condition.10,25,26 Different ankyloglossia examination protocols are available to clinicians and researchers, among which the Bristol Tongue Assessment Tool (BTAT) 27 is a simple, concise protocol and the most reliable with regard to its capacity to predict breastfeeding problems and identify infants that may benefit from frenotomy.11,28–30 Brazil has a mandatory frenulum inspection law using the BTAT protocol similar to the newborn screening laws for genetic diseases. 31
Therefore, the aim of the present study was to estimate the prevalence of ankyloglossia in the first year of life and investigate the association with exclusive and total breastfeeding duration in a birth cohort followed up in three large cities in different regions of Brazil.
Methods
Study design and participants
This is birth cohort study nested in a randomized field trial with 6- and 12-month follow-up conducted with mother–child pairs in three state capitals in Brazil: Porto Alegre (South region), Manaus (North region), and Salvador (Northeast region). The original study consisted of a single intervention for mothers in maternity hospitals shortly after the birth of their children. The intervention comprised (1) reinforcing the importance of breastfeeding and guiding the introduction of healthy foods from the sixth month of age, and (2) avoiding consumption of sugar and ultraprocessed foods for up to 2 years of age.
Enrollment took place at hospitals that take part in the Baby-Friendly Hospital Initiative (BFHI), which is internationally recognized for supporting breastfeeding. Among other rules and procedures, BFHI-participating hospitals inform all pregnant women about the benefits and management of breastfeeding, help mothers initiate breastfeeding after delivery, show mothers how to breastfeed and how to maintain lactation, do not offer artificial nipples or pacifiers to breastfed children, promote support groups for breastfeeding, and refer mothers to these groups at the time of discharge from the maternity ward. This is a worldwide initiative with recognized positive impacts on breastfeeding on short-, medium-, and long-term outcomes. 32 The eligibility criteria for the study included mothers 18 years of age or older, testing negative for HIV and HTLV1, with a singleton pregnancy, delivering at ≥37 weeks, birth weight >2500 g and the absence of congenital anomalies or neonatal conditions that could affect the newborn's ability to breastfeed. For the present study, frenotomy was an exclusion criterion.
The sample size for the intervention study was calculated using the G*Power software package version 3.1.9.4 (University of Düsseldorf, Düsseldorf, Germany, 2019) and was based on the estimate of the reduction in the prevalence of children who consumed sugar in the first year of life, determining a minimum sample of 114 children per region of collection. A factor of 1.2 was added for the cluster effect and an additional 20% was added to compensate for possible dropouts, leading to 168 children for each region, with an overall sample of 504 children. The sample of the present study was composed of the mother–child pairs included at birth and who completed the 12-month assessment. Considering an estimated 5% frequency of ankyloglossia, the sample size in the present study (n = 293) had an 83% power and 95% confidence level to detect an increase in the cessation of exclusive breastfeeding in the first month of life from 40% to 80% in children with ankyloglossia. 33 Figure 1 displays the diagram of the cohort from the recruitment of the pregnant women to 12 months of age.
