
Abstract
Background:
Bronchopulmonary dysplasia (BPD) is a common complication of preterm very low birth weight (VLBW) infants. Mother’s own milk (MOM) may mitigate the severity of BPD. Pasteurized donor human milk (PDHM) is often used as an alternative when MOM is unavailable with limited information on the influence of PDHM on BPD risk and severity.
Objective:
To compare the influence of MOM to PDHM on risk and severity of BPD in preterm VLBW infants.
Design/Methods:
A retrospective chart review of preterm (<34 weeks) and VLBW (<1,500 g) infants born at the Children’s Hospital of Richmond from 2019 to 2021 was performed. The analysis included demographics, type and timing of nutrition received (MOM, PDHM, Formula), and incidence/severity of BPD based on National Institute of Child Health & Human Development (NICHD) definition. Data analysis used chi-square, linear regression, and a multinomial logistic regression test.
Results:
A total of 200 infants met inclusion criteria, of which 116 (58%) had no BPD, 34 (17%) had mild BPD, 32 (16%) had moderate BPD, and 18 (9%) had severe BPD. Infants exposed to MOM within the first 3 days and within the first 7 days of life had lower incidence of moderate to severe BPD when compared to those with no MOM exposure (p = 0.02, p = 0.04). The percent of MOM received throughout hospitalization moderated the incidence of BPD (p = 0.01, 95% Confidence Interval (CI) [−0.14, −0.02]), such that as the percent of MOM received increased, the effect of gestational age on severity of BPD decreased. In contrast, the percent of PDHM received throughout hospitalization did not moderate BPD incidence (p = 0.61, 95% CI [2.28, 3.43]).
Conclusion:
These results identify that earlier and greater total exposure to MOM, but not PDHM, was associated with decreased moderate to severe BPD in <34-week preterm VLBW infants.
Introduction
Chronic lung disease during infancy, or bronchopulmonary dysplasia (BPD), a result of injury to the underdeveloped lung, is a major global problem with adverse effects on long-term pulmonary health and neurodevelopment that persists into adulthood.1–3 BPD is a common complication of very low birth weight (VLBW, birth weight <1,500 g) infants.2,3 Many external factors are implicated including positive pressure mechanical ventilation, oxygen toxicity, and infection with little improvement of BPD despite advanced noninvasive ventilation strategies.2,4 More recently, inadequate enteral nutrition, despite compensated total nutritional content, has been shown to contribute to the incidence and severity of BPD. 5
Mother’s own milk (MOM) is the preferred nutrition for the VLBW infant at risk for morbidities related to prematurity.6–10 Pasteurized donor human milk (PDHM) pooled from multiple donors, generally of mothers who have delivered at term, retains some of the nutritional and immunological properties of MOM but with reduced levels of leukocytes, immunoglobulins and antimicrobial proteins including lysozyme, lactadherin, and lactoferrin. 11 This data on the composition of PDHM suggests that PDHM may not provide the same level of benefit in a variety of diseases for preterm infants as MOM. 12
Nutrition and postnatal growth deficit have been important to the resolution of BPD. 13
Importantly, recent studies identify the specific influence of human milk and the incidence/severity of BPD.14,15 MOM compared to preterm formula (PF) has been shown to protect against BPD in VLBW infants.15,16 Similarly, PDHM compared to PF has been shown to protect against BPD in VLBW infants. 17 However, the evidence comparing the impact of MOM to PDHM in moderating BPD is limited. Therefore, the purpose of this study was to address this knowledge gap by investigating the dose-dependent impact of early provision of MOM on the incidence of moderate/severe BPD in comparison to the dose-dependent impact of PDHM on the incidence of moderate/severe BPD.
Methods
A retrospective chart review was conducted of VLBW infants admitted to the Children’s Hospital of Richmond (CHoR) NICU between 2019 and 2021. Inclusion criteria for the study were birth weight <1,500 g and gestational age <34 weeks. Exclusion criteria for the study were death within 7 days of life and major congenital anomalies. The study was approved by the Virginia Commonwealth University Institutional Review Board.