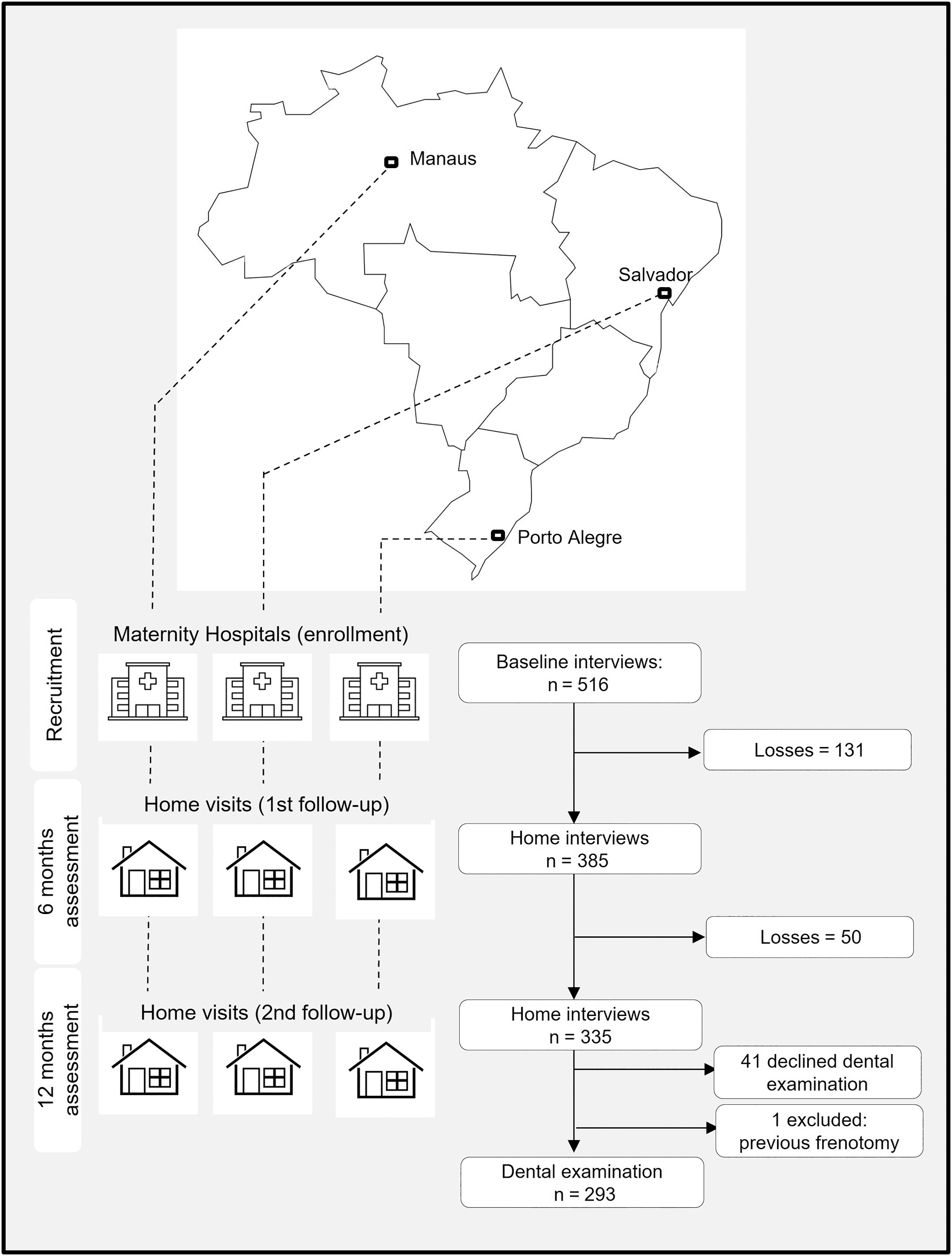
Flowchart of cohort.
Data collection
The baseline characteristics of the cohort were obtained in the maternity hospitals through interviews held with the mothers for the collection of their sociodemographic data: age (in complete years and categorized in terciles), education (in complete years of study and categorized as <8, 8 to 11, and >11 years), family structure (nuclear, when mother and father live together and nonnuclear), and onset of prenatal care (first trimester and after the first trimester). Data from the infants' health records after delivery furnished the following variables: sex, birth weight (in grams and categorized as <10th percentile and ≥10th percentile), and length at birth (in centimeters and categorized as <48 and ≥48 cm). At 6 and 12 months, face-to-face interviews were held with the mothers in their homes for the collection of data on feeding practices, pacifier use, and general health of the children. The interviews investigated exclusive and total breastfeeding and pacifier use (yes or no) for each month separately. Exclusive and total breastfeeding duration was then categorized as </≥1, </≥4, and </≥6 months.