Infant nutrition
CHoR NICU nutritional practice guidelines were unchanged during the timeframe of the study. All VLBW infants received total parental nutrition upon admission. Freshly expressed colostrum was administered as available. Enteral feedings were started as soon as the infant was clinically stable enough to feed, ideally within the first 24 hours of life. MOM was the preferred feeding. If MOM was not available, PDHM was preferred over formula for infants <34 weeks with written informed consent of the parents. Feedings of MOM or pasteurized donor milk were fortified with Prolact+H2MF® (Prolacta Bioscience, Industry, CA). 18 human milk-derived fortifier processed from 100% donor milk, when feeding volume reached 80 mL/kg/day.
Infants receiving PDHM were transitioned to PF at the completion of 34 weeks corrected age. Infants receiving MOM continued through discharge home with transition to unfortified mother’s milk and supplementation of two feedings of transitional 22-calorie formula at 36 weeks corrected age.
BPD classification
BPD was classified using the 2019 NICHD criteria, which categorizes severity of BPD by respiratory support at 36 weeks Post Menstrual Age (PMA), with infants requiring a fraction of inspired oxygen (FiO2) of <30% classified as moderate BPD and those requiring any positive pressure ventilation or FiO2 ≥ 30% as severe BPD. 1
Data extraction and analysis
A retrospective chart review included collection of demographic data, gestational age, birthweight, sex, race/ethnicity of the infant and mother, details of hospital course including maternal use of antenatal steroids, maternal chorioamnionitis, maternal hypertension, and fetal growth restriction. Infant hospital course data included type and duration of nutrition received weekly by volume, categorized as MOM, PDHM, and PF as well as use of fortification and volume. Medication exposure including exposure to surfactant, caffeine, postnatal steroids, diuretics, and iron/multivitamins was collected. Outcome data including incidence/severity of BPD, incidence of necrotizing enterocolitis ≥ stage II, incidence of any intraventricular hemorrhage and/or periventricular leukomalacia, incidence of any type of retinopathy of prematurity, incidence of sepsis/meningitis after 3 days, mortality, weight gain, linear growth, and head growth. For early exposure, all infants were included in analysis. For total Neonatal Intensive Care Unit (NICU) course, infants who died after 7 days of life and before 36 weeks corrected (N = 9) were excluded.
Data analysis
The data were expressed as means and standard deviations (SD) for continuous variables or as numbers/percentages for categorical variables. The Student’s t-test or the Mann–Whitney test were used to compare independent variables according to their size and characteristics between the two groups. Linear regression, a multinomial logistic regression, and tests of moderation were used to compare group differences. A Pearson chi-square test was used to compare categorical variables between groups. Moderation analysis was conducted examining percentage of MOM and PDHM (throughout total hospitalization) as a moderator on gestational age (weeks) to incidence of moderate/severe BPD. Significance was considered with a p < 0.05.
Results
Infant characteristics
There were 200 infants who met inclusion criteria, birth weight <1,500 g, and gestational age <34 weeks with 84 (42%) who met the criteria of BPD. The mean gestational age was 28.1 ± 2.9 SD, with a mean birth weight of 1024 ± 2.9 SD (Table 1). The characteristics of the infants within the four groups identified 116 (58%) with no BPD diagnosis. Of the 84 infants identified with BPD, 34 (41%) had mild BPD, 32 (38%) had moderate BPD, and 18 (21%) had severe BPD, as shown in Table 2. There were 17 infants who expired during their hospitalization with 183 infants included in the longitudinal volume analysis. The 50 infants with moderate and severe BPD were more likely to be of smaller gestational age and lower birth weight. Infants with moderate and severe BPD were more likely to be of male sex. There were no racial or ethnic differences in the risk of BPD severity among the population cohort (Table 2).
Infant Characteristics, N = 200
SD, standard deviation.
Characteristics of Infants Based on BPD Diagnosis and Severity, N = 200
Compared to No BPD cohort.
BPD, bronchopulmonary dysplasia; SD, standard deviation.