Among information regarding child's general health, mothers were asked about health events and procedures during the first year of life, including the performance of frenotomy.
At 12 months, dental clinical examinations were conducted by trained dentists with the aid of artificial light and a mouth mirror with the child lying on a mat on a stable, safe surface. The lingual frenulum was examined using the BTAT, which involves the assessment of four items: (1) appearance of the tip of the tongue; (2) attachment of the frenulum to the lower gingival margin; (3) elevation of the tongue; and (4) projection of the tongue. After scoring each item as 0, 1, or 2, the scores are summed and range from 0 to 8. 0 to 3 indicates a potential reduction in tongue function (defined ankyloglossia); 4 and 5 indicate suspected ankyloglossia; 6, 7 and 8 indicate the absence of ankyloglossia. The mothers were also asked about the age (in months) of the eruption of the first tooth.
Training of interviewers and examiners
Before each phase of the study, interviewers at the three centers underwent training supervised by the team coordinator to improve the reliability of the data collection process, including specific guidelines on each item of the questionnaire. Regular meetings were also held during the data collection period to obtain feedback on the interviews and clear up any questions, strengthening the key points of the training process.
Training of the dentists at the three centers was conducted by an experienced pediatric dentist. Theoretical training was performed with the aid of clinical photographs and a dental clinical examination manual developed specifically for the study, including dental caries, traumatic dental injuries, and the lingual frenulum. Practical training was then conducted involving the calibration of the examiners at the three centers conducted by the same pediatric dentist, which included the examination of children between 1 and 2 years of age for these three clinical conditions.
Statistical analysis
Statistical analysis was conducted with the aid of the SPSS software, version 20.0. Bristol ≤5 was classified as defined or suspected ankyloglossia. The chi-square and Mann–Whitney tests were used to compare the duration of exclusive and total breastfeeding (proportions at the different cutoff points and as a quantitative variable, respectively) between children with and without ankyloglossia. Poisson regression with robust variance was performed to investigate the association between ankyloglossia and the primary outcome (exclusive breastfeeding <1 month) and secondary outcome (total breastfeeding <6 months), with the calculation of unadjusted and adjusted relative risk (RR) and confidence intervals (95% CI). All variables of the unadjusted model were incorporated into the multivariable model. The significance level was set at 5% (p < 0.05).
Ethical aspects
This study received approval from the Human Research Ethics Committee of the Federal University of Health Sciences in the city of Porto Alegre (n° 88214918.3.0000.5345) and was registered with clinicaltrials.gov (n° NCT03841123). All mothers provided written informed consent on behalf of their newborns. All procedures were performed in accordance with Resolution 466/12 of the Brazilian National Health Council and the Declaration of Helsinki.
Results
Of the 335 children in the cohort evaluated at 12 months, 41 caregivers refused a dental examination and 1 child was excluded from the analysis due to a previous frenotomy. The final sample was composed of 293 children with nearly equal distribution in terms of sex (52.0% male). The majority of families had a nuclear structure (75.0%) and mother's education ranged from 1 to 17 years, with a mean and standard deviation of 10.0 ± 2.6 years. The sociodemographic characteristics of the mothers and anthropometric characteristics of the children at baseline of the cohort and in the sample analyzed herein were similar (Table 1).
Characteristics of Participants at the Baseline of the Cohort and at 12 Months of Age
SD, standard deviation.
The prevalence of exclusive breastfeeding for 1, 4, and 6 months was 74.0%, 35.4%, and 12.6%, respectively. At 12 months of age, 72.0% of children were still breastfeeding. Although exclusive breastfeeding rates at 1 month did not differ among regions, the prevalence of children still breastfeeding at 6 months of age was higher in the North and Northeast regions compared with the South region (p = 0.001).