Infant feeding characteristics during hospitalization
Infant feeding characteristics identified that 99/200 (49.5%) of infants were fed exclusive MOM during the first 3 days of life with 131 (65.5%) fed MOM during the first 7 days. Evaluation of the cumulative nutritional intake by MOM indicated that formula exposure was identified at a low percent during hospitalization for the cohort with 87% of the cohort receiving 0–25% of formula intake. In comparison, the percentage of infants receiving cumulatively greater percentage of MOM at 76–100% was MOM greater than PDHM greater than formula (Table 3).
Infant Feeding Information Related to Early Mother’s Own Milk Exposure and Percent Cumulative Nutritional Intake, N = 200.
For early exposure, all infants were included in analysis. For total NICU course, infants who died after 7 days of life and before 36 weeks corrected age (N = 9) were excluded.
MOM, mother’s own milk; PDHM, pasteurized donor human milk; SD, standard deviation.
Infant feeding dose response of nutrition type during hospitalization on BPD severity
To evaluate the feeding dose response of nutrition type on BPD severity, primary risk factors were examined via two linear regressions, one for % MOM over hospitalization and one for % PDHM over hospitalization. This analysis included gestational age, gender, and % PDHM and % MOM respectively, with BPD dichotomized as no BPD or mild to severe BPD. Birthweight was excluded due to multicollinearity with gestational age and due to greater clinical utility of gestational age in counseling patients on risk. As gestational age increased, infants have lower odds of developing BPD (OR = 0.91, 95% CI = 0.89–0.92, p < 0.001), controlling for sex and MOM. Compared to girls, boys were more likely to develop BPD (OR = 0.86, 95% CI = 0.77–0.96, p < 0.01), controlling for age and MOM. Notably, the main effect of MOM on BPD was not significant (OR = 1.00, 95% CI = 1.0–1.01, p = 0.14), controlling for gestational age and gender. Similarly, the main effect of donor milk on BPD was also not significant (OR = 1.00, 95% CI = 0.99–1.01, p = 0.09).
The moderating effect of nutrition type on relationship between gestational age and BPD