BTAT scores ranged from 0 to 8, with 1% of the children (3/293) having defined ankyloglossia and 4.8% exhibiting suspected ankyloglossia (14/293) Thus, the prevalence of defined or suspected ankyloglossia was 5.8% (95% CI: 3.1–8.5). Among the three children with defined ankyloglossia, one began exclusive breastfeeding but did not complete the first month, whereas the others completed 2 and 3 months of exclusive breastfeeding. The duration of total breastfeeding was 1 month for one of these children, whereas the other two were still breastfeeding at 12 months (Fig. 2).
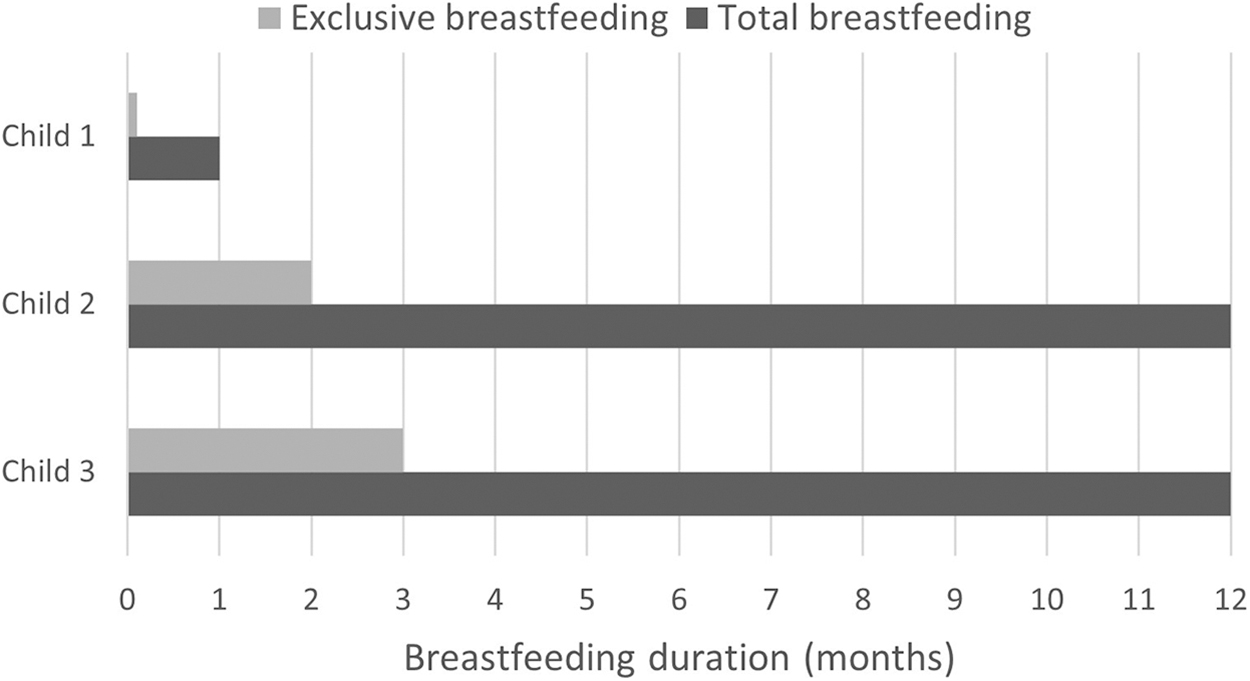
Exclusive and total breastfeeding duration in participants with ankyloglossia.
No difference was found between children with and without ankyloglossia with regard to the average duration of exclusive breastfeeding or the proportion of children who reached 1 and 4 months of exclusive and total breastfeeding. The prevalence of children with and without ankyloglossia who reached 6 months of total breastfeeding was virtually the same (Table 2).
Exclusive and Total Breastfeeding Duration According to the Presence of Defined/Suspected Ankyloglossia
SD, standard deviation.