Subsequently, a moderation analysis was conducted to examine whether nutrition type moderated the association between gestational age and BPD, as we had hypothesized that MOM would have greater impact for smaller gestation infants. The percent of the various feeding types associated with the incidence of BPD risk and severity is shown in Figure 1. Infants with severe BPD were more likely to be fed less MOM and greater PDHM with 17% a combination of PDHM and MOM as well as 17% who never received feedings.
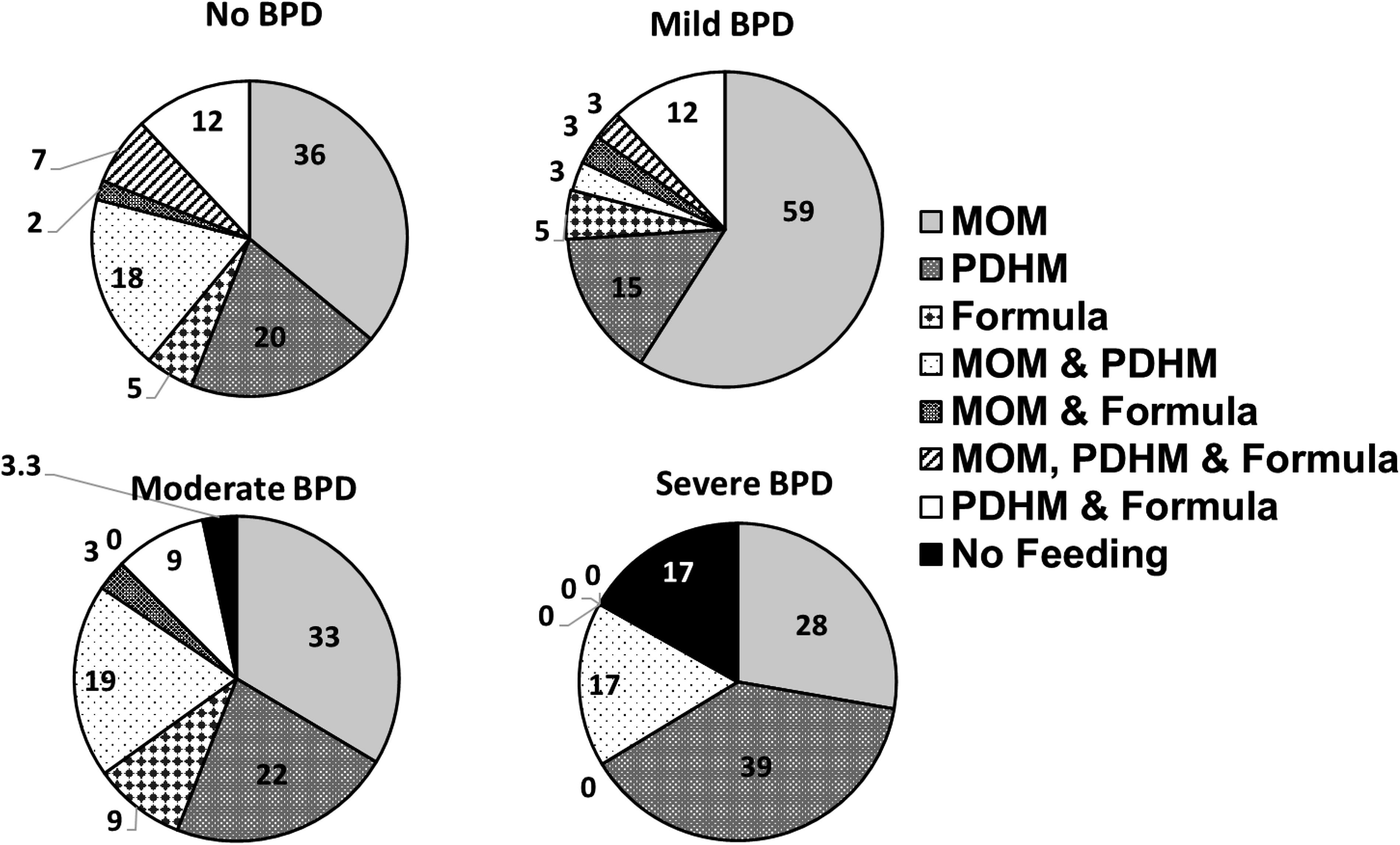
Percent of feeding type and incidence of BPD risk and severity. N = 191. BPD, bronchopulmonary dysplasia.
The percent volume of MOM received throughout hospitalization was a significant negative moderator for later development of moderate/severe BPD (p = 0.01, 95% CI [−0.13, −0.01]), such that as the percent of MOM received increases, the effect of gestational age on moderate/severe BPD decreases. In contrast, the percent of PDHM received throughout hospitalization was not found to be a significant moderator of the incidence of moderate/severe BPD (p = 0.61, 95% CI [2.31, 3.42]) (Figure 2).

Percent of MOM or PDHM feeding volume during hospitalization and moderation of the effect of gestational age on the severity of BPD. BPD, bronchopulmonary dysplasia; MOM, mother’s own milk; PDHM, pasteurized donor human milk.
Timing of exposure of MOM on BPD severity
There were 191 surviving infants to 36 weeks corrected included in the longitudinal analysis of which 128 infants received MOM, 49 infants received PDHM and 7 infants received initial PDHM then MOM during the first week of life (Table 3). There were seven infants who received no feedings during the first week of life. Infant birthweights were not significantly different among those infants exposed to MOM or PDHM in the first 3 days compared to those who received MOM, PDHM, or mixed feedings within the first week (inclusive of days 1–7) (Table 3). Infants exposed to MOM within the first 3 days compared to those with exposure within the first week (inclusive of days 1–7) had lower incidences of moderate to severe BPD when compared to those with no MOM exposure (p = 0.02, p = 0.04) (Figure 3).