The multivariable analysis revealed that the risk of cessation of exclusive breastfeeding before completing the first month was 61% greater in children who used a pacifier in the first month of life. However, no difference was found between children with and without ankyloglossia even after adjusting for confounding factors (p = 0.376, Table 3). The risk of not completing 6 months of total breastfeeding was 88% greater when the mother was <24 years of age, two and a half times greater in children with a lower birthweight (p = 0.005), and six and a half times greater in children who used a pacifier in the first month of life (p < 0.001; Table 4). However, children with ankyloglossia had a similar risk of cessation of total breastfeeding before 6 months of age as children without ankyloglossia (p = 0.944).
Unadjusted and Adjusted Relative Risk of Interrupting Exclusive Breastfeeding Before Completing the First Month of Life According to Mothers' and Children's Characteristics
CI, confidence interval; RR, relative risk.
Unadjusted and Adjusted Relative Risk of Interrupting Total Breastfeeding Before Completing 6 Months of Life According to Mothers' and Children's Characteristics
CI, confidence interval; RR, relative risk.
The most reported reasons by mothers who ceased breastfeeding were “the child doesn't want it anymore,” the mother's need to be away to work, “not enough milk,” and pain when breastfeeding. Even with follow-up in the primary care center, no mother reported problems related to tongue-tie.
An additional analysis was performed to investigate the potential effects of losses to follow-up on the results of the present study. No difference was found between the children who were lost to follow-up and those who remained at 12 months of age regarding exclusive breastfeeding at 1 month (lost: 74.1%; analyzed: 74.0%; p = 0.981), breastfeeding at 6 months (lost: 88.8%; analyzed: 82.6%; p = 0.123), or risk factors for breastfeeding cessation: maternal education ≤8 years (lost: 24.6%; analyzed: 23.9%, p = 0.856) and pacifier use at 6 months (lost 61.7%; analyzed: 59.2%; p = 0.656).
Discussion
The present birth cohort study investigated the prevalence of ankyloglossia and its association with exclusive and total breastfeeding duration in the first year of life. The findings showed that the prevalence of ankyloglossia was low and no associations were found with the different cutoff points of exclusive and total breastfeeding.
The very low prevalence of defined ankyloglossia limited the investigation of its association with breastfeeding duration. Interestingly, defined ankyloglossia was not an impediment for two of the three children with this condition to continue breastfeeding at 12 months of age and have exclusive breastfeeding for 2 and 3 months. At the same time, it is possible that defined ankyloglossia determined the early cessation of both outcomes in the other child. However, such results are merely descriptive and resemble findings from clinical case reports without providing evidence of the absence of harm from the exposure to breastfeeding duration.
On the other hand, analyzing the group of children with defined and suspected ankyloglossia together compared with those without ankyloglossia, no difference was found in the risk of cessation of exclusive breastfeeding in the first month or breastfeeding in the first 6 months of life. Although these findings do not eliminate the possibility of some influence of the exposure on the outcomes, with an emphasis on the possibility of breastfeeding difficulties, this effect was not sufficient to stop breastfeeding in the children investigated. Interestingly, the proportion of children that reached 6 months of breastfeeding, which is an important indicator of the World Health Organization, 2 was virtually the same among the children with and without ankyloglossia.
To the best of our knowledge, this is the first study to estimate exclusive and total breastfeeding duration in the first year of life according to the presence of ankyloglossia. Previous studies investigated breastfeeding difficulties soon after delivery or in the first months of life in children with ankyloglossia. A systematic review that investigated children with ankyloglossia reported that the average latch score was below the ideal limit, with high nipple pain scores; moreover, the Breastfeeding Self-Efficacy Scale-Short indicated risk scores for the cessation of exclusive breastfeeding in the first 3 months of life. However, average breastfeeding duration was not assessed and there was no comparison to children without ankyloglossia. 34 It has been reported that less than half of children with ankyloglossia have breastfeeding difficulties,35,36 whereas children without ankyloglossia can also have such difficulties. 37
Among the clinical implications, the present results together with the findings of previous studies put into question the decision for surgical treatment exclusively based on the classification of the lingual frenulum. The decision for invasive treatment in an infant, assuming the risk of side effects, should be preceded by a careful assessment of all possible causes of breastfeeding difficulties. First, mothers should be warned that crying, unsettled behavior, and short night-time durations, which are often misconceived as signs of feeding problems, may be common infant adaptations to the postbirth environment. 3 Common causes of real breastfeeding difficulties, such as pain during breastfeeding, emotional problems on the part of the mother (anxiety or depression), and lack of experience or guidance for the adequate practice of breastfeeding are also factors that must be taken into account. 38 This involves an interdisciplinary assessment that health care providers should make together, with the decision for surgical intervention indicated after all causal factors have been discarded.