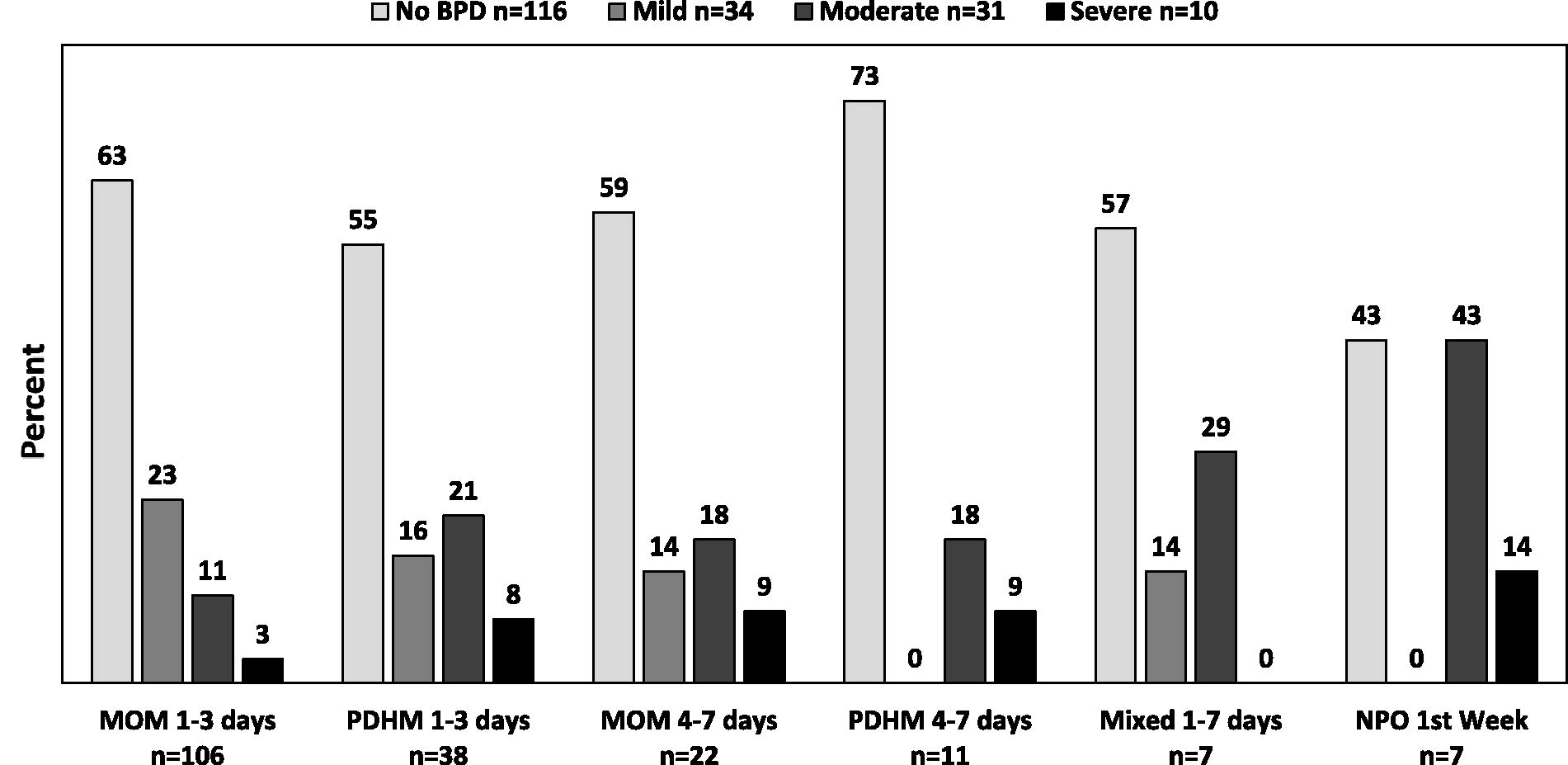
Timing of Feeding Exposure and incidence of BPD occurrence and severity. N = 191. BPD, bronchopulmonary dysplasia.
Discussion
BPD remains a significant pulmonary disease complication of preterm VLBW infants associated with high mortality and morbidity.3,4 Enteral feeding, and specifically MOM, may mitigate the severity of BPD. 5 There has been controversy related to the associated influence of PDHM as an alternative contributor to MOM as a method to mitigate the severity of BPD. 19 PDHM is often used within the first few days of life to serve as a bridge to MOM, with limited information on the influence of early first feedings using PDHM on BPD risk and severity.
The present study identifies the importance of early exposure, within the first week of life, of MOM. Our results identify that earlier exposure to MOM is associated with decreased rates of moderate to severe BPD in preterm VLBW infants, while earlier exposure to PDHM was not associated with lower rates of BPD. Of note, our study found no differences in birthweight or gestational age in infants with and without MOM in the first week, which reduces likelihood that these effects on BPD are attributable to differences in infant size. Despite the retrospective nature of this study, the high rate of infants with moderate and severe BPD suggests that MOM may be the preferred early nutrition, especially during the first weeks of life of the VLBW infant at risk for BPD. Our study limitations included the retrospective nature of the study including possible inaccurate or missing information inherent in this design. However, in our NICU, all premature infants were prospectively tracked for quality control assessment with targeted collection of feeding type and duration during the hospitalization as well as hospitalization morbidities including oxygen, ventilator use, and diagnosis of BPD and enteral feeding at discharge. Thus, we feel confident that we have fully captured the population of interest with accurate details to assess the comprehensive chart review and the findings identified.
Importantly, although the association of gestational immaturity overshadowed the influence of nutrition type (percentage of MOM or percentage PDHM throughout NICU course) on risk for BPD, the inclusion of moderation analyses identified that the percentage of MOM was associated with decreasing BPD severity among the youngest gestational age infants. This finding was not the case for PDHM, which did not influence BPD severity. These moderation effects demonstrate that nutrition type may be a modifiable risk factor that could mitigate some of the risk conferred by more established, but less easily modified, risk factors such as gestational age. The results underscore two findings: a potential critical intervention window to provide MOM ideally during the first few days of life, as well as the significant impact of continued utilization of MOM. Furthermore, the present study’s finding that MOM reduces the impact of the development of BPD has implications for counseling families, particularly those of extremely premature infants on the benefits of MOM as compared to PDHM.
Our results are in keeping with Zhu et al. 20 where timing of mother’s milk was associated with BPD risk. Our results identify a lack of influence of PDHM on mitigating BPD severity. The finding that PDHM did not attenuate the risk of gestational age on BPD severity is in contrast to Merino-Hernandez et al who identified that PDHM compared to MOM had a similar BPD protective impact in preterm infants. 21 Furthermore, in contrast to Villamor-Martinez, 22 in this population of 200 VLBW infants with a BPD rate of 42%, specific components attributed to MOM were associated with mitigation of BPD suggesting that components may be present in greater quantities than PDHM that are important to the BPD protective mechanism. The results also suggest and stress the importance of consideration of early MOM nutrition as the preferred first line of enteral feeding exposure as a form of critical medicine in the care of the VLBW infant that appears to be important to change the trajectory of lung disease to support healthy lung development in the premature infant.
Conclusion
This study supports well-known findings regarding the importance of MOM as the optimal nutritional support for the infant. Strategies that lead to early exposure and sustained support of MOM nutritional attainment can have an important positive influence on the trajectory of BPD and its severity in the VLBW preterm infant. For those infants who may not have the benefit of MOM, additional research is needed to identify the important human milk compositional characteristics that are beneficial in BPD reduction severity to provide access and opportunities for an individualized therapeutic approach to care in these at-risk infants.
Footnotes
Authors’ Contributions
K.D.H.-M. and J.V.: were responsible for the study concept, intellectual concept, and original study design. K.D.H.-M., A.S., N.C., J.X., and J.V.: were responsible for study design refinement and methodology. A.W., A.S., N.C., L.C., D.C., and J.X.: were responsible for data curation. K.D.H.-M., A.W., L.C., and D.C.: were responsible for statistical analysis. K.D.H.-M., A.W., L.C., D.C., and J.X.: were responsible for interpretation of the data. K.D.H.-M., A.W., L.C., N.C., D.C., and J.X.: were responsible for drafting and article preparation. All authors contributed to article reviewing, revision, and editing.
Disclosure Statement
The authors report no disclosures or conflicts of interest.
Funding Information
Support for this work has been provided in part through a grant from The Gerber Foundation (KDHM). The Gerber Foundation is a separately endowed, private, 501(c)(3) foundation not related to Gerber Products Company in any way. Support for this work was also supported through the Division of Neonatal Medicine JACK’s Summer Scholar Fund.