An adequate indication significantly increases the effectiveness of the procedure, with benefits for mothers and infants 36 and, at the same time, reduces the number of unnecessary surgeries with potential health and economic impacts, including unnecessary hospitalizations. 25 Another concern is that overdiagnosis and surgical overtreatment can mask and delay the diagnosis of other medical conditions that may be exerting an impact on the infant's capacity to breastfeed. 10
The assessment of the lingual frenulum using the BTAT Protocol is mandatory in Brazil and is part of the physical examination of newborns. 31 Even in children with Bristol scores less than or equal to 3, the surgical procedure is not immediately recommended, suggesting a new assessment of breastfeeding, including the need to rule out other factors that justify breastfeeding difficulties. Nonetheless, mandatory screening can inevitably lead to overtreatment. 39 The World Health Organization has proposed requirements with regard to screening for conditions or diseases and the occurrence of lingual frenulum only partially meets these assumptions. 40
Future prospective studies should investigate in a multidisciplinary way, and simultaneously all potential causes of breastfeeding difficulties, to identify the contribution of each factor. Such knowledge could provide safer cues of the proportion of infants who would benefit from each type of treatment.
The proportion of loss to follow-up stands out among the limitations of the present study. However, this proportion is similar to that of other birth cohort studies that follow-up children in their first year of life. 41 Moreover, the fact that there were no differences between the initial cohort and the one analyzed suggest the probability that the risk of selection bias is low. The final sample size was reasonable and capable of detecting other conditions previously associated with a shorter breastfeeding duration, such as a lower birthweight and pacifier use.8,42 In addition, the reported regional differences, with a higher frequency of breastfeeding at 6 months of age in the North and Northeast regions compared with the South region, reflect differences previously described in a national survey with Brazilian children <2 years of age. 33 Second, ankyloglossia was assessed at 12 months, which represents a limitation of the present study.
However, a previous study that prospectively investigated characteristics of the lingual frenulum from birth to 12 months concluded that changes concerning lingual frenulum thickness, attachment to the tongue and to the floor of the mouth were not observed in the infants during the first year of life. 43 Third, despite the diagnosis of ankyloglossia involves some degree of subjectivity on the part of the evaluator, the BTAT protocol is simple, concise, and the most reliable instrument in predicting breastfeeding problems. In addition, extensive prior training was carried out, reducing the possibility of information bias.
In conclusion, the prevalence of defined ankyloglossia was very low in the three Brazilian state capitals and no association was found between defined/suspected ankyloglossia and exclusive or total breastfeeding duration. Although these results do not eliminate the possibility of the interference of the lingual frenulum with breastfeeding practices in specific situations, the findings draw attention to the need to investigate all potential reasons for the cessation of breastfeeding before proceeding to frenotomy.
Footnotes
Authors' Contributions
A.B.d.S.H.: Conceptualization, Methodology, and Software. C.A.F.: Conceptualization, Methodology, Software, Data curation, Writing—Original draft preparation, and Investigation. P.H.R.: Investigation, and Methodology. E.M.R.d.B.C.: Methodology, and Software. M.R.V.: Conceptualization, Methodology, Software, and Validation. P.F.K.: Supervision, and Writing—Reviewing and Editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
The work was supported by the National Council for Scientific and Technological Development (CNPq) (No. 408125/2017-9).